
Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review

Abstract
:1. Introduction
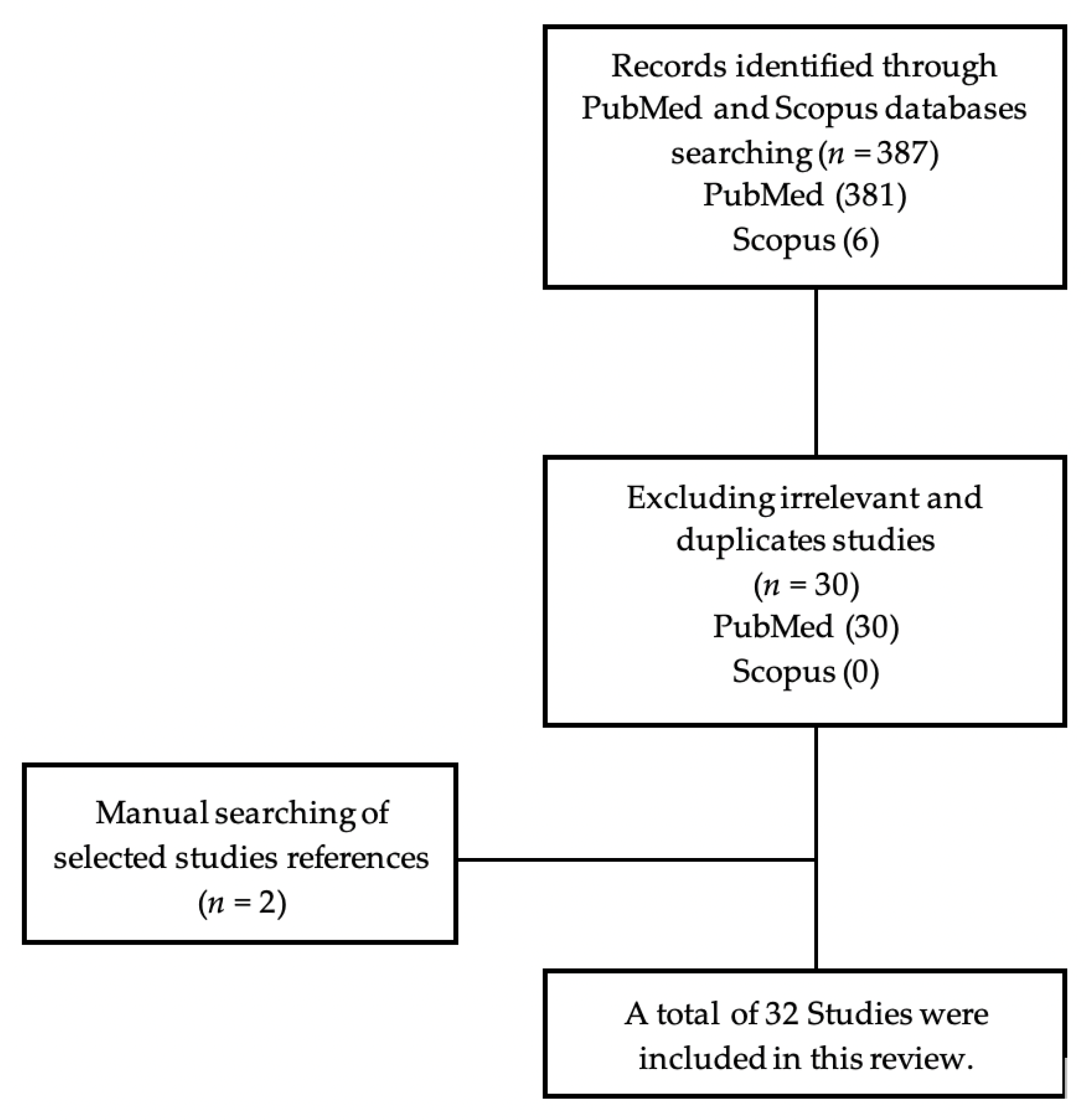
2. Materials and Methods
3. Results
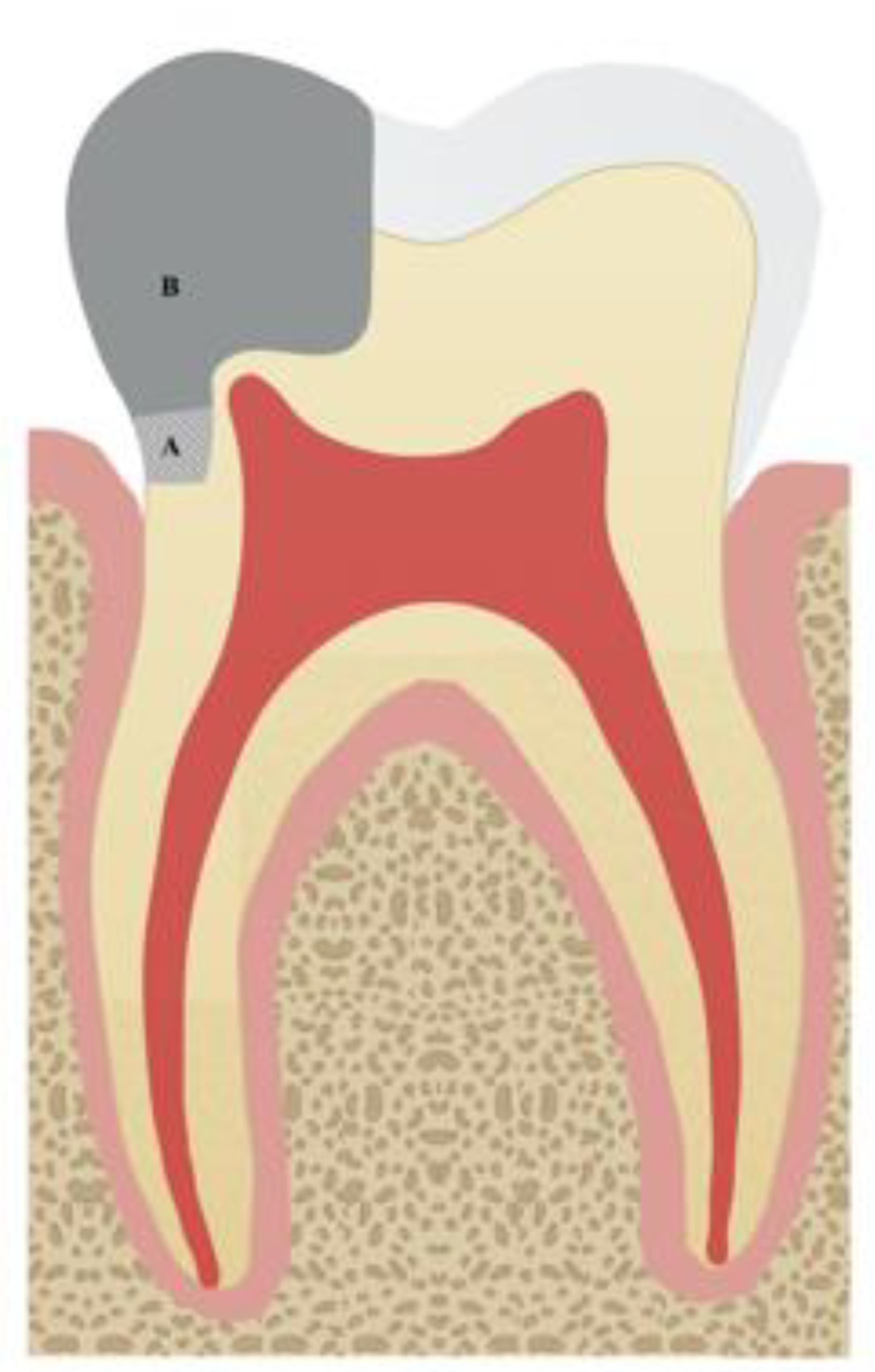
3.1. Deep Margin Elevation Concept
3.2. Periodontal Aspects
3.3. DME versus Surgical Crown Lengthening
3.4. Orthodontic Extrusion
3.5. DME Technique
3.6. Marginal Integrity
3.7. Fracture Resistance of Teeth Restored Using DME
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dietschi, D.; Spreafico, R. Current Clinical Concepts for Adhesive Cementation of Tooth-Colored Posterior Restorations. Pract. Periodont. Aesthet. Dent. 1998, 10, 47–54. [Google Scholar]
- Magne, P.; Spreafico, R.C. Deep Margin Elevation: A Paradigm Shift. Am. J. Esthet. Dent. 2012, 2, 86–96. [Google Scholar]
- Juloski, J.; Köken, S.; Ferrari, M. Cervical Margin Relocation in Indirect Adhesive Restorations: A Literature Review. J. Prosthodont. Res. 2018, 62, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Binalrimal, S.R.; Banjar, W.M.; Alyousef, S.; Alawad, M.; Alawad, G. Assessment of Knowledge, Attitude, and Practice Regarding Deep Margin Elevation (DME) Among Dental Practitioners in Riyadh, Saudi Arabia. Fam. Med. Prim. Care Rev. 2021, 10, 1931. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, A.; Tirlet, G. Deep Margin Elevation Versus Crown Lengthening: Biologic Width Revisited. Int. J. Esthet. Dent. 2018, 13, 334–356. [Google Scholar]
- Kielbassa, A.M.; Philipp, F. Restoring Proximal Cavities of Molars Using the Proximal Box Elevation Technique: Systematic Review and Report of a Case. Quintessence Int. 2015, 46, 751–764. [Google Scholar] [PubMed]
- D’Arcangelo, C.; Vanini, L.; Casinelli, M.; Frascaria, M.; De Angelis, F.; Vadini, M.; D’Amario, M. Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature Review. Compend. Contin. Educ. Dent. 2015, 36, 570–578. [Google Scholar]
- Veneziani, M. Adhesive Restorations in the Posterior Area with Subgingival Cervical Margins: New Classification and Differentiated Treatment Approach. Eur. J. Esthet. Dent. 2010, 5, 50–76. [Google Scholar]
- Ferrari, M.; Koken, S.; Grandini, S.; Ferrari Cagidiaco, E.; Joda, T.; Discepoli, N. Influence of Cervical Margin Relocation (CMR) on Periodontal Health: 12-Month Results of a Controlled Trial. J. Dent. 2018, 69, 70–76. [Google Scholar] [CrossRef]
- Cardoso, M.; de Almeida Neves, A.; Mine, A.; Coutinho, E.; Van Landuyt, K.; De Munck, J.; Van Meerbeek, B. Current Aspects on Bonding Effectiveness and Stability in Adhesive Dentistry. Aust. Dent. J. 2011, 56, 31–44. [Google Scholar]
- Da Silva, D.; Ceballos, L.; Fuentes, M. Influence of the Adhesive Strategy in the Sealing Ability of Resin Composite Inlays After Deep Margin Elevation. J. Clin. Exp. Dent. 2021, 8, e886–e893. [Google Scholar] [CrossRef]
- Ilgenstein, I.; Zitzmann, N.; Bühler, J.; Wegehaupt, F.; Attin, T.; Weiger, R.; Krastl, G. Influence of Proximal Box Elevation on the Marginal Quality and Fracture Behavior of Root-Filled Molars Restored with CAD/CAM Ceramic or Composite Onlays. Clin. Oral. Investig. 2014, 19, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Grubbs, T.; Vargas, M.; Kolker, J.; Teixeira, E. Efficacy of Direct Restorative Materials in Proximal Box Elevation on the Margin Quality and Fracture Resistance of Molars Restored with CAD/CAM Onlays. Oper. Dent. 2020, 45, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Da Silva Gonçalves, D.; Cura, M.; Ceballos, L.; Fuentes, M. Influence of Proximal Box Elevation on Bond Strength of Composite Inlays. Clin. Oral. Investig. 2017, 21, 247–254. [Google Scholar] [CrossRef]
- Roggendorf, M.; Krämer, N.; Dippold, C.; Vosen, V.; Naumann, M.; Jablonski-Momeni, A.; Frankenberger, R. Effect of Proximal Box Elevation with Resin Composite on Marginal Quality of Resin Composite Inlays in Vitro. J. Dent. 2012, 40, 1068–1073. [Google Scholar] [CrossRef]
- Spreafico, R.; Marchesi, G.; Turco, G.; Frassetto, A.; Di Lenarda, R.; Mazzoni, A.; Cadenaro, M.; Breschi, L. Evaluation of the in Vitro Effects of Cervical Marginal Relocation Using Composite Resins on the Marginal Quality of CAD/CAM Crowns. J. Adhes. Dent. 2016, 18, 355–362. [Google Scholar]
- Frankenberger, R.; Hehn, J.; Hajtó, J.; Krämer, N.; Naumann, M.; Koch, A.; Roggendorf, M. Effect of Proximal Box Elevation with Resin Composite on Marginal Quality of Ceramic Inlays in Vitro. Clin. Oral. Investig. 2013, 17, 177–183. [Google Scholar] [CrossRef]
- Zaruba, M.; Göhring, T.; Wegehaupt, F.; Attin, T. Influence of a Proximal Margin Elevation Technique on Marginal Adaptation of Ceramic Inlays. Acta Odontol. Scand. 2012, 71, 317–324. [Google Scholar]
- Dietschi, D.; Spreafico, R. Evidence-Based Concepts and Procedures for Bonded Inlays and Onlays. Part I. Historical Perspectives and Clinical Rationale for a Biosubstitutive Approach. Int. J. Esthet. Dent. 2015, 10, 210–227. [Google Scholar]
- Rocca, G.T.; Rizcalla, N.; Krejci, I.; Dietschi, D. Evidence-Based Concepts and Procedures for Bonded Inlays and Onlays. Part I.I. Guidelines for Cavity Preparation and Restoration Fabrication. Int. J. Esthet. Dent. 2015, 10, 392–413. [Google Scholar]
- Müller, V.; Friedl, K.; Friedl, K.; Hahnel, S.; Handel, G.; Lang, R. Influence of Proximal Box Elevation Technique on Marginal Integrity of Adhesively Luted Cerec Inlays. Clin. Oral Investig. 2017, 21, 607–612. [Google Scholar] [CrossRef]
