

Evaluation of the Safety and Efficacy of Ormeloxifene, a Selective Estrogen Receptor Modulator and Medroxyprogesterone Acetate in Women with Non-Structural Abnormal Uterine Bleeding: A Randomized Clinical Trial

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
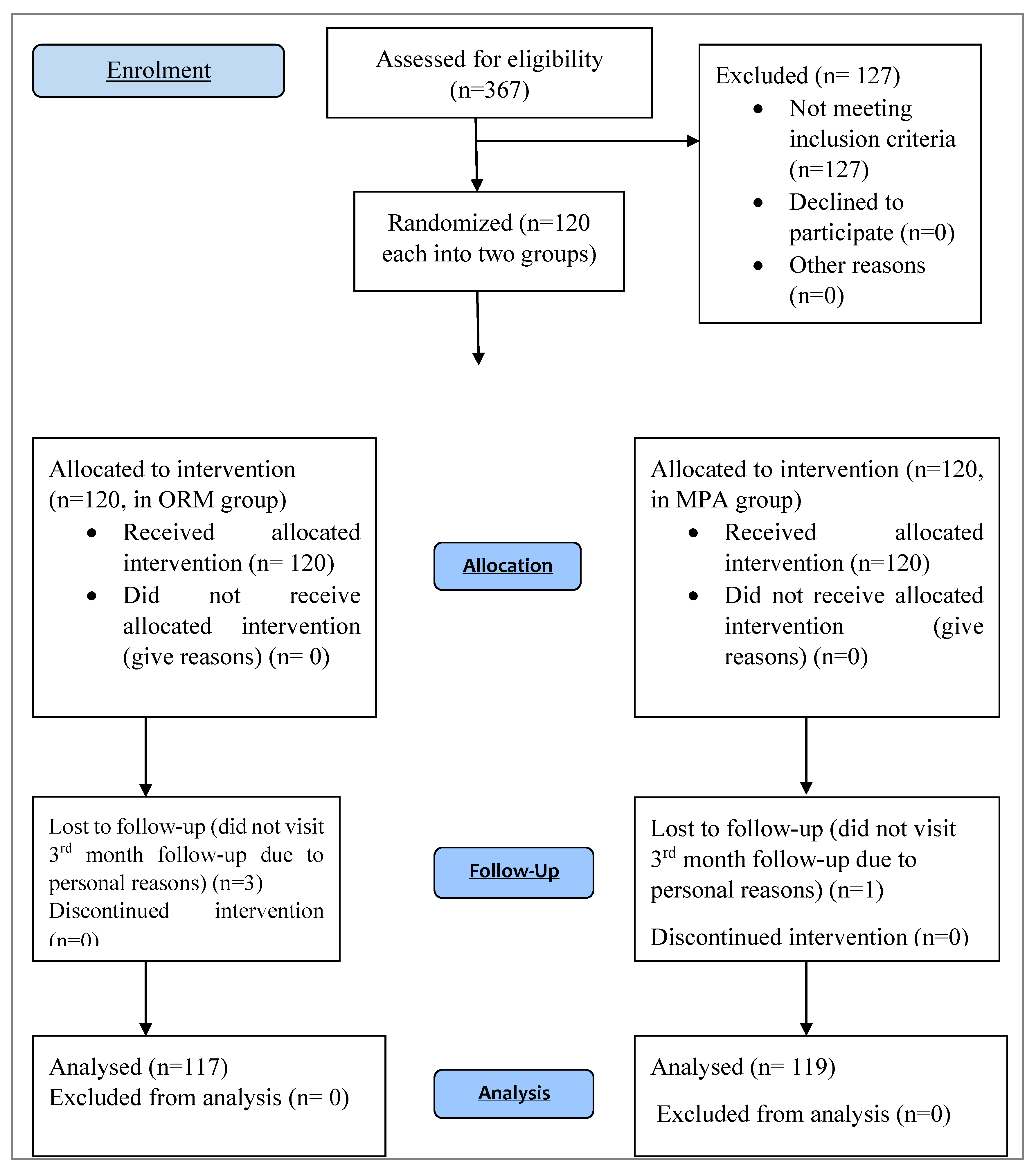
2.1. Clinical Trial
2.2. Clinical Trial Registration
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Sample Size
2.6. Study Population
2.7. Data Collection
2.8. HRQoL (SF-36 Quality of Life Scale)
2.9. Statistical Analysis
3. Results
4. Discussion
4.1. Strength of the Study
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nouri, M.; Tavakkolian, A.; Mousavi, S.R. Association of dysfunctional uterine bleeding with high body mass index and obesity as a main predisposing factor. Diab. Met. Syndr. Clin. Res. Rev. 2014, 8, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Munro, M.G.; Critchley, H.O.D.; Broder, M.S.; Fraser, I.S.; Working, F.; Disorders, M. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int. J. Gynaecol. Obstet. 2011, 113, 3–13. [Google Scholar] [CrossRef]
- Fraser, I.S.; Langham, S.; Uhl-hochgraeber, K. Health-related quality of life and economic burden of abnormal uterine bleeding. Exp. Rev. Obstet. Gynecol. 2018, 4, 179–189. [Google Scholar] [CrossRef]
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Heavy Menstrual Bleeding. Available online: https://www.ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27sHealth/Patientinformation/Heavy-menstrual-bleeding-bleeding-pamphlet.pdf?ext=.pdf (accessed on 10 August 2022).
- Kjerulff, K.H.; Erickson, B.A.; Langenberg, P.W. Chronic gynecological conditions reported by US women: Findings from the National Health Interview Survey. Am. J. Public Health 1996, 86, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Frick, K.D.; Clark, M.A.; Steinwachs, D.M.; Langenberg, P.; Stovall, D.; Munro, M.G.; Dickersin, K. Financial and quality-of-life burden of dysfunctional uterine bleeding among women agreeing to obtain surgical treatment. Womens Health Issues 2009, 19, 70–78. [Google Scholar] [CrossRef] [PubMed]
- The Royal College of Obstetricians and Gynecologists. National Heavy Menstrual Bleeding Audit; Royal College of Obstetricians and Gynaecologists, 27 Sussex Place, Regent’s Park: London, UK, 2014; p. 47. [Google Scholar]
- Davidson, B.R.; Dipiero, C.M.; Govoni, K.D.; Littleton, S.S.; Neal, J.L. Abnormal uterine bleeding during the reproductive years. J. Midwifery Womens Health 2012, 57, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Doan, Q.V.; Blumenthal, P.; Dubois, R.W. A systematic review evaluating health-related quality of life, work impairment, and health-care costs and utilization in abnormal uterine bleeding. Value Health 2007, 10, 183–194. [Google Scholar] [CrossRef] [Green Version]
