
Computed Tomography Does Not Improve Intra- and Interobserver Agreement of Hertel Radiographic Prognostic Criteria
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Intraobserver Agreement
3.2. Interobserver Agreement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Individual Folders with Instructions on How to Respond the Survey
- -
- This study seeks to evaluate Hertel’s radiographic criteria using computed tomography (CT);
- -
- We separated 20 cases of fractures of the proximal humerus, with X-rays and CT images, individualized in a separate folder;
- -
- Randomization was performed, and the cases were numbered from 1 to 20;
- -
- We ask that each examiner define which Hertel criteria are present by evaluating the radiographs and then their respective CT scans;
- -
- At the end of the evaluation, each examiner will have made 40 evaluations. 2 for each case;
- -
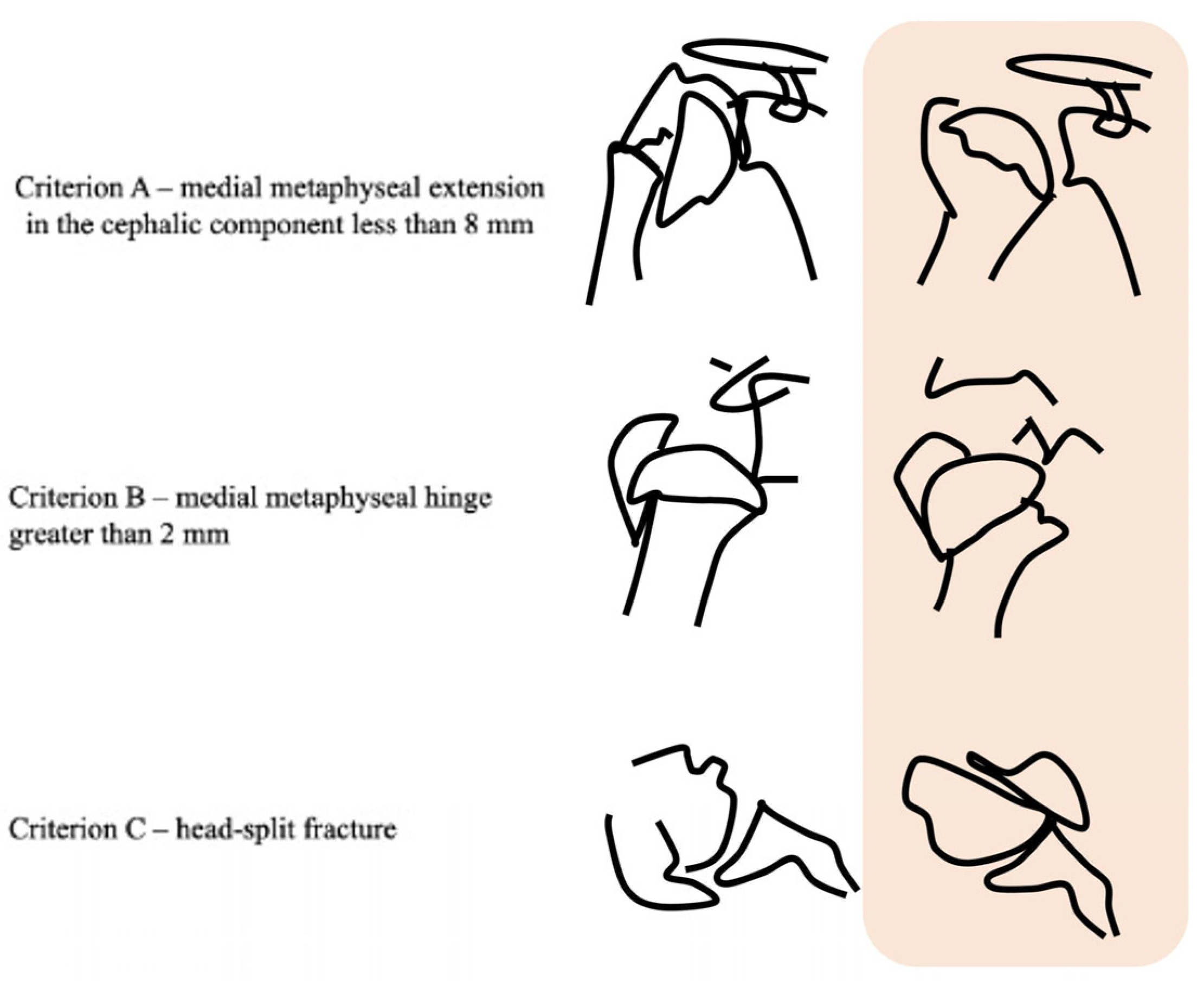
- In the folder with the files there is a photo explaining each of the 3 Hertel criteria, (reproduced from these author original article);
- -
- We kindly ask you to return these results for each patient. Example:
- -
- criterion A present/absent/cannot evaluate;
- -
- criterion B present/absent/cannot evaluate;
- -
- criterion C present/absent/cannot evaluate;
- -
- criterion A present/absent/cannot evaluate;
- -
- criterion B present/absent/cannot evaluate;
- -
- criterion C present/absent/cannot evaluate;
- -
- The annotation of these results can be done in the way that suits the examiner. Annotated on a sheet of paper, or in an Excell table, or in a .doc text;
- -
- After ending with the document, please send it to the emails: p_tullio@hotmail.com and v_giordano@me.com;
- -
- Very soon we will send the same cases again but with a new randomization for a second evaluation, allowing us to make an intra and interobserver agreement comparison.