- Köken, S.; Juloski, J.; Sorrentino, R.; Grandini, S.; Ferrari, M. Marginal Sealing of Relocated Cervical Margins of Mesio-Occluso-Distal Overlays. J. Oral Sci. 2018, 60, 460–468. [Google Scholar] [CrossRef] [Green Version]
- Marchesi, G.; Spreafico, R.; Frassetto, A.; Turco, G.; Di Lenarda, R.; Cadenaro, M.; Breschi, L. Cervical Margin-Relocation of CAD/CAM Lithium Disilicate Ceramic Crown Using Resin-Composite. Dent. Mater. 2014, 30, e14. [Google Scholar] [CrossRef]
- Lefever, D.; Gregor, L.; Bortolotto, T.; Krejci, I. Supragingival Relocation of Subgingivally Located Margins for Adhesive Inlays/Onlays with Different Materials. J. Adhes. Dent. 2012, 14, 561–567. [Google Scholar]
- Bresser, R.; van de Geer, L.; Gerdolle, D.; Schepke, U.; Cune, M.; Gresnigt, M. Influence of Deep Margin Elevation and Preparation Design on the Fracture Strength of Indirectly Restored Molars. J. Mech. Behav. Biomed. Mater. 2020, 110, 103950. [Google Scholar] [CrossRef]
- Dietschi, D.; Olsburgh, S.; Krejci, I.; Davidson, C. in vitro evaluation of marginal and internal adaptation after occlusal stressing of indirect class II composite restorations with different resinous bases. Eur. J. Oral. Sci. 2003, 111, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Juloski, J.; Köken, S.; Ferrari, M. No Correlation Between Two Methodological Approaches Applied to Evaluate Cervical Margin Relocation. Dent. Mater. J. 2020, 39, 624–632. [Google Scholar] [CrossRef] [Green Version]
- Alhassan, M.A.; Bajunaid, S.O. Effect of cervical margin relocation technique with composite resin on the marginal integrity of a ceramic onlay: A case report. Gen. Dent. 2020, 68, e1–e3. [Google Scholar]
- Bertoldi, C.; Monari, E.; Cortellini, P.; Generali, L.; Lucchi, A.; Spinato, S.; Zaffe, D. Clinical and Histological Reaction of Periodontal Tissues to Subgingival Resin Composite Restorations. Clin. Oral Investig. 2019, 24, 1001–1011. [Google Scholar] [CrossRef]
- Frese, C.; Wolff, D.; Staehle, H.J. Proximal box elevation with resin composite and the dogma of biological width: Clinical R2-technique and critical review. Oper. Dent. 2014, 39, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Dablanca-Blanco, A.B.; Blanco-Carrión, J.; Martín-Biedma, B.; Varela-Patiño, P.; Bello-Castro, A.; Castelo-Baz, P. Management of large class II lesions in molars: How to restore and when to perform surgical crown lengthening? Restor. Dent. Endod. 2017, 42, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Mugri, M.H.; Sayed, M.E.; Nedumgottil, B.M.; Bhandi, S.; Raj, A.T.; Testarelli, L.; Khurshid, Z.; Jain, S.; Patil, S. Treatment Prognosis of Restored Teeth with Crown Lengthening vs. Deep Margin Elevation: A Systematic Review. Materials 2021, 14, 6733. [Google Scholar] [PubMed]
- Vertolli, T.J.; Martinsen, B.D.; Hanson, C.M.; Howard, R.S.; Kooistra, S.; Ye, L. Effect of Deep Margin Elevation on CAD/CAM-Fabricated Ceramic Inlays. Oper. Dent. 2020, 45, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, H.; Cong, Q.; Zhang, Z.; Du, A.; Wang, Y. Effect of proximal box elevation on fracture resistance and microleakage of premolars restored with ceramic endocrowns. PLoS ONE 2021, 16, e0252269. [Google Scholar] [CrossRef]
- Zaruba, M.; Kasper, R.; Kazama, R.; Wegehaupt, F.; Ender, A.; Attin, T.; Mehl, A. Marginal Adaptation of Ceramic and Composite Inlays in Minimally Invasive Mod Cavities. Clin. Oral Investig. 2013, 18, 579–587. [Google Scholar] [CrossRef] [Green Version]
- Rocca, G.T.; Gregor, L.; Sandoval, M.J.; Krejci, I.; Dietschi, D. in vitro evaluation of marginal and internal adaptation after occlusal stressing of indirect class II composite restorations with different resinous bases and interface treatments. Post-fatigue adaptation of indirect composite restorations. Clin. Oral Investig. 2012, 16, 1385–1393. [Google Scholar]
- Lindberg, A.; van Dijken, J.W.; Lindberg, M. Nine-Year Evaluation of a Polyacid-Modified Resin Composite/Resin Composite Open Sandwich Technique in Class II Cavities. J. Dent. 2007, 35, 124–129. [Google Scholar]
- Shafiei, F.; Akbarian, S. Microleakage of Nanofilled Resin-Modified Glass-Ionomer/Silorane- Or Methacrylate-Based Composite Sandwich Class II Restoration: Effect of Simultaneous Bonding. Oper. Dent. 2014, 39, E22–E30. [Google Scholar] [CrossRef]
- Atlas, A.M.; Raman, P.; Dworak, M.; Mante, F.; Blatz, M.B. Effect of Delayed Light Polymerization of a Dual-Cured Composite Base on Microleakage of Class 2 Posterior Composite Open-Sandwich Restorations. Quintessence Int. 2009, 40, 471–477. [Google Scholar]
- Kamin, S. the biologic width--periodontal-restorative relationship. Singapore Dent. J. 1989, 14, 13–15. [Google Scholar]
- Rochdi, T.; Nouha, M.; Hayet, H.; Abdellatif, B. Deep margin elevation for indirect bonded restorations: A clinical report. Sch. J. Dent. Sci. 2018, 5, 7–16. [Google Scholar]
- Kanca III, J.; GREITZER, G. Class II Restorations with Margins below the CE. J. Esthet. Restor. Dent. 2009, 21, 193–201. [Google Scholar] [CrossRef]
- De Munck, J.; Van Landuyt, K.; Peumans, M.; Poitevin, A.; Lambrechts, P.; Braem, M.; Van Meerbeek, B. a Critical Review of the Durability of Adhesion to Tooth Tissue: Methods and Results. J. Dent. Res. 2005, 84, 118–132. [Google Scholar] [CrossRef]
- Cavalcanti, A.N.; Mitsui, F.H.O.; Lima, A.F.; Mathias, P.; Marchi, G.M. Evaluation of Dentin Hardness and Bond Strength At Different Walls of Class II Preparations. J. Adhes. Dent. 2010, 12, 183–188. [Google Scholar]
