

The Value of Myocardium and Kidney Histopathological and Immunohistochemical Findings in Accidental Hypothermia-Related Fatalities
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographical Characteristics and Medico-Legal Findings
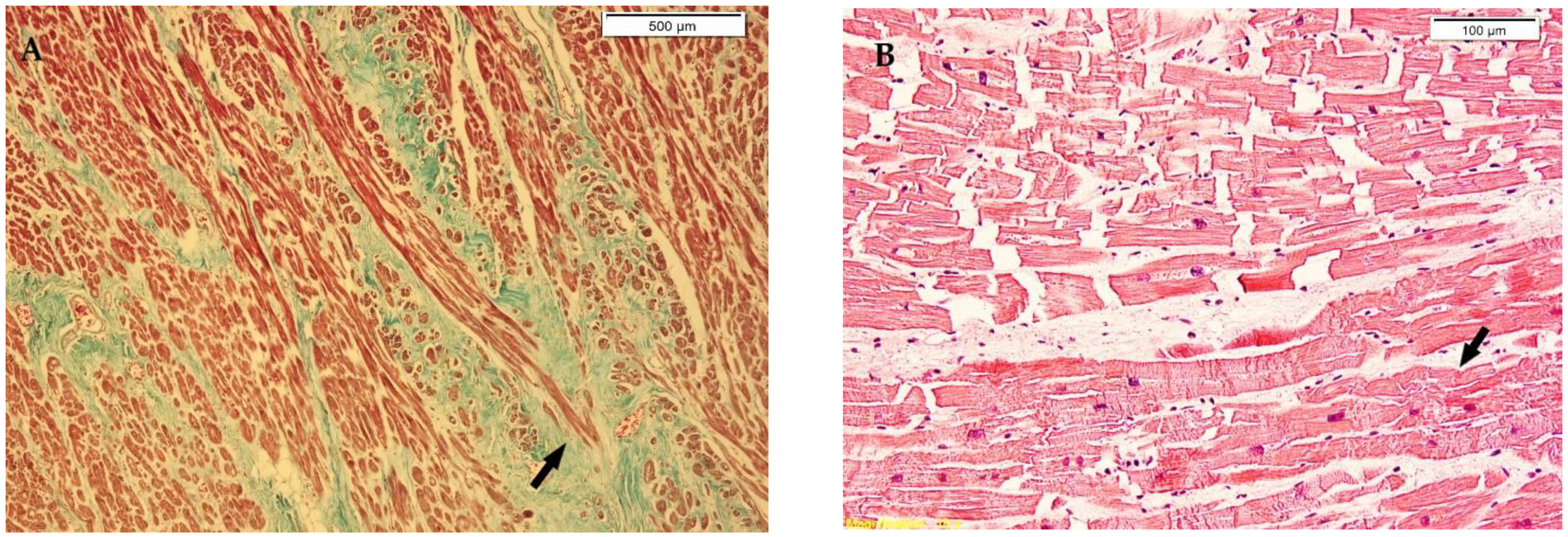
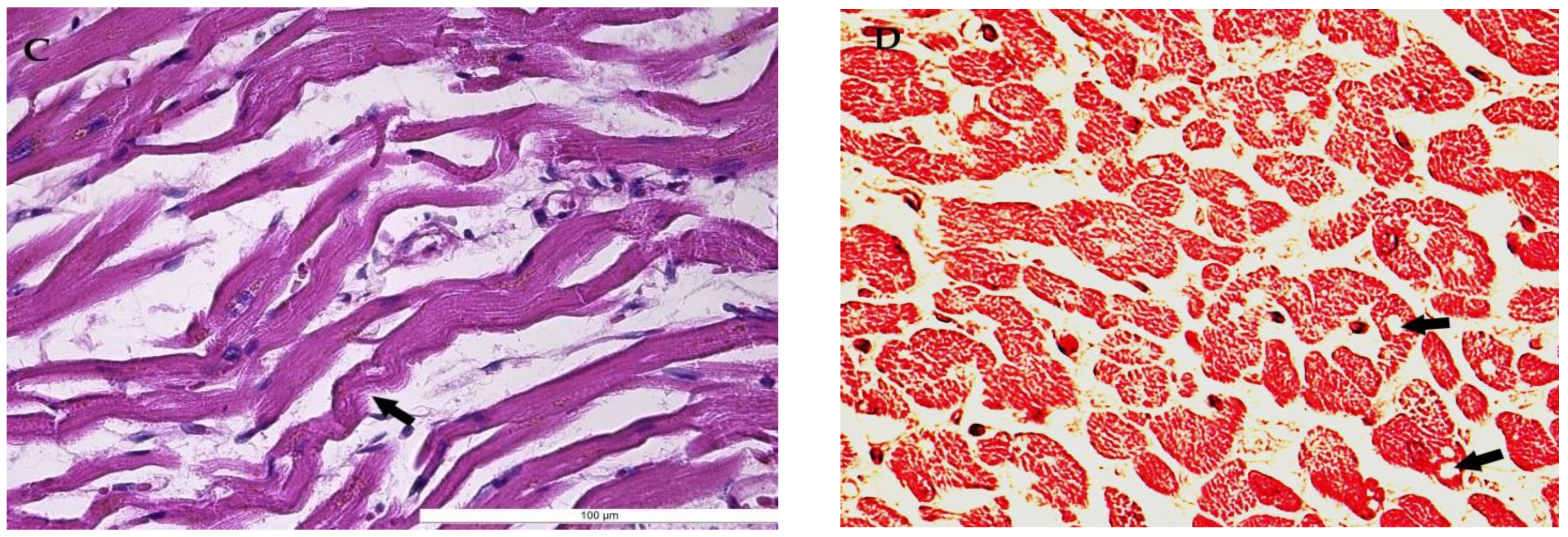
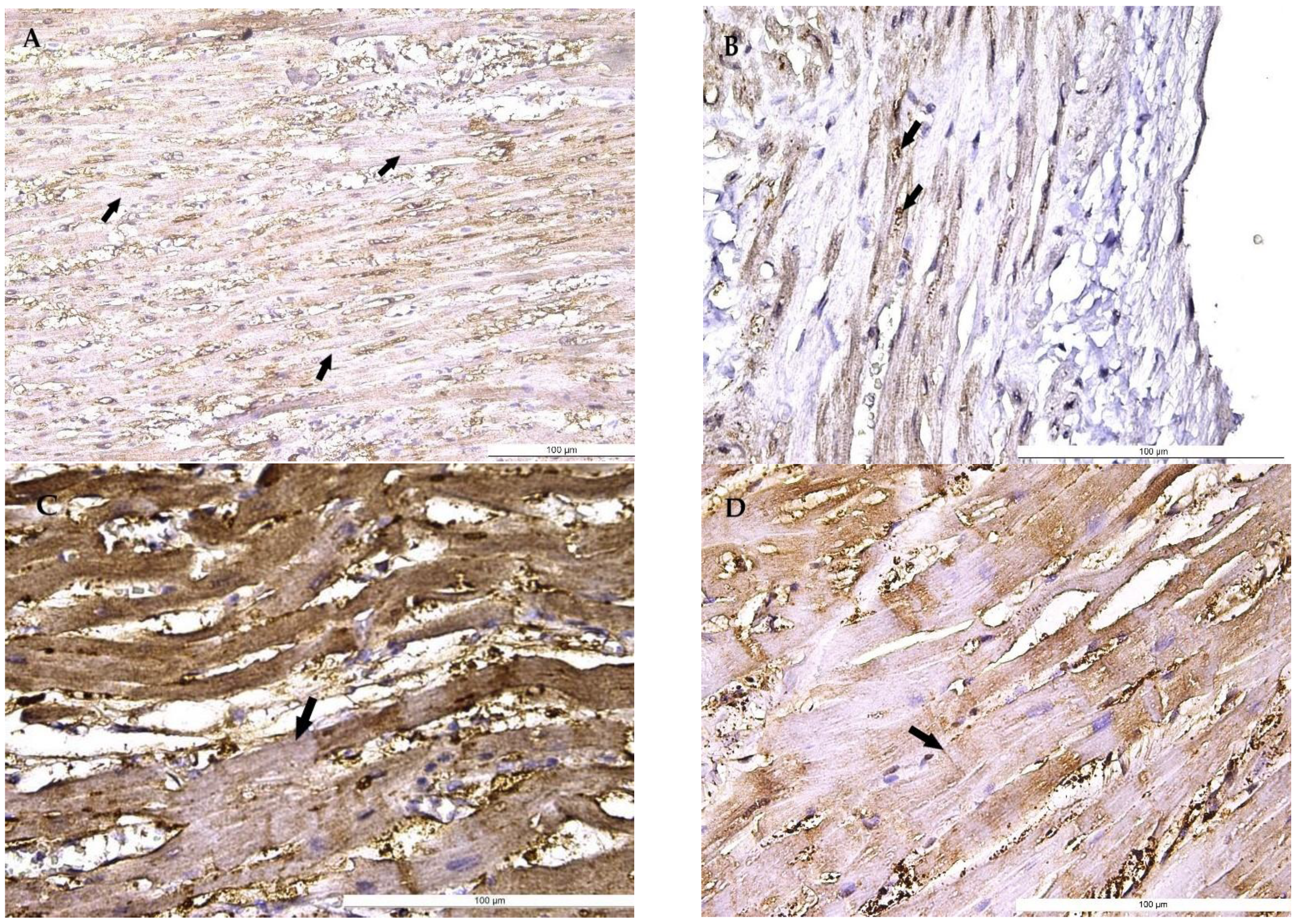
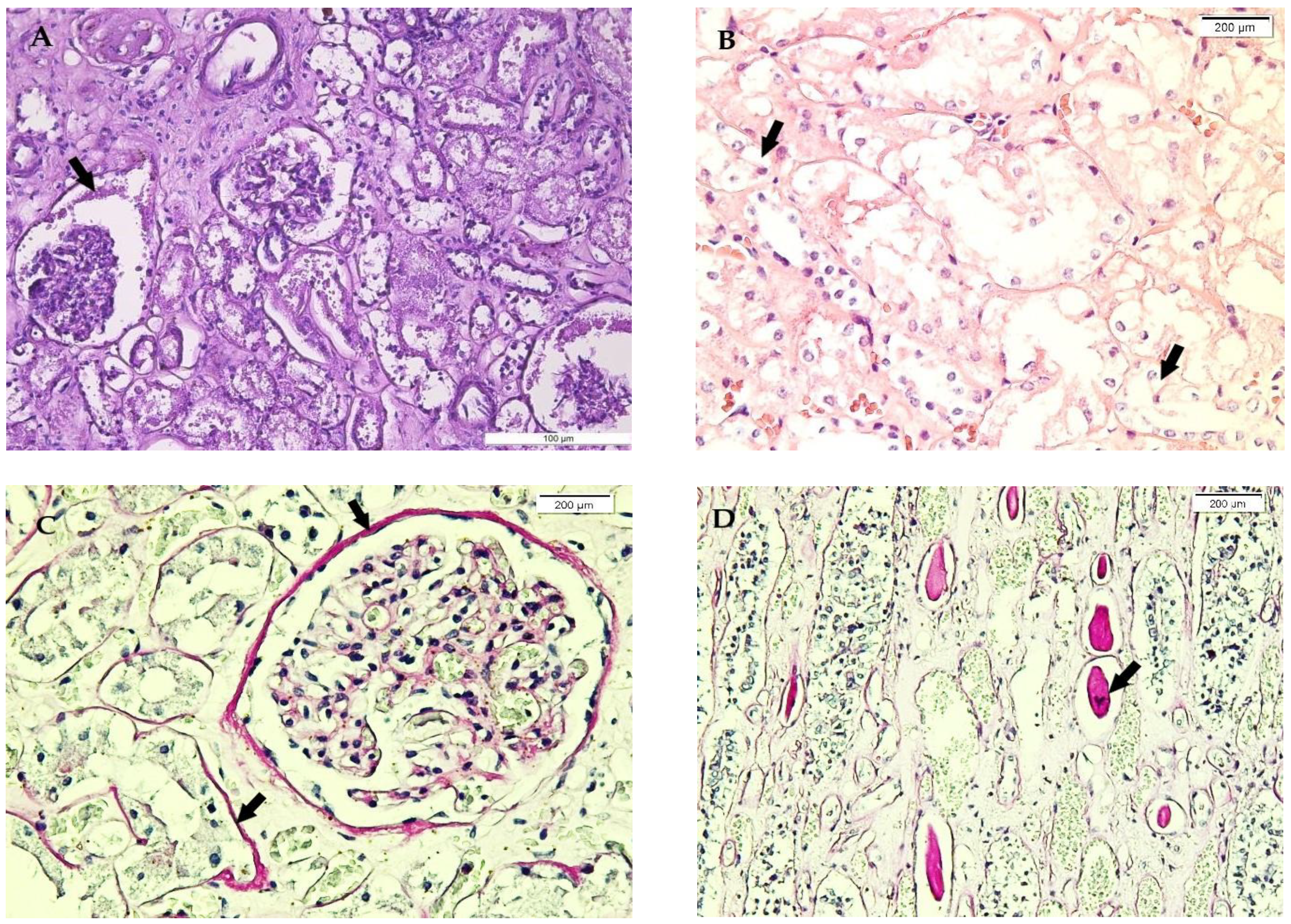
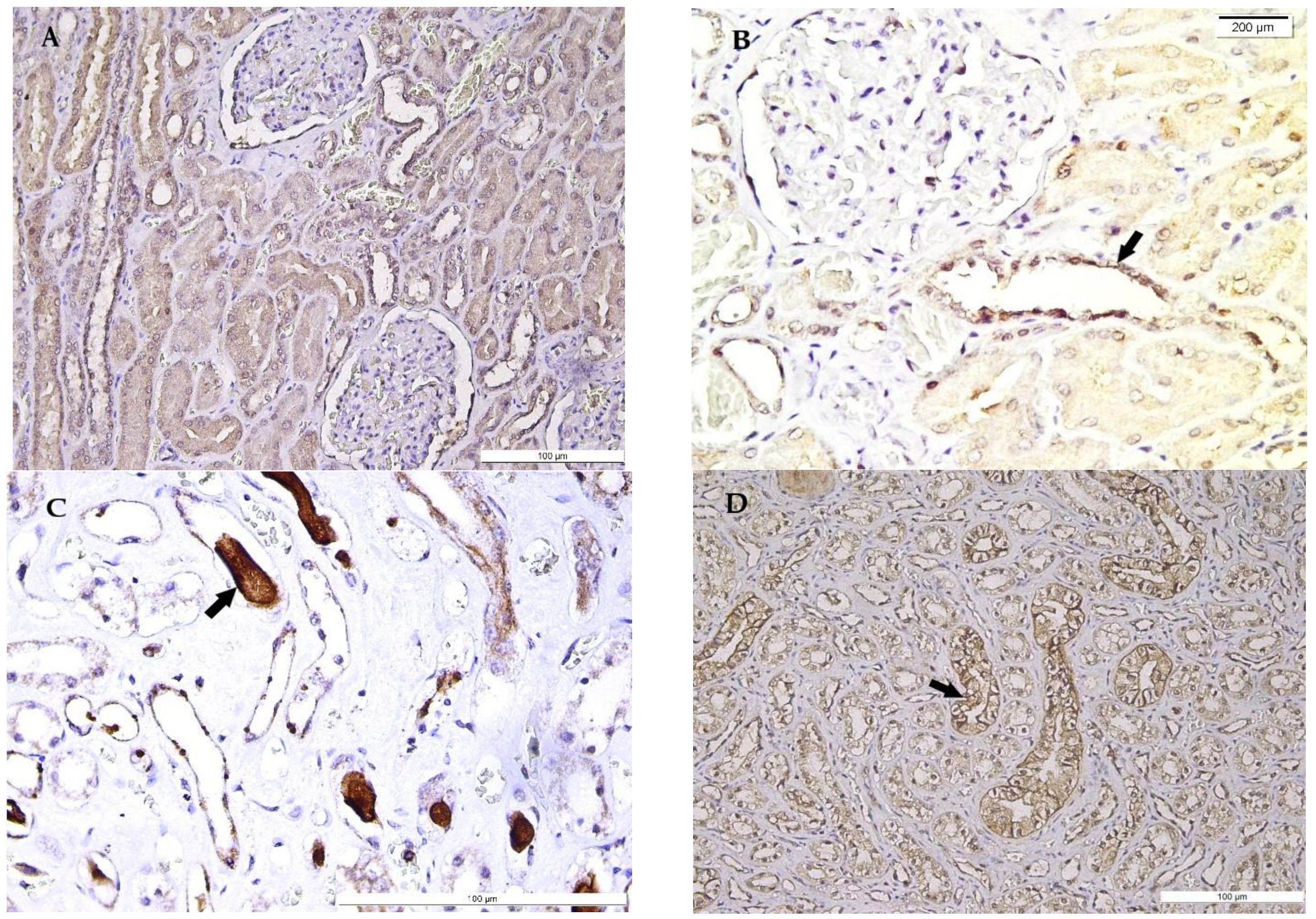
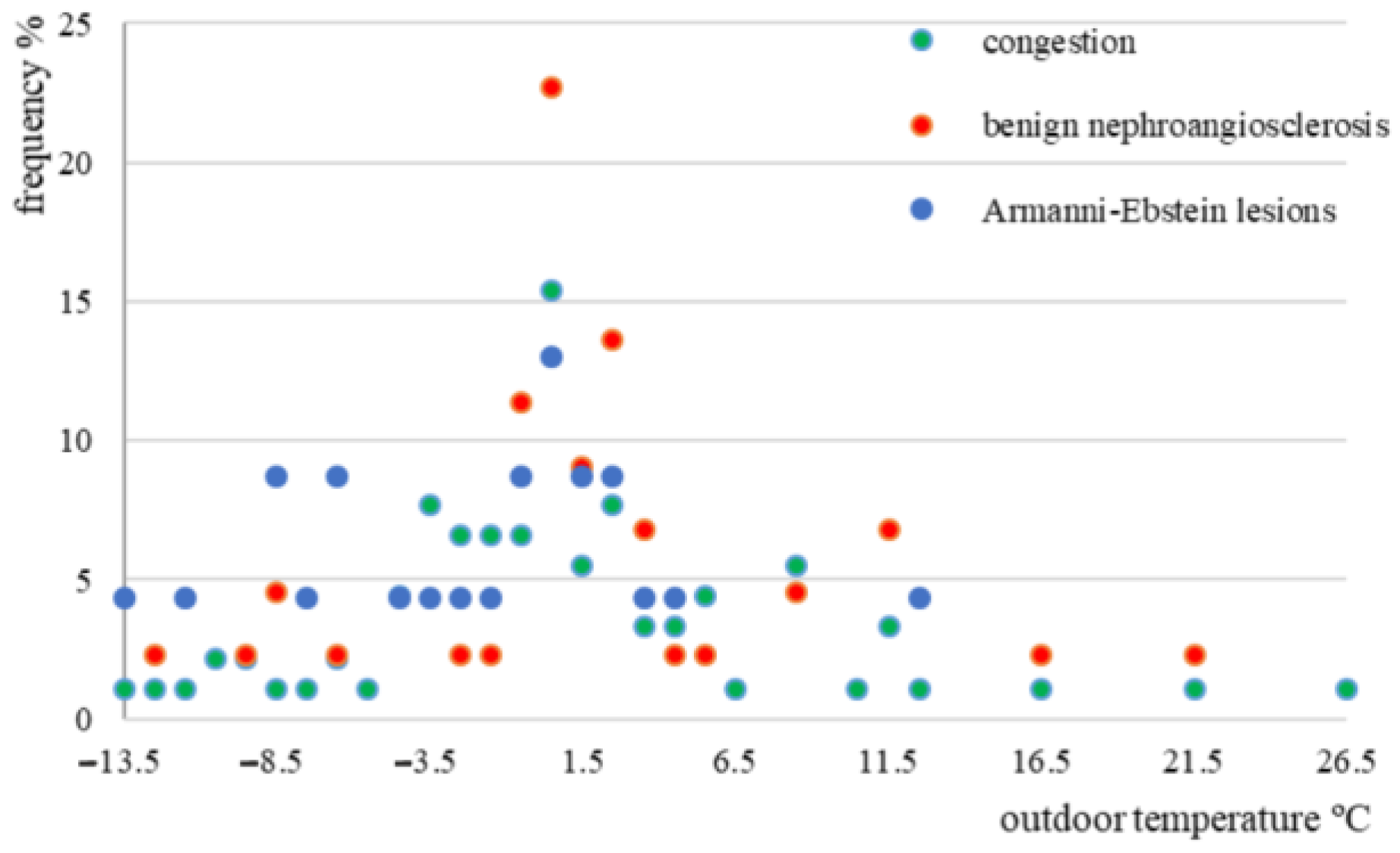
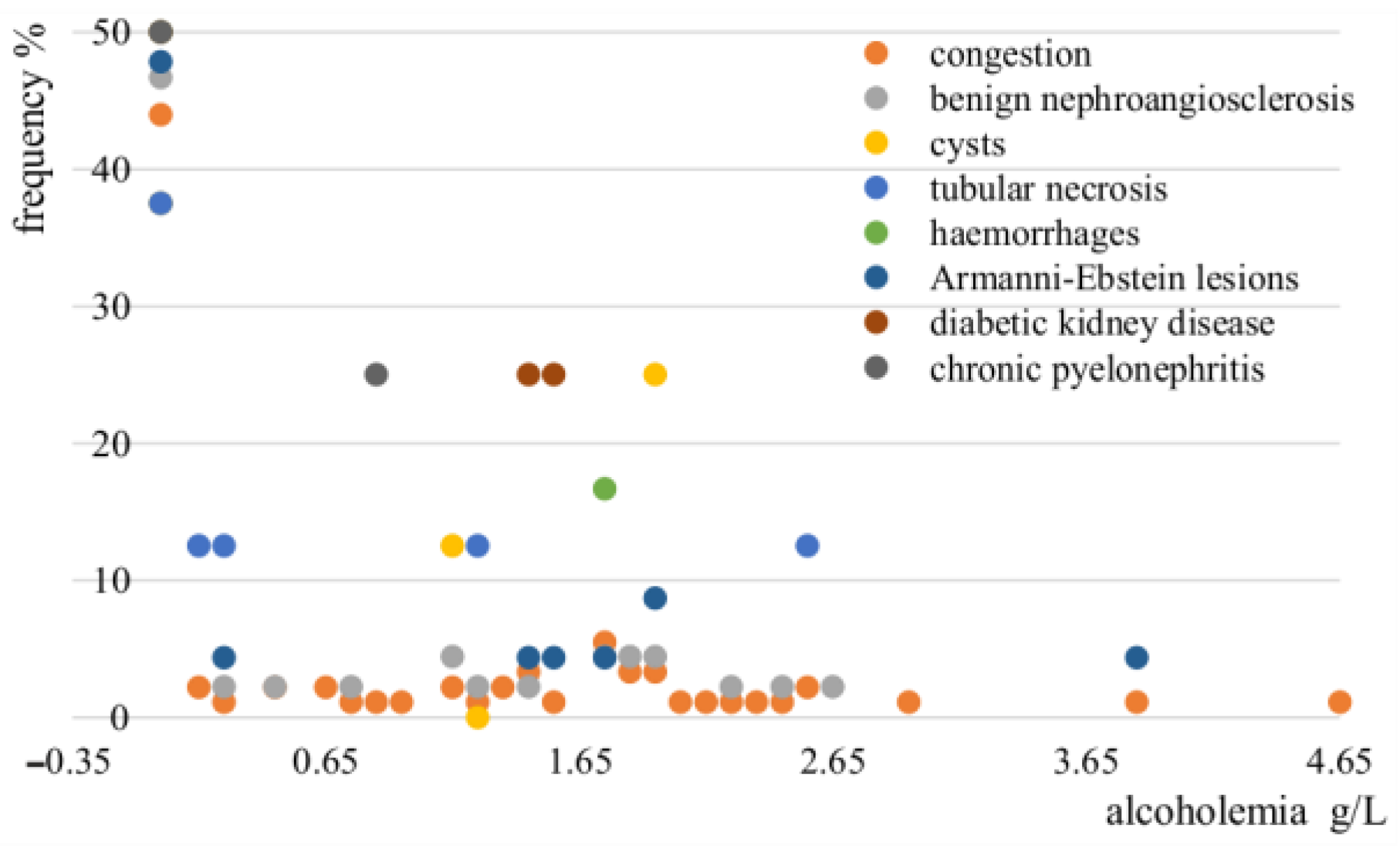
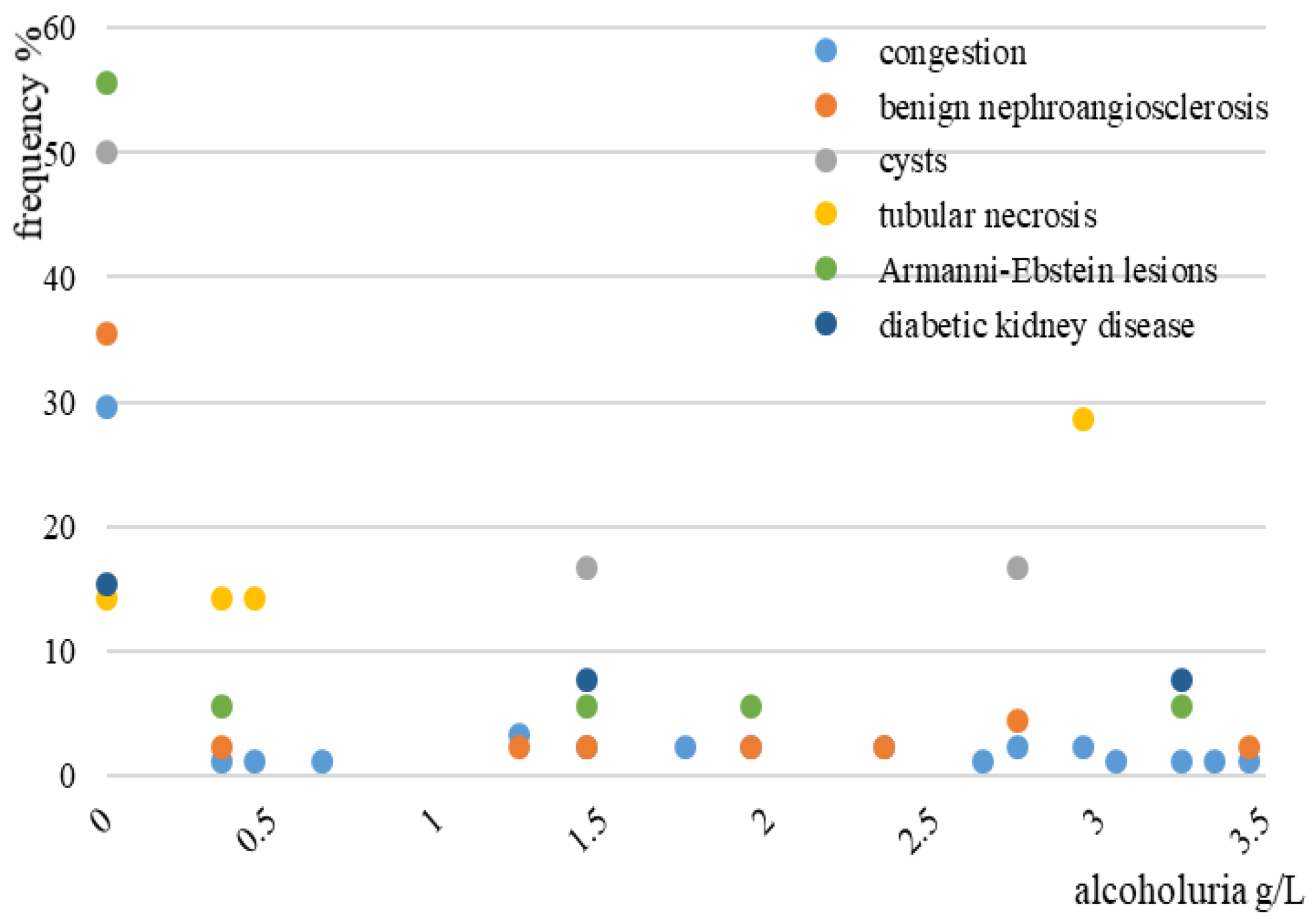
3.2. Myocardium and Renal Histopathological and Immunohistochemical Findings
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palmiere, C.; Mangin, P. Hyperthermia and postmortem biochemical investigations. Int. J. Leg. Med. 2012, 127, 93–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.A.; Mohammed, S.S.; Tammam, H.G.; Abdel-Karim, R.I.; Farag, M.M. Histopathological, histochemical and biochemical postmortem changes in induced fatal hypothermia in rats. Forensic Sci. Res. 2021, 7, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Sacco, M.A.; Abenavoli, L.; Juan, C.; Ricci, P.; Aquila, I. Biological mechanisms behind wischnewsky spots finding on gastric mucosa: Autopsy cases and literature review. Int. J. Environ. Res. Public Health 2022, 19, 3601. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Bright, F.; Winskog, C.; Yool, A.J.; Byard, R.W. Lethal hypothermia in an animal model, not associated with basal renal epithelial vacuolization. J. Forensic Leg. Med. 2013, 21, 14–16. [Google Scholar] [CrossRef]
- Clark, K.H.; Stoppacher, R. Gastric mucosal petechial hemorrhages (wischnewsky lesions), hypothermia, and diabetic ketoacidosis. Am. J. Forensic Med. Pathol. 2016, 37, 165–169. [Google Scholar] [CrossRef]
- Ball, C.G.; Herath, J.C. Earth, air, water, and fire: Histopathology of environmental death. Acad. Forensic Pathol. 2018, 8, 641–652. [Google Scholar] [CrossRef]