- Strine, T.W.; Chapman, D.P.; Ahluwalia, I.B. Menstrual-related problems and psychological distress among women in the United States. J. Womens Health 2005, 14, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Matteson, K.A.; Clark, M.A. Questioning our questions: Do frequently asked questions adequately cover the aspects of women’s lives most affected by abnormal uterine bleeding? Opinions of women with abnormal uterine bleeding participating in focus group discussions. Women Health 2010, 50, 195–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.L. Iron Deficiency anemia: A common and curable disease. Cold Spring Harb. Perspect. Med. 2013, 3, a011866. [Google Scholar] [CrossRef] [PubMed]
- Woolcock, J.G.; Critchley, H.O.D.; Munro, M.G.; Broder, M.S.; Fraser, I.S. Review of the confusion in current and historical terminology and definitions for disturbances of menstrual bleeding. Fertil. Steril. 2008, 90, 2269–2280. [Google Scholar] [CrossRef] [PubMed]
- Fraser, I.; Critchley, H.; Broder, M.; Munro, M. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Semin. Reprod. Med. 2011, 29, 383–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark-Coller, T. Dysfunctional uterine bleeding and amenorrhea. Differential diagnosis and management. J. Nurse Midwifery 1991, 36, 49–62. [Google Scholar] [CrossRef]
- Gussi, I. Clinical gynecologic endocrinology and infertility. Acta Endocrinol. 2005, 1, 240. [Google Scholar] [CrossRef]
- Kriplani, A.; Kulshrestha, V.; Agarwal, N. Efficacy and safety of ormeloxifene in management of menorrhagia: A pilot study. J. Obstet. Gynaecol. Res. 2009, 35, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Zakherah, M.S.; Sayed, G.H.; El-Nashar, S.A.; Shaaban, M.M. Pictorial blood loss assessment chart in the evaluation of heavy menstrual bleeding: Diagnostic accuracy compared to alkaline hematin. Gynecol. Obstet. Invest. 2011, 71, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Doraiswami, S.; Johnson, T.; Rao, S.; Rajkumar, A.; Vijayaraghavan, J.; Panicker, V.K. Study of endometrial pathology in abnormal uterine bleeding. J. Obstet. Gynecol. India 2011, 61, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.M.; Uk, F.; Al-githmi, F.I. Factors influencing job satisfaction of employees. Bahrain Med. Bull. 2011, 33, 285–291. [Google Scholar]
- Bindroo, S.; Garg, M.; Kaur, T. Histopathological spectrum of endometrium in abnormal uterine bleeding. Int. J. Reprod. ContraceptionObstet. Gynecol. 2018, 7, E3633. [Google Scholar] [CrossRef] [Green Version]