- Van Meerbeek, B.; Peumans, M.; Poitevin, A.; Mine, A.; Van Ende, A.; Neves, A.; De Munck, J. Relationship Between Bond-Strength Tests and Clinical Outcomes. Dent. Mater. 2010, 26, e100–e121. [Google Scholar] [CrossRef]
- Mormann, W.; Regolati, B.; Renggli, H. Gingival Reaction to Well-Fitted Subgingival Proximal Gold Inlays. J. Clin. Periodontol. 1974, 1, 120–125. [Google Scholar] [CrossRef]
- Ariaans, K.; Heussen, N.; Schiffer, H.; Wienert, A.; Plümäkers, B.; Rink, L.; Wolfart, S. Use of Molecular Indicators of Inflammation to Assess the Biocompatibility of All-Ceramic Restorations. J. Clin. Periodontol. 2016, 43, 173–179. [Google Scholar] [CrossRef]
- Schmidt, J.; Sahrmann, P.; Weiger, R.; Schmidlin, P.R.; Walter, C. Biologic Width Dimensions—A Systematic Review. J. Clin. Periodontol. 2013, 40, 493–504. [Google Scholar] [CrossRef]
- Magne, P. IDS: Immediate Dentin Sealing (IDS) for tooth preparations. J. Adhes. Dent. 2014, 16, 594. [Google Scholar]
- Padbury, A.; Eber, R.; Wang, H. Interactions Between the Gingiva and the Margin of Restorations. J. Clin. Periodontol. 2003, 30, 379–385. [Google Scholar] [CrossRef]
- Paolantonio, M.; D’ercole, S.; Perinetti, G.; Tripodi, D.; Catamo, G.; Serra, E.; Brue, C.; Piccolomini, R. Clinical and Microbiological Effects of Different Restorative Materials on the Periodontal Tissues Adjacent to Subgingival Class V Restorations. 1-Year Results. J. Clin. Periodontol. 2004, 31, 200–207. [Google Scholar] [CrossRef]
- Waerhaug, J. Effect of rough surfaces upon gingival tissue. J. Dent. Res. 1956, 35, 323–325. [Google Scholar] [CrossRef]
- Larato, D.C. Influence of a composite resin restoration on the gingiva. J. Prosthet. Dent. 1972, 28, 402–404. [Google Scholar] [CrossRef]
- Schatzle, M.; Land, N.P.; Anerud, A.; Boysen, H.; Burgin, W.; Loë, H. the influence of margins of restorations of the periodontal tissues over 26 years. J. Clin. Periodontol. 2001, 28, 57–64. [Google Scholar] [CrossRef]
- Roman-Torres, C.; Cortelli, S.; de Araujo, M.; Aquino, D.; Cortelli, J. a Short-Term Clinical and Microbial Evaluation of Periodontal Therapy Associated with Amalgam Overhang Removal. J. Periodontol. 2006, 77, 1591–1597. [Google Scholar] [CrossRef]
- Waerhaug, J. Histologic Considerations Which Govern Where the Margins of Restorations Should Be Located in Relation to the Gingiva. Dent. Clin. N. Am. 1960, 4, 161–176. [Google Scholar] [CrossRef]
- Waerhaug, J. Presence or Absence of Plaque on Subgingival Restorations. Eur. J. Oral Sci. 1975, 83, 193–201. [Google Scholar] [CrossRef]
- Van Dijken, J.W.; Sjostrom, S. the Effect of Glass Ionomer Cement and Composite Resin Fillings on Marginal Gingiva. J. Clin. Periodontol. 1991, 18, 200–203. [Google Scholar] [CrossRef]
- Truffier-Boutry, D.; Gallez, X.; Demoustier-Champagne, S.; Devaux, J.; Mestdagh, M.; Champagne, B.; Leloup, G. Identification of Free Radicals Trapped in Solid Methacrylated Resins. J. Polym. Sci. Polym. Chem. 2003, 41, 1691–1699. [Google Scholar] [CrossRef]
- Jørgensen, K.D. Restorative resins: Abrasion vs. mechanical properties. Scand. J. Dent. Res. 1980, 88, 557–568. [Google Scholar]
- van Dijken, J.W.; Ruyter, I.E.; Holland, R.I. Porosity in posterior composite resins. Scand. J. Dent. Res. 1986, 94, 471–478. [Google Scholar] [CrossRef] [PubMed]
- McCabe, J.F.; Ogden, A.R. the Relationship Between Porosity, Compressive Fatigue Limit and Wear in Composite Resin Restorative Materials. Dent. Mater. 1987, 3, 9–12. [Google Scholar] [CrossRef]
- Opdam, N.J.; Roeters, J.J.; Joosten, M.; Veeke, O. Porosities and voids in class I restorations placed by six operators using a packable or syringable composite. Dent. Mater. 2002, 18, 58–63. [Google Scholar] [CrossRef]
- Tantbirojn, D.; Versluis, A.; Cheng, Y.S.; Douglas, W.H. Fracture toughness and microhardness of a composite: Do they correlate? J. Dent. 2003, 31, 89–95. [Google Scholar] [CrossRef]
- Drummond, J.L. Degradation, Fatigue, and Failure of Resin Dental Composite Materials. J. Dent. Res. 2008, 87, 710–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planciunas, L.; Puriene, A.; Mackeviciene, G. Surgical lengthening of the clinical tooth crown. Stomatologija 2006, 8, 88–95. [Google Scholar] [PubMed]
- Mishkin, D.J.; Gellin, R.G. Re: Biologic width and crown lengthening. J. Periodontol. 1993, 64, 920. [Google Scholar]
- Gargiulo, A.; Wentz, F.; Orban, B. Dimensions and Relations of the Dentogingival Junction in Humans. J. Periodontol. 1961, 32, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Perez, J.R.; Smukler, H.; Nunn, M.E. Clinical evaluation of the supraosseous gingivae before and after crown lengthening. J. Periodontol. 2007, 78, 1023–1030. [Google Scholar] [CrossRef]
- Van der Velden, U. Probing Force and the Relationship of the Probe Tip to the Periodontal Tissues. J. Clin. Periodontol. 1979, 6, 106–114. [Google Scholar] [CrossRef]
- Armitage, G.C. Manual periodontal probing in supportive periodontal treatment. Periodontol. 2000 1996, 12, 33–39. [Google Scholar] [CrossRef]
- Newcomb, G. the Relationship Between the Location of Subgingival Crown Margins and Gingival Inflammation. J. Periodontol. 1974, 45, 151–154. [Google Scholar] [CrossRef]
- Martins, T.; Bosco, A.; Nóbrega, F.; Nagata, M.; Garcia, V.; Fucini, S. Periodontal Tissue Response to Coverage of Root Cavities Restored with Resin Materials: A Histomorphometric Study in Dogs. J. Periodontol. 2007, 78, 1075–1082. [Google Scholar] [CrossRef]