- Rösli, D.; Schnüriger, B.; Candinas, D.; Haltmeier, T. The impact of accidental hypothermia on mortality in trauma patients overall and patients with traumatic brain injury specifically: A systematic review and meta-analysis. World J. Surg. 2020, 44, 4106–4117. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.; Thomsen, J.L.; Kristensen, I.B.; Ottosen, P.D. Accumulation of triglycerides in the proximal tubule of the kidney in diabetic coma. Pathology 2003, 35, 305–310. [Google Scholar] [CrossRef]
- Chavala, M.A.; Gallardo, M.A.; Martínez, S.; Bayego, E.S. Management of accidental hypothermia: A narrative review. Med. Intensiv. (Engl. Ed.) 2019, 43, 556–568. [Google Scholar] [CrossRef]
- Lott, C.; Truhlář, A.; Alfonzo, A.; Barelli, A.; González-Salvado, V.; Hinkelbein, J.; Nolan, J.; Paal, P.; Perkins, G.; Thies, K.C.; et al. European resuscitation council guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021, 161, 152–219. [Google Scholar] [CrossRef]
- Elibol, B.; Kilic, U. High levels of SIRT1 expression as a protective mechanism against disease-related conditions. Front. Endocrinol. 2018, 9, 614. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Zhang, X.; Rong, J. SUMOylation as a therapeutic target for myocardial infarction. Front. Cardiovasc. Med. 2021, 8, 701583. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Chen, X.; Liu, S. Role of sirtuin-1 in neonatal hypoxic-ischemic encephalopathy and its underlying mechanism. Med. Sci. Monit. 2020, 26, e924544-1–e924544-10. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Ishida, Y.; Ishigami, A.; Nosaka, M.; Kuninaka, Y.; Hata, S.; Yamamoto, H.; Hashizume, Y.; Matsuki, J.; Yasuda, H.; et al. Forensic application of epidermal ubiquitin expression to determination of wound vitality in human compressed neck skin. Front. Med. 2022, 9, 867365. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Xiao, P.; Cui, H.; Gong, P.; Lin, C.; Chen, F.; Tang, Z. Hypothermia-induced ubiquitination of voltage-dependent anion channel 3 protects BV2 microglia cells from cytotoxicity following oxygen-glucose deprivation/recovery. Front. Mol. Neurosci. 2020, 13, 100. [Google Scholar] [CrossRef] [PubMed]