- Jairajpuri, Z.; Jetley, S.; Rana, S. Morphological spectrum of endometrial pathology in middle-aged women with atypical uterine bleeding: A study of 219 cases. J. Midlife Health 2013, 4, 216–220. [Google Scholar] [CrossRef]
- Nayak, A.K.; Hazra, K.; Jain, M.K. Clinico-pathological evaluation of dysfunctional uterine bleeding. Int. J. Contemp. Med. Res. 2017, 4, 920–924. [Google Scholar]
- Mahapatra, M.; Mishra, P. Clinicopathological evaluation of abnormal uterine bleeding. J. Health Res. Rev. 2015, 2, 45–49. [Google Scholar] [CrossRef]
- Mahmoud, M.M.; Ghazi, R.A. Endometrial histopathological changes in women with abnormal uterine bleeding in Kirkuk city, a clinicopathological study. Med. J. Babylon 2013, 10, 567–582. [Google Scholar]
- Afghan, S.; Yasmeen, A. Abnormal uterine bleeding (AUB) a clinicopathological study of 150 cases. Ann. Pak. Inst. Med. Sci. 2013, 9, 201–204. [Google Scholar]
- Zawar, M.P.; Deshpande, N.M.; Gadgil, P.A.; Mahanta, A.A. Histopathological study of endometrium in infertility. Indian J. Pathol. Microbiol. 2003, 46, 630–633. [Google Scholar] [PubMed]
- Doddamani, U.G.; Doddamani, G.B.; Katageri, G.; Mallapur, A. Clinicopathological correlation of endometrium in abnormal uterine bleeding. Sch. J. Appl. Med. Sci. 2014, 2, 46–49. [Google Scholar]
- Shravage, J.; Mekhala, D.; Bellad, M.B.; Ganachari, M.S.; Dhumale, H.A. Ormeloxifene versus medroxyprogesterone acetate (MPA) in the treatment of dysfunctional uterine bleeding: A double-blind randomized controlled trial. J. Safog. 2011, 3, 21–24. [Google Scholar]
- Dhananjay, B.S.; Nanda, S.K. The role of sevista in the management of dysfunctional uterine bleeding. J. Clin. Diagn. Res. 2013, 7, 132–134. [Google Scholar]
- Ravibabu, K.; Palla, J.; Chintatada, G.S. A study of efficacy of ormeloxifene in the pharmacological management of dysfunctional uterine bleeding. J. Clin. Diagn. Res. 2013, 7, 2534–2536. [Google Scholar] [CrossRef]
- Pati, T.; Chanania, K.; Marandi, S.; Hansa, J. Ormeloxifene–looking beyond contraception. J. Midlife Health 2017, 8, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Godha, Z.; Mohsin, Z.; Hakim, S.; Wasim, S. Comparative study of Ormeloxifene and Medroxyprogesterone acetate in abnormal uterine bleeding. J. Obstet. Gynecol. India 2016, 66, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varwatte, P.B.; Fonseca, M. Study of the efficacy of ormeloxifene in abnormal uterine bleeding. Int. J. Reprod. Contracept. Obstet. Gynecol. 2020, 9, 4941–4946. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Particulars (Drug Used) | Trade Name and Manufacturer | Total Dose/Tablets Needed | Price/Strip of 10 Tablets (INR) | Total Expenditure for 3 Months (INR) |
|---|---|---|---|---|
| Medroxyprogesterone Acetate | Deviry Torrent pharmaceuticals | 12.6 strips of 10 tablets (13 strips) | 60 | 780 |