- Paniz, G.; Nart, J.; Gobbato, L.; Mazzocco, F.; Stellini, E.; De Simone, G.; Bressan, E. Clinical Periodontal Response to Anterior All-Ceramic Crowns with Either Chamfer or Feather-Edge Subgingival Tooth Preparations: Six-Month Results and Patient Perception. Int. J. Periodontics Restor. Dent. 2017, 37, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Valderhaug, J.; Ellingsen, J.; Jokstad, A. Oral Hygiene, Periodontal Conditions and Carious Lesions in Patients Treated with Dental Bridges. A 15-Year Clinical and Radiographic Follow-Up Study. J. Clin. Periodontol. 1993, 20, 482–489. [Google Scholar] [CrossRef]
- Lang, N.; Kiel, R.; Anderhalden, K. Clinical and Microbiological Effects of Subgingival Restorations with Overhanging or Clinically Perfect Margins. J. Clin. Periodontol. 1983, 10, 563–578. [Google Scholar] [CrossRef]
- Valderhaug, J.; Birkeland, J. Periodontal Conditions in Patients 5 Years Following Insertion of Fixed Prostheses. J. Oral Rehabil. 1976, 3, 237–243. [Google Scholar] [CrossRef]
- Ingber, J.S.; Rose, L.F.; Coslet, J.G. the “biologic width”: A concept in periodontics and restorative dentistry. Alpha Omegan. 1977, 70, 62–65. [Google Scholar]
- Al-Sowygh, Z.H. Does Surgical Crown Lengthening Procedure Produce Stable Clinical Outcomes for Restorative Treatment? A Meta-Analysis. J. Prosthodont. 2019, 28, e103–e109. [Google Scholar] [CrossRef] [Green Version]
- Mavrogiannis, M.; Ellis, J.S.; Seymour, R.A.; Thomason, J.M. the efficacy of three different surgical techniques in the management of drug-induced gingival overgrowth. J. Clin. Periodontol. 2006, 33, 677–682. [Google Scholar] [CrossRef]
- Maynard, J.G., Jr.; Wilson, R.D. Physiologic dimensions of the periodontium significant to the restorative dentist. J. Periodontol. 1979, 50, 170–174. [Google Scholar] [CrossRef]
- Pilalas, I.; Tsalikis, L.; Tatakis, D.N. Pre-restorative crown lengthening surgery outcomes: A systematic review. J. Clin. Periodontol. 2016, 43, 1094–1108. [Google Scholar] [CrossRef]
- Patil, K.; Khalighinejad, N.; El-Refai, N.; Williams, K.; Mickel, A. the Effect of Crown Lengthening on the Outcome of Endodontically Treated Posterior Teeth: 10-year Survival Analysis. J. Endod. 2019, 45, 696–700. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. a prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 2: Tooth survival. Int. Endod. J. 2011, 44, 610–625. [Google Scholar] [CrossRef]
- Moghaddam, A.S.; Radafshar, G.; Taramsari, M.; Darabi, F. Long-term survival rate of teeth receiving multidisciplinary endodontic, periodontal and prosthodontic treatments. J. Oral Rehabil. 2014, 41, 236–242. [Google Scholar] [CrossRef]
- Lanning, S.K.; Waldrop, T.C.; Gunsolley, J.C.; Maynard, J.G. Surgical crown lengthening: Evaluation of the biological width. J. Periodontol. 2003, 7, 468–474. [Google Scholar] [CrossRef] [Green Version]
- Rocca, G.T.; Krejci, I. Bonded indirect restorations for posterior teeth: The luting appointment. Quintessence Int. 2007, 38, 543–553. [Google Scholar]
- Rocca, G.T.; Krejci, I. Bonded indirect restorations for posterior teeth: From cavity preparation to provisionalization. Quintessence Int. 2007, 38, 371–379. [Google Scholar]
- Castelo-Baz, P.; Argibay-Lorenzo, O.; Muñoz, F.; Martin-Biedma, B.; Darriba, I.L.; Miguéns-Vila, R.; Ramos-Barbosa, I.; López-Peña, M.; Blanco-Carrión, J. Periodontal response to a tricalcium silicate material or resin composite placed in close contact to the supracrestal tissue attachment: A histomorphometric comparative study. Clin. Oral Investig. 2021, 25, 5743–5753. [Google Scholar] [CrossRef]
- Stetler, K.J.; Bissada, N.F. Significance of the width of keratinized gingiva on the periodontal status of teeth with submarginal restorations. J. Periodontol. 1987, 58, 696–700. [Google Scholar] [CrossRef]
- Oppermann, R.V.; Gomes, S.C.; Cavagni, J.; Cayana, E.G.; Conceição, E.N. Response to Proximal Restorations Placed Either Subgingivally or Following Crown Lengthening in Patients with No History of Periodontal Disease. Int. J. Periodontics Restor. Dent. 2016, 36, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, R.; Narula, S.C.; Sharma, R.K.; Tewari, S. Evaluation of supracrestal gingival tissue after surgical crown lengthening: A 6-month clinical study. J. Periodontol. 2013, 84, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Deas, D.E.; Moritz, A.J.; McDonnell, H.T.; Powell, C.A.; Mealey, B.L. Osseous surgery for crown lengthening: A 6-month clinical study. J. Periodontol. 2004, 75, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Pontoriero, R.; Carnevale, G. Surgical crown lengthening: A 12-month clinical wound healing study. J. Periodontol. 2001, 72, 841–848. [Google Scholar] [CrossRef]
- Marzadori, M.; Stefanini, M.; Sangiorgi, M.; Mounssif, I.; Monaco, C.; Zucchelli, G. Crown lengthening and restorative procedures in the esthetic zone. Periodontol. 2000 2018, 77, 84–92. [Google Scholar] [CrossRef]
- Ingber, J.S. Forced eruption I. A method of treating isolated one and two wall infrabony osseous defects-rationale and case report. J. Periodontol. 1974, 45, 199–206. [Google Scholar]
- Sabri, R. Principes et techniques [Crown lengthening by orthodontic extrusion. Principles and technics]. J. Parodontol. 1989, 8, 197–204. [Google Scholar]
- Minsk, L. Orthodontic tooth extrusion as an adjunct to periodontal therapy. Compend. Contin. Educ. Dent. 2000, 21, 768–770. [Google Scholar]