- Boiculese, L.V.; Dimitriu, G.; Moscalu, M. Nearest neighbor classification with improved weighted dissimilarity measure. Proc. Rom. Acad. Ser. A-Math. Phys. Tech. Sci. Inf. Sci. 2009, 10, 205–213. [Google Scholar]
- Cardillo, G. MyFisher: The Definitive Function for the Fisher’s Exact and Conditional Test for Any RxC Matrix, MyFisher. Available online: https://github.com/dnafinder/myfisher (accessed on 16 July 2022).
- Nixdorf-Miller, A.; Hunsaker, D.M.; Hunsaker, J.C., 3rd. Hypothermia and hyperthermia medicolegal investigation of morbidity and mortality from exposure to environmental temperature extremes. Arch. Pathol. Lab. Med. 2006, 130, 1297–1304. [Google Scholar] [CrossRef]
- Revised Wind Chill Index Charts. National Weather Service. National Oceanic & Atmospheric Administration, US Department of Commerce. Available online: http://www.infoplease.com/ipa/A0001374.html?mail-11–22 (accessed on 2 August 2022).
- Paal, P.; Pasquier, M.; Darocha, T.; Lechner, R.; Kosinski, S.; Wallner, B.; Zafren, K.; Brugger, H. Accidental hypothermia: 2021 update. Int. J. Environ. Res. Public Health 2022, 19, 501. [Google Scholar] [CrossRef]
- Zafren, K.; Atkins, D.; Brugger, H. Reported resuscitation of a hypothermic avalanche victim with assisted ventilation in 1939. Wilderness Environ. Med. 2018, 29, 275–277. [Google Scholar] [CrossRef]
- Descloux, E.; Ducrot, K.; Scarpelli, M.P.; Lobrinus, A.; Palmiere, C. Paradoxical undressing associated with subarachnoid hemorrhage in a non-hypothermia case? Int. J. Leg. Med. 2017, 131, 1341–1345. [Google Scholar] [CrossRef]
- Ishikawa, T.; Quan, L.; Li, D.-R.; Zhao, D.; Michiue, T.; Hamel, M.; Maeda, H. Postmortem biochemistry and immunohistochemistry of adrenocorticotropic hormone with special regard to fatal hypothermia. Forensic Sci. Int. 2008, 179, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Preuß, J.; Dettmeyer, R.; Lignitz, E.; Madea, B. Fatty degeneration of myocardial cells as a sign of death due to hypothermia versus degenerative deposition of lipofuscin. Forensic Sci. Int. 2006, 159, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Wingenfeld, L.; Sakaguchi, I.; Nakagawa, T.; Takaya, A.; Morita, S.; Yamasaki, S.; Nishi, K. Histopathological characteristics of human cardiac tissues in accidental hypothermia using conventional staining techniques. Romanian J. Leg. Med. 2012, 20, 241–246. [Google Scholar] [CrossRef]
- Elshama, S.S.; Osman, H.E.H.; El-Kenawy, A.E.M. Postmortem diagnosis of induced fatal hypothermia in adult albino rats. Rom. J. Leg. Med. 2016, 24, 106–114. [Google Scholar]
- Curca, G.C.; Dermengiu, D.; Ceausu, M.; Francisc, A.; Rusu, M.C.; Hostiuc, S. Cardiac lesions associated with cardiopulmonary resuscitation. Rom. J. Leg. Med. 2011, 19, 1–6. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, Q.; Lu, Y.; Wan, J.; Dai, H.; Zhou, X.; Lv, S.; Chen, X.; Zhang, X.; Hang, C.; et al. Cerebroprotection by salvianolic acid B after experimental subarachnoid hemorrhage occurs via Nrf2- and SIRT1-dependent pathways. Free Radic. Biol. Med. 2018, 124, 504–516. [Google Scholar] [CrossRef]
- Yang, H.-Y.; Chen, J.-Y.; Huo, Y.-N.; Yu, P.-L.; Lin, P.-Z.; Hsu, S.-C.; Huang, S.-M.; Tsai, C.-S.; Lin, C.-Y. The role of sirtuin 1 in palmitic acid-induced endoplasmic reticulum stress in cardiac myoblasts. Life 2022, 12, 182. [Google Scholar] [CrossRef]
- Morita, S.; Furukawa, S.; Nishi, K. Classification of contraction bands using immunohistochemistry. Am. J. Forensic Med. Pathol. 2015, 36, 23–26. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Byard, R.W. Armanni-Ebstein phenomenon and hypothermia. Forensic Sci. Int. 2011, 206, e82–e84. [Google Scholar] [CrossRef]
- Doberentz, E.; Markwerth, P.; Madea, B. Fatty degeneration in renal tissue in cases of fatal accidental hypothermia. Romanian J. Leg. Med. 2017, 25, 152–157. [Google Scholar] [CrossRef]