| Ormeloxifene | Sevista Torrent pharmaceuticals | 2 strips of 10 tablets | 195 | 390 |
| Baseline Demographic and Clinical Characteristics of the Study Patients | |||
|---|---|---|---|
| Variable | Ormeloxifene (n = 120) | Medroxyprogesterone Acetate (n = 120) | p-Value * |
| Age-years | 40.31 ± 5.852 | 39.90 ± 5.418 | 0.926 |
| Height—m | 1.659 ± 0.107 | 1.694 ± 0.129 | 0.585 |
| Body Weight—kg | 66.60 ± 6.054 | 66.72 ± 6.872 | 0.928 |
| Body Mass Index (BMI#)—kg/m2 | 23.37 ± 3.70 | 23.63 ± 4.574 | 0.884 |
| Comorbidities | |||
| Diabetes | 22 | 33 | |
| Sub-Clinical Hypothyroidism | 19 | 24 | |
| Urinary tract infection | 12 | 8 | |
| Obesity | 43 | 34 | |
| Laboratory Parameters before the start of therapy | |||
| Haemoglobin—g/dL | 8.56 ± 0.77 | 8.60 ± 0.97 | 0.809 |
| PBLAC Score | 289.92 ± 42.39 | 287.38 ± 40.94 | 0.964 |
| Endometrial Thickness (mm) | 8.52 ± 1.61 | 8.40 ± 2.09 | 0.808 |
| Bleeding Duration (Days) | 16.88 ± 6.46 | 15.91 ± 5.04 | 0.860 |
| Relationship between parity and Abnormal uterine bleeding found in this study (Percentage is calculated as cases divided by total number of cases in both the groups) | |||
| Parity | No of patients (%) | No of patients (%) | |
| Unmarried | 14 (5.83%) | 10 (4.16%) | |
| Nullipara | 25 (10.41%) | 33 (13.75%) | |
| Parity 2 | 23 (9.58%) | 35 (14.58%) | |
| Multiparity | 58 (24.16%) | 42 (17.5%) | |
| Distribution of AUB cases according to age (Percentage is calculated as cases divided by total number of cases in both the groups) | |||
| Age Group In years | No of patients (%) | No of patients (%) | |
| 20–25 | 0 (0%) | 0 (0%) | |
| 26–30 | 9 (3.75%) | 13 (5.41%) | |
| 31–35 | 20 (8.33%) | 24 (10%) | |
| 36–40 | 37 (15.41%) | 34 (14.16%) | |
| 41–45 | 50 (20.83%) | 40 (16.66%) | |
| 46–50 | 2 (0.83%) | 5 (2.08%) | |
| 51–55 | 2 (0.83%) | 4 (1.66%) | |
| Incidence of various modes of presentation of abnormal uterine bleeding (Percentage is calculated as cases divided by total number of cases in both the groups) | |||
| Type | No. of patients (%) | No. of patients (%) | |
| Menorrhagia | 60 (25%) | 52 (21.66%) | |
| Metrorrhagia | 31 (12.91%) | 35 (14.58%) | |
| Polymenorrhagia | 21 (8.75%) | 19 (7.91%) | |
| Polymenorrhoea | 5 (2.08%) | 9 (3.75%) | |
| Continuous bleeding | 3 (1.25%) | 5 (2.08%) | |
| Baseline Clinical Data | |||
|---|---|---|---|
| Laboratory Parameters | Ormeloxifene (n = 120) | Medroxyprogesterone Acetate (n = 120) | * p-Value |
| Haemoglobin—g/dL | 8.56 ± 0.77 | 8.60 ± 0.97 | 0.809 |
| PBLAC Score | 289.92 ± 42.39 | 287.38 ± 40.94 | 0.964 |
| Endometrial Thickness (mm) | 8.52 ± 1.61 | 8.40 ± 2.09 | 0.808 |
| Bleeding Duration (Days) | 16.88 ± 6.46 | 15.91 ± 5.04 | 0.860 |
| 3rd month clinical data | |||