- Oesterle, L.J.; Wood, L.W. Raising the root. a look at orthodontic extrusion. J. Am. Dent. Assoc. 1991, 122, 193–198. [Google Scholar] [CrossRef]
- Nobre, C.M.; de Barros Pascoal, A.L.; Albuquerque Souza, E.; Machion Shaddox, L.; Dos Santos Calderon, P.; de Aquino Martins, A.R.; de Vasconcelos Gurgel, B.C. a systematic review and meta-analysis on the effects of crown lengthening on adjacent and non-adjacent sites. Clin. Oral Investig. 2017, 21, 7–16. [Google Scholar] [CrossRef]
- Faria, L.P.; Almeida, M.M.; Amaral, M.F.; Pellizzer, E.P.; Okamoto, R.; Mendonça, M.R. Orthodontic Extrusion as Treatment Option for Crown-Root Fracture: Literature Review with Systematic Criteria. J. Contemp. Dent. Pract. 2015, 16, 758–762. [Google Scholar]
- Buskin, R.; Castellon, P.; Hochstedler, J.L. Orthodontic extrusion and orthodontic extraction in preprosthetic treatment using implant therapy. Pract. Periodontol. Aesthet. Dent. 2000, 12, 213–220. [Google Scholar]
- Brown, I.S. the effect of orthodontic therapy on certain types of periodontal defects. I. Clinical findings. J. Periodontol. 1973, 44, 742–756. [Google Scholar] [CrossRef]
- Bach, N.; Baylard, J.F.; Voyer, R. Orthodontic extrusion: Periodontal considerations and applications. J. Can. Dent. Assoc. 2004, 70, 775–780. [Google Scholar]
- Smidt, A.; Gleitman, J.; Dekel, M.S. Forced eruption of a solitary nonrestorable tooth using mini-implants as anchorage: Rationale and technique. Int. J. Prosthodont. 2009, 22, 441–446. [Google Scholar]
- Barone, A.; Derchi, G.; Rossi, A.; Marconcini, S.; Covani, U. Longitudinal clinical evaluation of bonded composite inlays: A 3-year study. Quintessence Int. 2008, 39, 65–71. [Google Scholar]
- Dukic, W.; Dukic, O.L.; Milardovic, S.; Delija, B. Clinical evaluation of indirect composite restorations at baseline and 36 months after placement. Oper. Dent. 2010, 35, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Huth, K.C.; Chen, H.Y.; Mehl, A.; Hickel, R.; Manhart, J. Clinical study of indirect composite resin inlays in posterior stress-bearing cavities placed by dental students: Results after 4 years. J. Dent. 2011, 39, 478–488. [Google Scholar] [CrossRef]
- Manhart, J.; Chen, H.Y.; Neuerer, P.; Scheibenbogen-Fuchsbrunner, A.; Hickel, R. Three-year clinical evaluation of composite and ceramic inlays. Am. J. Dent. 2001, 14, 95–99. [Google Scholar]
- Thordrup, M.; Isidor, F.; Hörsted-Bindslev, P. a prospective clinical study of indirect and direct composite and ceramic inlays: Ten-year results. Quintessence Int. 2006, 37, 139–144. [Google Scholar]
- Leirskar, J.; Nordbø, H.; Thoresen, N.R.; Henaug, T.; von der Fehr, F.R. a four to six years follow-up of indirect resin composite inlays/onlays. Acta Odontol. Scand. 2003, 61, 247–251. [Google Scholar] [CrossRef]
- Li, H.; Burrow, M.F.; Tyas, M.J. Nanoleakage patterns of four dentin bonding systems. Dent. Mater. 2000, 16, 48–56. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; De Munck, J.; Vanloy, A.; Declerck, D.; Lambrechts, P.; Peumans, M.; Teughels, W.; Van Meerbeek, B.; Van Landuyt, K.L. Secondary caries: Prevalence, characteristics, and approach. Clin. Oral. Investig. 2020, 24, 683–691. [Google Scholar] [CrossRef]
- Flores-de-Jacoby, L.; Zafiropoulos, G.G.; Ciancio, S. Effect of crown margin location on plaque and periodontal health. Int. J. Periodontics Restorative Dent. 1989, 9, 197–205. [Google Scholar]
- Kemp-Scholte, C.M.; Davidson, C.L. Marginal integrity related to bond strength and strain capacity of composite resin restorative systems. J. Prosthet. Dent. 1990, 64, 658–664. [Google Scholar] [CrossRef]
- Cavalcanti, A.N.; Mitsui, F.H.; Ambrosano, G.M.; Marchi, G.M. Influence of adhesive systems and flowable composite lining on bond strength of class II restorations submitted to thermal and mechanical stresses. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 80, 52–58. [Google Scholar] [CrossRef]
- Castañeda-Espinosa, J.C.; Pereira, R.A.; Cavalcanti, A.P.; Mondelli, R.F. Transmission of composite polymerization contraction force through a flowable composite and a resin-modified glass ionomer cement. J. Appl. Oral Sci. 2007, 15, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Litonjua, L.A.; Andreana, S.; Bush, P.J.; Tobias, T.S.; Cohen, R.E. Noncarious cervical lesions and abfractions: A re-evaluation. J. Am. Dent. Assoc. 2003, 134, 845–850. [Google Scholar] [CrossRef]
- Agarwal, R.S.; Hiremath, H.; Agarwal, J.; Garg, A. Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: An in vitro study. J. Conserv. Dent. 2015, 18, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Francis, A.V.; Braxton, A.D.; Ahmad, W.; Tantbirojn, D.; Simon, J.F.; Versluis, A. Cuspal Flexure and Extent of Cure of a Bulk-fill Flowable Base Composite. Oper. Dent. 2015, 40, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, A.; Hogg, C.H.; Dowling, A.H.; Grufferty, B.F.; Benetti, A.R.; Fleming, G.J. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J. Dent. 2012, 40, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Kamath, U.; Sheth, H.; Vigneshwar, *!!! REPLACE !!!*. Role of delayed light polymerization of a dual-cured composite base on marginal adaptation of class II posterior composite open-sandwich restoration. Indian J. Dent. Res. 2012, 23, 296. [Google Scholar]