References
- Jabran, A.; Peach, C.; Ren, L. Biomechanical analysis of plate systems for proximal humerus fractures: A systematic literature review. Biomed. Eng. Online 2018, 17, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hageman, M.G.; Jayakumar, P.; King, J.D.; Guitton, T.G.; Doornberg, J.N.; Ring, D.; Science of Variation Group. The factors influencing the decision making of operative treatment for proximal humeral fractures. J. Shoulder Elb. Surg. 2015, 24, e21–e26. [Google Scholar] [CrossRef] [PubMed]
- Keding, A.; Handoll, H.; Brealey, S.; Jefferson, L.; Hewitt, C.; Corbacho, B.; Torgerson, D.; Rangan, A. The impact of surgeon and patient treatment preferences in an orthopaedic trauma surgery trial. Trials 2019, 20, 570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maccagnano, G.; Solarino, G.; Pesce, V.; Vicenti, G.; Coviello, M.; Nappi, V.S.; Giannico, O.V.; Notarnicola, A.; Moretti, B. Plate vs reverse shoulder arthroplasty for proximal humeral fractures: The psychological health influence the choice of device? World J. Orthop 2022, 13, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Belayneh, R.; Lott, A.; Haglin, J.; Konda, S.; Zuckerman, J.D.; Egol, K.A. Osteonecrosis after surgically repaired proximal humerus fractures is a predictor of poor outcomes. J. Orthop. Trauma 2018, 32, e387–e393. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, C.S.; Cofield, R.H. Osteonecrosis of the shoulder. Orthop Trans. 1987, 11, 239. [Google Scholar]
- Hertel, R.; Hempfing, A.; Stiehler, M.; Leunig, M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J. Shoulder Elb. Surg. 2004, 13, 427–433. [Google Scholar] [CrossRef]
- Patel, S.; Colaco, H.B.; Elvey, M.E.; Lee, M.H. Post-traumatic osteonecrosis of the proximal humerus. Injury 2015, 46, 1878–1884. [Google Scholar] [CrossRef]
- Majed, A.; Macleod, I.; Bull, A.M.; Zyto, K.; Resch, H.; Hertel, R.; Reilly, P.; Emery, R.J. Proximal humeral fracture classification systems revisited. J. Shoulder Elb. Surg. 2011, 20, 1125–1132. [Google Scholar] [CrossRef]
- Sukthankar, A.V.; Leonello, D.T.; Hertel, R.W.; Ding, G.S.; Sandow, M.J. A comprehensive classification of proximal humeral fractures: HGLS system. J. Shoulder Elb. Surg. 2013, 22, e1–e6. [Google Scholar] [CrossRef]
- Campochiaro, G.; Rebuzzi, M.; Baudi, P.; Catani, F. Complex proximal humerus fractures: Hertel’s criteria reliability to predict head necrosis. Musculoskelet. Surg. 2015, 99, S9–S15. [Google Scholar] [CrossRef]
- Neer, C.S., 2nd. Displaced proximal humeral fractures. I. Classification and evaluation. J. Bone Joint Surg. Am. 1970, 52, 1077–1089. [Google Scholar] [CrossRef]
- Senna, L.F.; Pires, E.; Albuquerque, R. Modified axillary radiograph of the shoulder: A new position. Rev. Bras. Ortop. 2016, 52, 115–118. [Google Scholar] [CrossRef] [Green Version]
- Neer, C.S., 2nd. Displaced proximal humeral fractures. II. Treatment of three-part and four-part displacement. J. Bone Joint Surg. Am. 1970, 52, 1090–1103. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.M.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.; et al. Towards complete and accurate reporting of studies of diagnostic accuracy: The STARD initiative. Clin. Radiol. 2003, 58, 575–580. [Google Scholar] [CrossRef] [Green Version]