- Natanti, A.; Mazzanti, R.; Palpacelli, M.; Turchi, C.; Tagliabracci, A.; Pesaresi, M. Death following extreme temperature exposure: Histological, biochemical and immunohistochemical markers. Med. Sci. Law 2021, 61, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Zhu, B.-L.; Li, D.-R.; Zhao, D.; Michiue, T.; Maeda, H. Immunohistochemical investigation of ubiquitin and myoglobin in the kidney in medicolegal autopsy cases. Forensic Sci. Int. 2007, 171, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Fineschi, V.; D’Errico, S.; Neri, M.; Panarese, F.; Ricci, P.A.; Turillazzi, E. Heat stroke in an incubator: An immunohistochemical study in a fatal case. Int. J. Legal. Med. 2004, 119, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Quan, L.; Ishikawa, T.; Michiue, T.; Li, D.-R.; Zhao, D.; Zhu, B.-L.; Maeda, H. Quantitative analysis of ubiquitin-immunoreactivity in the midbrain periaqueductal gray matter with regard to the causes of death in forensic autopsy. Leg. Med. 2005, 7, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Ohtani, S.; Shiono, H.; Fukusima, T.; Sasaki, M. Expression of ubiquitin protein in each organ at death from hypothermia. Forensic Sci. Int. 1997, 86, 61–68. [Google Scholar] [CrossRef]
- Brändström, H.; Eriksson, A.; Giesbrecht, G.; Ängquist, K.-A.; Haney, M. Fatal hypothermia: An analysis from a sub-arctic region. Int. J. Circumpolar Health 2012, 71, 18502. [Google Scholar] [CrossRef]
- Yousef, H.; Ahangar, E.R.; Varacallo, M. Physiology, thermal regulation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Tipton, M.J.; Collier, N.; Massey, H.; Corbett, J.; Harper, M. Cold water immersion: Kill or cure? Exp. Physiol. 2017, 102, 1335–1355. [Google Scholar] [CrossRef] [Green Version]
- Knechtle, B.; Waśkiewicz, Z.; Sousa, C.V.; Hill, L.; Nikolaidis, P.T. Cold water swimming—Benefits and risks: A narrative review. Int. J. Environ. Res. Public Health 2020, 17, 8984. [Google Scholar] [CrossRef]
- Lankford, H.V.; Fox, L.R. The wind-chill index. Wilderness Environ. Med. 2021, 32, 392–399. [Google Scholar] [CrossRef]
- Szota, A.M.; Araszkiewicz, A.S. The risk factors, frequency and diagnosis of atypical antipsychotic drug-induced hypothermia: Practical advice for doctors. Int. Clin. Psychopharmacol 2019, 34, 1–8. [Google Scholar] [CrossRef]