- Rodrigues Junior, S.A.; Pin, L.F.; Machado, G.; Della Bona, A.; Demarco, F.F. Influence of different restorative techniques on marginal seal of class II composite restorations. J. Appl. Oral Sci. 2010, 18, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Chang, Y.H.; Chang, C.Y.; Pai, C.A.; Huang, S.F. Finite element and Weibull analyses to estimate failure risks in the ceramic endocrown and classical crown for endodontically treated maxillary premolar. Eur. J. Oral Sci. 2010, 118, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Eraslan, Ö.; Eraslan, O.; Eskitaşcıoğlu, G.; Belli, S. Conservative restoration of severely damaged endodontically treated premolar teeth: A FEM study. Clin. Oral Investig. 2011, 15, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature—Part 1. Composition and micro- and macrostructure alterations. Quintessence Int. 2007, 38, 733–743. [Google Scholar]
- ElAyouti, A.; Serry, M.I.; Geis-Gerstorfer, J.; Löst, C. Influence of cusp coverage on the fracture resistance of premolars with endodontic access cavities. Int. Endod. J. 2011, 44, 543–549. [Google Scholar] [CrossRef]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature, Part II (Evaluation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int. 2008, 39, 117–129. [Google Scholar]



{kind=link}
{kind=link}
| Authors, Year of Publication | Type of Study | Investigated Factors | Study Design/Methodology | Summary of Findings |
|---|---|---|---|---|
| Dietschi et al., 1998 [1] | Review | - | Described the procedures used for adhesive cementation of different types of posterior restorations. | Application of composite layer in the base of the proximal cavity under rubber dam isolation for DME is possible. |
| Magne et al., 2012 [2] | Review | - | An in-depth explanation of the DME technique. | Deep margin elevation can be a less invasive alternative compared with surgical crown lengthening. |
| Juloski et al., 2018 [3] | Review1234567 | - | Discussed the effect of DME on marginal adaptation, fracture resistance, and bond strength. | No evidence of a difference in marginal quality in raised and non-raised margins. No difference in fracture resistance values among DME groups regardless of the restoration type used. With regard to bond strength, higher results were obtained with raised margins. The current evidence is not strong enough to encourage or discourage the use of DME. |
| Binalrimal et al., 2021 [4] | Cross-sectional | Knowledge, attitude, and practice regarding DME among dental practitioners. | Assessed the knowledge of dental practioners regarding DME and the relation between years of experience and DME knowledge. | Adequate knowledge among practitioners was observed with regard to DME. |
| Sarfati et al., 2018 [5] | Review and case report | - | Compared the outcomes of SCL versus DME and the periodontal response to different restorative materials. | Similar results were seen in DME and SCL regarding BoP, with higher CAL values in SCL, suggesting the well tolerance of DME by the periodontium. |
| Kielbassa et al., 2015 [6] | Systematic review and case report | Fracture resistance and marginal integrity. | Evaluated in vitro studies and randomized controlled trials on DME. | Fracture resistance was improved by applying flowable composite liner in class II amalgam restorations. With regard to marginal integrity, the preferred base material is controversial. |
| Veneziani et al., 2010 [8] | Review | - | Discussed different treatment approaches for posterior teeth with sub-gingival margins. | A new classification was established based on operative and biological parameters for dealing with sub-gingival margins. |
| Ferrari et al., 2018 [9] | Controlled trial | Periodontal health | Assessed the effect of DME on periodontal health. A 12-month controlled trial was obtained to assess GI, PI, and BoP in teeth restored with DME. A total of 35 teeth were divided into two groups: (G1) DME and (G2) shoulder preparation without DME. For DME, G-Premio bond and resin composite were used. Lithium disilicate crowns were luted. | A higher incidence of BoP was noticed in teeth treated with DME when margins are closer than 2 mm to the alveolar crest. No significant difference was found in GI and PI between both groups. |
| Da Silva et al., 2021 [11] | In vitro | Marginal seal | Assessed the effect of margin location and adhesive strategy of DME technique on the marginal seal of resin composite inlays. MOD cavities on 12 third molars were prepared and divided into six groups based on margin location and type of adhesive used as follow: (G1) Enamel + ERA (SB1XT), (G2) Dentin + ERA (SB1XT), (G3) DME + ERA (SB1XT), (G4) Enamel + SEA with enamel selective etching Clearfil SE Bond (CSE), (G5) Dentin + SEA, (G6) DME + SEA. Resin composite inlay bonded with conventional dual-cure resin. | SEA showed better sealing ability than the ERA when DME was applied or when margins were located sub-gingivally. Hermetic seal can be achieved whenever enamel margin is present with the use of selective enamel etching, regardless of the type of adhesive. |
| Ilgenstein et al., 2014 [12] | In vitro | Marginal quality and fracture behavior. | Assessed the marginal quality and fracture behavior of root filled molars restored with CAD/CAM fabricated ceramic and composite onlays. A total of 48 MOD cavities with distal margins 2 mm below CEJ were prepared. Proximal box elevation to CEJ with composite resin prepared in (G1+ G2), no elevation was prepared in (G3+ G4). CAD-CAM fabricated restorations with feldspathic ceramic in (G1 + G3) and resin nano-ceramic in (G2 + G4). | Marginal integrity and fracture resistance were not affected by DME. |