- Giordano, V.; Gomes, A.F.; Amaral, N.P.; Albuquerque, R.P.; Pires, R.E. Preventing surgical complications: A survey on surgeons’ perception of intra-articular malleolar screw misplacement in a cadaveric study. Patient Saf. Surg. 2011, 5, 24. [Google Scholar] [CrossRef] [Green Version]
- Oladiran, O.; Gichoya, J.; Purkayastha, S. Conversion of JPG image into DICOM image format with one click tagging. In Digital Human Modeling. Applications in Health, Safety, Ergonomics, and Risk Management: Health and Safety; Duffy, V., Ed.; Springer: Cham, Switzerland, 2017; pp. 61–70. [Google Scholar] [CrossRef] [Green Version]
- El-Boghdadly, K.; Onwochei, D.N.; Millhoff, B.; Ahmad, I. The effect of virtual endoscopy on diagnostic accuracy and airway management strategies in patients with head and neck pathology: A prospective cohort study. Can. J. Anaesth. 2017, 64, 1101–1110. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Solberg, B.D.; Moon, C.N.; Franco, D.P.; Paiement, G.D. Surgical treatment of three and four-part proximal humeral fractures. J. Bone Joint Surg. Am. 2009, 91, 1689–1697. [Google Scholar] [CrossRef]
- Leyshon, R.L. Closed treatment of fractures of the proximal humerus. Acta Orthop. Scand. 1984, 55, 48–51. [Google Scholar] [CrossRef]
- Sandstrom, C.K.; Kennedy, S.A.; Gross, J.A. Acute shoulder trauma: What the surgeon wants to know. Radiographics 2015, 35, 475–492. [Google Scholar] [CrossRef]
- Richards, B.; Riley, J.; Saithna, A. Improving the diagnostic quality and adequacy of shoulder radiographs in a District General Hospital. BMJ Qual. Improv. Rep. 2016, 5, u209855.w3501. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Sola, R.; León-Muñoz, V.J.; Najem-Rizk, A.N.; Soler-Vasco, B.; Arrieta-Martínez, C.J.; López-Sorroche, E.; Cárdenas-Grande, E.; Salmerón-Vélez, G.; Ruiz-Molina, J.Á.; Martínez-Martínez, F.; et al. ‘Absolute’ inter-observer classifications agreement for proximal humeral fractures with a single shoulder anteroposterior X-ray. J. Orthop. Surg. 2021, 29, 23094990211010520. [Google Scholar] [CrossRef] [PubMed]
- Iordens, G.I.; Mahabier, K.C.; Buisman, F.E.; Schep, N.W.; Muradin, G.S.; Beenen, L.F.; Patka, P.; van Lieshout, E.M.; sen Hartog, D. The reliability and reproducibility of the Hertel classification for comminuted proximal humeral fractures compared with the Neer classification. J. Orthop. Sci. 2016, 21, 596–602. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.M.; Khan, L.A.; Akhtar, M.A. Treatment of anterior fracture-dislocations of the proximal humerus by open reduction and internal fixation. J. Bone Joint Surg. Br. 2006, 88, 502–508. [Google Scholar] [CrossRef]
- Schnetzke, M.; Bockmeyer, J.; Loew, M.; Studier-Fischer, S.; Grützner, P.A.; Guehring, T. Rate of avascular necrosis after fracture dislocations of the proximal humerus: Timing of surgery. Obere Extrem. 2018, 13, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.K.; Hansen, H.R. Post-traumatic avascular necrosis of the humeral head in displaced proximal humeral fractures. J. Trauma 1981, 21, 788–791. [Google Scholar] [CrossRef]
- Neviaser, A.S.; Hettrich, C.M.; Dines, J.S.; Lorich, D.G. Rate of avascular necrosis following proximal humerus fractures treated with a lateral locking plate and endosteal implant. Arch. Orthop. Trauma Surg. 2011, 131, 1617–1622. [Google Scholar] [CrossRef]