- Zonnenberg, C.; Bueno-De-Mesquita, J.M.; Ramlal, D.; Blom, J.D. Antipsychotic-related hypothermia: Five new cases. Front. Psychiatry 2019, 10, 543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burk, B.G.; Ward, A.H.; Clark, B. A case report of acute hypothermia during initial inpatient clozapine titration with review of current literature on clozapine-induced temperature dysregulations. BMC Psychiatry 2020, 20, 290. [Google Scholar] [CrossRef] [PubMed]
- Berube, M.W.; Lemmon, M.E.; Pizoli, C.E.; Bidegain, M.; Tolia, V.N.; Cotten, C.M.; Greenberg, R.G. Opioid and benzodiazepine use during therapeutic hypothermia in encephalopathic neonates. J. Perinatol. 2019, 40, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, A.C.; Quraishi, I.H.; Mattson, R.H. Hypothermia associated with clobazam use in adult epilepsy. Epilepsy Behav. Rep. 2016, 5, 17–18. [Google Scholar] [CrossRef] [Green Version]
- Griffin, C.E., 3rd; Kaye, A.M.; Bueno, F.R.; Kaye, A.D. Benzodiazepine pharmacology and central nervous system-mediated effects. Ochsner J. 2013, 13, 214–223. [Google Scholar]
- DiFazio, M.P.; Lavenstein, B.; Demarest, S. Profound hypothermia secondary to clobazam use in epilepsy: A novel association. Neurosci. Med. 2014, 5, 15–19. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Death Area | Total % | Male % | Female % | p-Value * | Urban % | Rural % | p-Value * |
|---|---|---|---|---|---|---|---|
| Non-built-up areas | 23 | 19.6 | 1.9 | <0.01 | 4.7 | 16.8 | <0.01 |
| Hospital | 30 | 22.4 | 5.6 | <0.01 | 10.3 | 17.8 | <0.01 |
| Domicile | 32 | 19.6 | 10.3 | 0.02 | 7.5 | 22.4 | <0.01 |
| Public spaces | 22 | 14 | 6.5 | <0.01 | 9.3 | 11.2 | 0.03 |
| Patients’ Characteristics | No. Cases (%) (n = 107) | Mean ± SD | p-Value | |
|---|---|---|---|---|
| Gender | ||||
| Female | 26 (24%) | - | 0.634 # | |
| Male | 81 (76%) | - | ||
| Mean age (years) | 57.95 ± 1.47 | |||
| Female | 26 (24%) | 62.5 ± 13.65 | 0.085 * | |
| Male | 81 (74.8%) | 56.5 ± 15.8 | ||
| Environment | ||||
| Urban | 34 (31.8%) | - | 0.566 # | |
| Rural | 73 (68.2%) | - | ||
| Mean ambient temperature (°C/°F) | - | 0.57 ± 6.4 °C/33 ± 11.5 °F | - | |