| Grubbs et al., 2020 [13] | In vitro | Marginal quality and fracture resistance | Assessed the effect of restorative material type used in DME on the marginal quality and fracture resistance of CAD/CAM fabricated onlays. A total of 75 MOD specimens prepared by CAD-CAM divided into five groups depending on the type of material used for margin elevation: (G1) type II GI, (G2) type II RMGI, (G3) RBC, (G4) BF RBC, (G5) a control with no box elevation procedure. | Restorative materials have no effect on marginal quality nor fracture resistance. |
| Da Silva Gonçalves et al., 2017 [14] | In vitro | Bond strength | Assessed the effects of DME on bond strength of composite inlays. Class II cavities were prepared in 25 molars and divided into four groups: (G1) RelyX ARC, without DME, (G2) RelyX ARC with DME, (G3) G-Cem without DME, (G4) G-Cem with DME. | In the case where DME was applied and G-Cem resin cement was used, the bond strength of composite inlays was significantly increased. When DME technique was applied and RelyX ARC cement was used, the bond strength was not affected. |
| Roggendorf et al., 2012 [15] | In vitro | Marginal quality | 40 MOD cavities were raised 3 mm with one of the following materials: (G1) G-Cem, (G2) Maxcem Elite (G3 + G4) Clearfil Majesty Posterior in one or three layers, respectively, (G5) untreated “control”, then restored with resin composite inlays. | Multi-layered DME is highly effectual in bonding indirect resin composite to deep proximal boxes. Self-adhesive cement proved unsuitable for this technique. |
| Spreafico et al., 2016 [16] | In vitro | Marginal quality | A total of 40 molars with standard crown preparations with non-raised distal margins located in enamel as a control group. Mesial margins were located 2 mm below CEJ and raised using: (G1) Filtek Flow Supreme XTE and LAVA ultimate, (G2) Filtek Supreme XTE and LAVA Ultimate, (G3) Filtek Flow Supreme XTE and IPS e-max, (G4) Filtek Supreme XTE and IPS e-max.1234567 | DME has no effect with regard to marginal integrity. |
| Frankenberger et al., 2013 [17] | In vitro | Marginal quality | A total of 48 MOD cavities were raised 3 mm with one of the following materials: (G1) G-Cem, (G2) Maxcem Elite (G3 + G4) Clearfil Majesty Posterior in one or three layers respectively, (G5) untreated “control”, then restored with ceramic inlays. | DME aided the bonding of ceramics to deep cervical margins. The best marginal quality was obtained by 3 layers of DME. Self-adhesive cement proved unsuitable for this technique. |
| Zaruba et al., 2012 [18] | In vitro | Marginal adaptation | A total of 40 MOD cavities distributed into four groups: (G1) enamel margins, (G2-4) margins 2 mm below CEJ, (G2) one 3 mm layer DME, (G3) two 1.5 mm layers DME, (G4) left untreated. Ceramic inlays were bonded to all groups | DME does not affect the marginal integrity of ceramic inlays. |
| Dietschi et al., 2015 [19] | Review | - | Presented a treatment protocol for dealing with bonded inlays and onlays. | DME will ease isolation, impression taking, cementation procedures, and finishing of the margins. |
| Rocca et al., 2015 [20] | Review | - | Presented evidence-based concepts and procedures for bonded inlays and onlays. | With regard to DME, the minimum thickness needed for locating the margin supragingivally was 1–1.5 mm. |
| Müller et al., 2017 [21] | In vitro | Marginal integrity | Assessed the effect of deep margin elevation on the marginal integrity of teeth restored with adhesively bonded cerec inlays in 24 molar teeth with MOD cavities extending to CEJ. DME was prepared on one of the proximal boxes using Filtek Supreme. The sample was further divided into three groups: (G1) inlays luted using Scotchbond Universal and Rely X Ultimate, (G2) inlays luted using Monobond Plus, Syntac, and Variolink II, (G3) inlays luted using Clearfil Ceramic Primer and Panavia SA Cement. | Similar marginal integrity between teeth restored with DME and teeth with inlays directly bonded to dentin. |
| Köken et al., 2018 [22] | In vitro | Marginal sealing | Assessed the effect of DME using hybrid composite and flowable composite on the marginal sealing of CAD/CAM MOD overlays. MOD cavities in 39 molars with a 1 mm sub-gingival margin on the mesial side, the sample was divided into three groups: (G1) = DME using Hybrid composite (GC Essentia MD), (G2) = DME using Flowable composite (GC G-aenial Universal Flo), and (G3) = no DME was prepared. | In the DME groups (1 + 2), the marginal sealing ability of both types of composites was comparable. Bonding CAD/CAM overlays directly to dentin without DME showed better marginal sealing. |
| Marchesi et al., 2014 [23] | In vitro | Marginal integrity | Assessed the effect of DME using Optibond FL and Filtek Supreme XTE flow on the marginal integrity of CAD/CAM fabricated lithium disilicate crowns. | DME does not affect marginal integrity. |
| Lefever et al., 2012 [24] | In vitro | Marginal adaptation | A total of 88 molars with a standardized box cavity where margins are located below CEJ were distributed into 11 groups according to the type of restorative materials and adhesive systems used as follows: (G1) Filtek Silorane, (G2) Clearfil AP-X, (G3) Clearfil Majesty Posterior, (G4) Filtek Silorane, (G5) Filtek Silorane, (G6) Clearfil AP-X, (G7) Clearfil Majesty Posterior, (G8) Vertise Flow, (G9) Clearfil Majesty Flow, (G10) RelyX Unicem, (G11) SDR. The adhesive systems used were: (G1–G3) Filtek Silorane Primer + bond, (G4–G7 and G9 + G11) Clearfil Protect Bond, and (G8 + G10) no adhesive was used. | Using different materials for relocating sub-gingival margins can have different results in marginal integrity. |