- Trupka, A.; Wiedemann, E.; Ruchholtz, S.; Brunner, U.; Habermeyer, P.; Schweiberer, L. Dislozierte Mehrfragmentfrakturen des Humeruskopfes. Bedeutet die Luxation des Kopffragments eine Prognoseverschlechterung? Unfallchirurg 1997, 100, 105–110. [Google Scholar] [CrossRef]
- Thompson, J.H.; Attum, B.; Rodriguez-Buitrago, A.; Yusi, K.; Cereijo, C.; Obremskey, W.T. Open reduction and internal fixation with a locking plate via deltopectoral approach for the treatment of three and four-part and proximal humeral fractures. JBJS Essent. Surg. Tech. 2018, 8, e26. [Google Scholar] [CrossRef]
- Berkes, M.B.; Dines, J.S.; Little, M.T.; Garner, M.R.; Shifflett, G.D.; Lazaro, L.E.; Wellman, D.S.; Dines, D.M.; Lorich, D.G. The impact of three-dimensional CT imaging on intraobserver and interobserver reliability of proximal humeral fracture classifications and treatment recommendations. J. Bone Joint Surg. Am. 2014, 96, 1281–1286. [Google Scholar] [CrossRef]
- Greiner, S.; Kääb, M.J.; Haas, N.P.; Bail, H.J. Humeral head necrosis rate at mid-term follow-up after open reduction and angular stable plate fixation for proximal humeral fractures. Injury 2009, 40, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Sugano, N.; Nishii, T.; Hananouchi, T.; Yoshikawa, H. Extent of osteonecrosis on MRI predicts humeral head collapse. Clin. Orthop. Relat. Res. 2008, 466, 1074–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahrs, C.; Rolauffs, B.; Südkamp, N.P.; Schmal, H.; Eingartner, C.; Dietz, K.; Pereira, P.L.; Weise, K.; Lingenfelter, E.; Helwig, P. Indications for computed tomography (CT-) diagnostics in proximal humeral fractures: A comparative study of plain radiography and computed tomography. BMC Musculoskelet. Disord. 2009, 10, 33. [Google Scholar] [CrossRef] [Green Version]
- Chelli, M.; Gasbarro, G.; Lavoué, V.; Gauci, M.O.; Raynier, J.L.; Trojani, C.; Boileau, P. The reliability of the Neer classification for proximal humerus fractures: A survey of orthopedic shoulder surgeons. JSES Int. 2022, 6, 331–337. [Google Scholar] [CrossRef]
- Jia, X.; Chen, Y.; Qiang, M.; Zhang, K.; Li, H.; Jiang, Y.; Zhang, Y. Compared to X-ray, three-dimensional computed tomography measurement is a reproducible radiographic method for normal proximal humerus. J. Orthop. Surg. Res. 2016, 11, 82. [Google Scholar] [CrossRef] [Green Version]
- Stirma, G.A.; Secundino, A.R.; Gonzalez, G.F.G.; Sola, W.C.; de Souza, G.A.L.; Dau, L. Inter/intra-observer evaluation between radiographs and tomographies for proximal humerus fracture. Acta Ortop. Bras. 2020, 28, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Dauwe, J.; Mys, K.; Putzeys, G.; Schader, J.F.; Richards, R.G.; Gueorguiev, B.; Varga, P.; Nijs, S. Advanced CT visualization improves the accuracy of orthopaedic trauma surgeons and residents in classifying proximal humeral fractures: A feasibility study. Eur. J. Trauma Emerg. Surg. 2020, 1–7. [Google Scholar] [CrossRef]
- Cocco, L.F.; Aihara, A.Y.; Lopes, F.P.P.L.; Werner, H.; Franciozi, C.E.; Dos Reis, F.B.; Luzo, M.V.M. Three-dimensional printing models increase inter-rater agreement for classification and treatment of proximal humerus fractures. Patient Saf. Surg. 2022, 16, 5. [Google Scholar] [CrossRef]