| Mean wind speed (km/h) | - | 2.28 ± 3.3 | - | |
| Air humidity index | - | 0.74 ± 0.23 | - | |
| Wind chill index ** | - | 5.83 ± 8.9 | - | |
| Clothing | ||||
| Paradoxical undressing Female/Male | 10 (9.3%) 3/7 (2.8%/6.5%) | - | 0.061 # | |
| Fully clothed Female/Male | 97 (90.6%) 23/74 (21.5%/69.2%) | - | 0.015 # | |
| Comorbidities | ||||
| Alcoholism Female/Male | 54 (50.5%) 14/40 (13.1%/37.4%) | - | 0.021 # | |
| Neuro-psychiatric diseases Female/Male | 11 (10.3%) 4/7 (3.7%/6.5%) | - | 0.034 # | |
| Diabetes mellitus Female/Male | 4 (3.7%) 2/2 (1.9%/1.9%) | - | 0.892 # | |
| Total/partial gastrectomy Male | 3 (2.8%) 3 (2.8%) | - | - | |
| Lung tuberculosis Female/Male | 5 (4.7%) 2/3(1.9%/2.8%) | - | 0.048 # | |
| Miscellaneous Female/Male | 7 (6.5%) 1/6 (0.9%/5.6%) | - | 0.037 # | |
| Without known comorbidities Female/Male | 39 (36.4%) 9/30 (8.4%/28%) | - | 0.026 # | |
| Alcoholemia | ||||
| Negative Female/Male | 62 (57.9%) 18/44 (16.8%/41.1%) | - | 0.031 # | |
| Positive Female/Male | 45 (42%) 13/38 (12.1%/35.5%) # | 1.67 ± 1.04 g/L 1.71 ± 0.95 g/L/1.52 ± 0.73 g/L * | 0.024 # | 0.545 * |
| Alcoholuria | ||||
| Negative Female/Male | 81 (75.7%) 21/60 (19.6%/56.1%) | - | 0.001 # | |
| Positive Female/Male | 26 (24.3%) 8/18 (7.5%/16.8%) # | 2.14 ± 1.22 g/L 1.96 ± 1.05 g/L/2.18 ± 0.93 g/L * | 0.028 # | 0.642 * |
| Toxicology | ||||
| Negative | 42 (39.2%) | - | ||
| Positive | 3 (2.8%) | - | ||
| Organ | Gross Findings | No. of Cases n, (%); (nF; nM) * | Microscopy | No. of Cases n, (%); (nF; nM) | p-Value |
|---|---|---|---|---|---|
| Heart | Atherosclerosis | 65 (60.7%); (17 F; 48 M) | Coronary fibrous cap atheroma | 52 (48.6%); (15 F; 37 M) | 0.015 |
| Cardiac fibrosis | 40 (37.4%); (8 F; 32 M) | Ischemic myocardial fibrosis | 73 (68.2%); (21 F; 52 M) | 0.001 | |
| Cardiac hypertrophy | 25 (23.6%) (7 F; 18 M) | Cardiomyocytes hypertrophy | 20 (18.7%); (3 F; 17 M) | 0.020 | |
| Epicardial petechiae | 6 (5.6%); (1 F; 5 M) | Epicardial haemorrhages | 6 (5.6%); (2 F; 4 M) | - | |