| Bresser et al., 2020 [25] | In vitro | Fracture strength | Assessed the effect of DME and preparation geometry on the fracture strength of CAD/CAM fabricated lithium disilicate restorations. A total of 60 extracted molars were randomly assigned to one of four groups: (G1) inlay without DME, (G2) inlay with DME, (G3) onlay without DME, and (G4) onlay with DME. Aging and occlusal stressing were applied to all samples. | DME did not affect the fracture strength of lithium disilicate restorations, while cuspal coverage increased the fracture strength. |
| Dietschi et al., 2003 [26] | In vitro | Marginal and internal adaptation. | Compared the marginal and internal adaptation of fine hybrid composite onlays with and without DME after occlusal stressing. A total of 40 molars were prepared with proximal boxes extending into the cervical margins. The type of restorative materials used for bases was as follows: Revolution (Kerr), Tetric flow (Vivadent), Dyract (Detery-Dentsply), and Prodigy (Kerr). | The bonding of inlays can be influenced by the physical properties of materials, and flowable composites can be used for relocating the margins. |
| Juloski et al., 2020 [27] | In vitro | Marginal quality | Assessed the marginal quality of 14 molars prepared for MOD cavities with proximal margins located in dentin. All the mesial proximal boxes were elevated and further divided into two groups depending on the type of material used: (G1) TEA and flowable composite, (G2) UA and bulk-fill flowable composite. The distal proximal boxes were not elevated. | Placing the restoration directly to dentin without DME showed better marginal sealing. In addition, the type of restorative material used affects the marginal sealing. |
| Alhassan et al., 2020 [28] | Case report | - | Reported a case with deep proximal cavities treated using DME. | Whenever adequate isolation and feasible matrix placement can be achieved, DME can be used. |
| Bertoldi et al., 2019 [29] | Clinical study | Clinical and histological response. | Assessed the response of periodontal tissues to sub-gingival restorations when compared with untreated root surfaces. DME was applied on 29 teeth with sub-gingival cavities. | With respect to biological width and following a firm supportive therapy, DME is compatible with periodontal tissues. |
| Frese et al., 2014 [30] | Review and case report | - | Presented a step-by-step technique for DME in a case where biological width was invaded. | The 12-month follow-up period showed no signs of hard or soft tissue inflammation. |
| Dablanca-Blanco et al., 2017 [31] | Case reports | - | Discussed seven different scenarios of molars with deep sub-gingival margins, their treatment approaches, and the indication for DME vs. SCL. | Whenever optimal matrix placement can be achieved, the DME technique can be used. Otherwise, in deeper cavities that invades the BW, SCL is recommended. |
| Mugri et al., 2021 [32] | Systematic review | Survival rate | Compared the survival rate of teeth restored with SCL versus DME. | A higher long-term predictability of teeth treated using SCL was noticed. However, the survival ratio of DME treated teeth was higher than SCL. |
| Vertolli et al., 2020 [33] | In vitro | Structural and marginal integrity | Assessed the effects of DME on the structural and marginal integrity of teeth restored using CAD/CAM fabricated ceramic inlays. A total of 40 molars were separated into four groups as follows: (G1) enamel margins, (G2) margins 2 mm below CEJ, (G3) margins 2 mm below CEJ and elevated with GIC, (G4) margins 2 mm below CEJ and elevated with RMGI. The class II inlays were bonded to all teeth. | Margins placed in cementum had a higher ceramic fracture rate and DME was not affected by the type of restoration GI or RMGI. |
| Zhang et al., 2021 [34] | In vitro | Fracture resistance and microleakage | Assessed the effects of DME on the fracture resistance and microleakage of teeth restored using ceramic endocrowns. | Fracture resistance in raised margins had higher values in comparison with non-raised margins. |
| Grade I | On placement of rubber dam in the gingival sulcus, the cervical margin can be adequately visible. |
| Grade II | A rubber dam is not sufficient to isolate the field, yet biological width is respected. |
| Grade III | Deep sub-gingival margins violating the biological width. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldakheel, M.; Aldosary, K.; Alnafissah, S.; Alaamer, R.; Alqahtani, A.; Almuhtab, N. Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review. Medicina 2022, 58, 1482. https://doi.org/10.3390/medicina58101482
Aldakheel M, Aldosary K, Alnafissah S, Alaamer R, Alqahtani A, Almuhtab N. Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review. Medicina. 2022; 58(10):1482. https://doi.org/10.3390/medicina58101482
Chicago/Turabian StyleAldakheel, Majed, Khalid Aldosary, Shatha Alnafissah, Rahaf Alaamer, Anwar Alqahtani, and Nora Almuhtab. 2022. "Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review" Medicina 58, no. 10: 1482. https://doi.org/10.3390/medicina58101482