- Puglisi, G.; Montemagno, M.; Denaro, R.; Condorelli, G.; Caruso, V.F.; Vescio, A.; Testa, G.; Pavone, V. 3D-printed models versus CT scan and X-rays imaging in the diagnostic evaluation of proximal humerus fractures: A triple-blind interobserver reliability comparison study. Adv. Orthop. 2022, 2022, 5863813. [Google Scholar] [CrossRef]
- Lambert, S.M. Ischaemia, healing and outcomes in proximal humeral fractures. EFORT Open Rev. 2018, 3, 304–315. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age (Years) | Gender | Side | Mechanism of Trauma | Neer (Parts) | Hertel | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| X-ray C1 | X-ray C2 | X-ray C3 | CT C1 | CT C2 | CT C3 | ||||||
| 1 | 58 | M | R | MCA | III (H, GT, S) | P | A | A | P | A | A |
| 2 | 53 | F | R | Fall to the ground | II (GT) | A | A | A | A | A | A |
| 3 | 52 | F | R | Fall to the ground | III (H GT, S) | P | P | A | P | P | A |
| 4 | 68 | M | R | Fall to the ground | II (LT) | P | P | A | P | P | A |
| 5 | 57 | F | L | Fall to the ground | IV | A | A | I | A | A | A |
| 6 | 65 | F | L | Fall to the ground | IV | I | A | A | A | A | A |
| 7 | 55 | F | L | Fall to the ground | IV | A | A | I | A | A | P |
| 8 | 64 | F | R | Fall to the ground | IV | P | P | A | P | P | A |
| 9 | 67 | F | R | Fall to the ground | IV | A | A | I | A | A | P |
| 10 | 59 | M | L | MCA | III (H, GT, S) | P | A | A | P | A | A |
| 11 | 53 | M | R | MVA | III (H, GT, S) | P | A | A | P | A | A |
| 12 | 56 | F | L | Fall to the ground | II (H) | P | A | A | P | P | A |
| 13 | 52 | F | R | Running over | III (H, GT, S) | P | P | A | P | P | A |
| 14 | 70 | F | R | Fall to the ground | IV | P | A | A | P | A | A |
| 15 | 66 | F | L | Fall to the ground | II (LT) | P | P | A | P | P | A |
| 16 | 58 | F | R | Fall to the ground | III (H, GT, S) | I | A | A | A | A | A |
| 17 | 54 | F | L | Fall to the ground | II (LT) | P | P | A | A | A | A |
| 18 | 69 | M | R | Fall to the ground | II (H) | P | A | A | P | A | A |
| 19 | 53 | F | L | Fall to the ground | II (H) | A | A | A | A | A | A |
| 20 | 59 | F | R | Fall to the ground | III (H, GT, S) | A | A | A | A | A | A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tullio, P.O.d.; Giordano, V.; Belangero, W.D.; Pires, R.E.; de Souza, F.S.; Labronici, P.J.; Zamboni, C.; Malzac, F.; Belangero, P.S.; Ikemoto, R.Y.; et al. Computed Tomography Does Not Improve Intra- and Interobserver Agreement of Hertel Radiographic Prognostic Criteria. Medicina 2022, 58, 1489. https://doi.org/10.3390/medicina58101489
Tullio POd, Giordano V, Belangero WD, Pires RE, de Souza FS, Labronici PJ, Zamboni C, Malzac F, Belangero PS, Ikemoto RY, et al. Computed Tomography Does Not Improve Intra- and Interobserver Agreement of Hertel Radiographic Prognostic Criteria. Medicina. 2022; 58(10):1489. https://doi.org/10.3390/medicina58101489
Chicago/Turabian StyleTullio, Paulo Ottoni di, Vincenzo Giordano, William Dias Belangero, Robinson Esteves Pires, Felipe Serrão de Souza, Pedro José Labronici, Caio Zamboni, Felipe Malzac, Paulo Santoro Belangero, Roberto Yukio Ikemoto, and et al. 2022. "Computed Tomography Does Not Improve Intra- and Interobserver Agreement of Hertel Radiographic Prognostic Criteria" Medicina 58, no. 10: 1489. https://doi.org/10.3390/medicina58101489