| Laboratory Parameters | Ormeloxifene (n = 117) | Medroxyprogesterone Acetate (n = 119) | * p-value |
| Haemoglobin—g/dL | 10.12 ± 0.87 | 9.55 ± 0.90 | 0.0001 |
| PBLAC Score | 128.11 ± 33.10 | 123.5 ± 29.57 | 0.0001 |
| Endometrial Thickness (mm) | 6.92 ± 1.68 | 7.46 ± 1.97 | 0.0001 |
| Bleeding Duration (Days) | 7.76 ± 1.55 | 8.7 ± 1.91 | 0.024 |
| * p-value (within the group) | 0.0001 | 0.0001 | |
| Dimensions of Quality of Life Scale | Group A (ORM) Before Therapy | Group A (ORM) After Therapy | Group B (MPA) Before Therapy | Group B (MPA) After Therapy | p-Value (Between the Groups) | p-Value (Within the Groups) |
|---|---|---|---|---|---|---|
| Physical function | 24.39 | 28.95 | 25.41 | 27.02 | 0.0001 | 0.0001 |
| Social functioning | 7.26 | 9.2 | 8.1 | 8.6 | ||
| Mental health | 17.21 | 20.1 | 16.95 | 18.2 | ||
| General health | 15.35 | 18.32 | 15.9 | 16.3 | ||
| Role physical | 1.72 | 2.9 | 1.6 | 2.2 | ||
| Role emotional | 1.49 | 3.2 | 1.83 | 2.63 | ||
| Energy/Fatigue | 12.99 | 18 | 13.6 | 16 | ||
| Pain | 6.25 | 9 | 7.1 | 8.3 |
| Health and Functions | Group A (ORM) (%) | Group B (MPA) (%) | p-Value |
|---|---|---|---|
| Very dissatisfied | 5 | 10 | 0.0001 |
| Moderately dissatisfied | 10 | 20 | 0.0001 |
| Slightly dissatisfied | 20 | 31.66 | 0.0001 |
| Slightly satisfied | 31.66 | 16.66 | 0.0001 |
| moderately satisfied | 16.68 | 11.68 | 0.0001 |
| Very satisfied | 16.66 | 10 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mir, S.A.; Ara, R.; Amin, F.; Malik, A.; Hamid, L.; Ali, T.; Bader, G.N.; Wani, S.U.D.; Almuqbil, M.; Alshehri, S.; et al. Evaluation of the Safety and Efficacy of Ormeloxifene, a Selective Estrogen Receptor Modulator and Medroxyprogesterone Acetate in Women with Non-Structural Abnormal Uterine Bleeding: A Randomized Clinical Trial. Medicina 2022, 58, 1503. https://doi.org/10.3390/medicina58111503
Mir SA, Ara R, Amin F, Malik A, Hamid L, Ali T, Bader GN, Wani SUD, Almuqbil M, Alshehri S, et al. Evaluation of the Safety and Efficacy of Ormeloxifene, a Selective Estrogen Receptor Modulator and Medroxyprogesterone Acetate in Women with Non-Structural Abnormal Uterine Bleeding: A Randomized Clinical Trial. Medicina. 2022; 58(11):1503. https://doi.org/10.3390/medicina58111503
Chicago/Turabian StyleMir, Suhail Ahmad, Rifat Ara, Fiza Amin, Anjum Malik, Laraibah Hamid, Tabasum Ali, Ghulam Nabi Bader, Shahid Ud Din Wani, Mansour Almuqbil, Sultan Alshehri, and et al. 2022. "Evaluation of the Safety and Efficacy of Ormeloxifene, a Selective Estrogen Receptor Modulator and Medroxyprogesterone Acetate in Women with Non-Structural Abnormal Uterine Bleeding: A Randomized Clinical Trial" Medicina 58, no. 11: 1503. https://doi.org/10.3390/medicina58111503