| No evident lesions | 8 (7.5%); (1 F; 7 M) | - | |||
| Degeneration or loss of myocardial architecture | 107 (100%); (26 F; 81 M) | - | |||
| Contraction bands | 102 (95.3%); (24 F; 78 M) | - | |||
| Congestion | 92 (86%); (21 F; 71 M) | - | |||
| Cardiomyocytes vacuolisation (fatty changes) | 14 (13.1%); (3 F; 11 M) | - | |||
| Pericarditis | 2 (1.9%); (0 F; 2 M) | - | |||
| Myocarditis | 1 (0.9%); (1 F; 0 M) | - | |||
| Endocardial degenerative lesions | 1 (0.9%); (0 F; 1 M) | - | |||
| Kidneys | Stasis | 89 (83.2%) (21 F; 68 M) | Congestion | 90 (84.1%) (22 F; 69 M) | 0.001 |
| Cicatricial retractions | 19 (17.8%) (7 F; 12 M) | Benign nephroangiosclerosis | 45 (42.1%) (15 F; 30 M) | 0.001 | |
| Absent (hemicorporectomy) | 1 (0.9%) (0 F; 1 M) | - | |||
| Renal cysts | 9 (8.4%) (2 F; 7 M) | Tubular cysts | 8 (7.5%) (1 F; 7 M) | 0.003 | |
| Armanni-Ebstein lesions | 23 (21.5%) (5 F; 18 M) | - | |||
| Tubular necrosis | 8 (7.5%) (2 F; 6 M) | - | |||
| Interstitial haemorrhages | 6 (5.6%) (2 F; 4 M) | - | |||
| Diabetic kidney disease | 4 (3.7%) (2 F; 2 M) | - | |||
| Chronic pyelonephritis | 4 (3.7%) (2 F; 2 M) | - | |||
| Renal crystal deposits | 1 (0.9%) (1 M) | - | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hleșcu, A.A.; Grigoraș, A.; Covatariu, G.; Moscalu, M.; Amalinei, C. The Value of Myocardium and Kidney Histopathological and Immunohistochemical Findings in Accidental Hypothermia-Related Fatalities. Medicina 2022, 58, 1507. https://doi.org/10.3390/medicina58111507
Hleșcu AA, Grigoraș A, Covatariu G, Moscalu M, Amalinei C. The Value of Myocardium and Kidney Histopathological and Immunohistochemical Findings in Accidental Hypothermia-Related Fatalities. Medicina. 2022; 58(11):1507. https://doi.org/10.3390/medicina58111507
Chicago/Turabian StyleHleșcu, Andreea Alexandra, Adriana Grigoraș, Gabriela Covatariu, Mihaela Moscalu, and Cornelia Amalinei. 2022. "The Value of Myocardium and Kidney Histopathological and Immunohistochemical Findings in Accidental Hypothermia-Related Fatalities" Medicina 58, no. 11: 1507. https://doi.org/10.3390/medicina58111507