2. Case Report
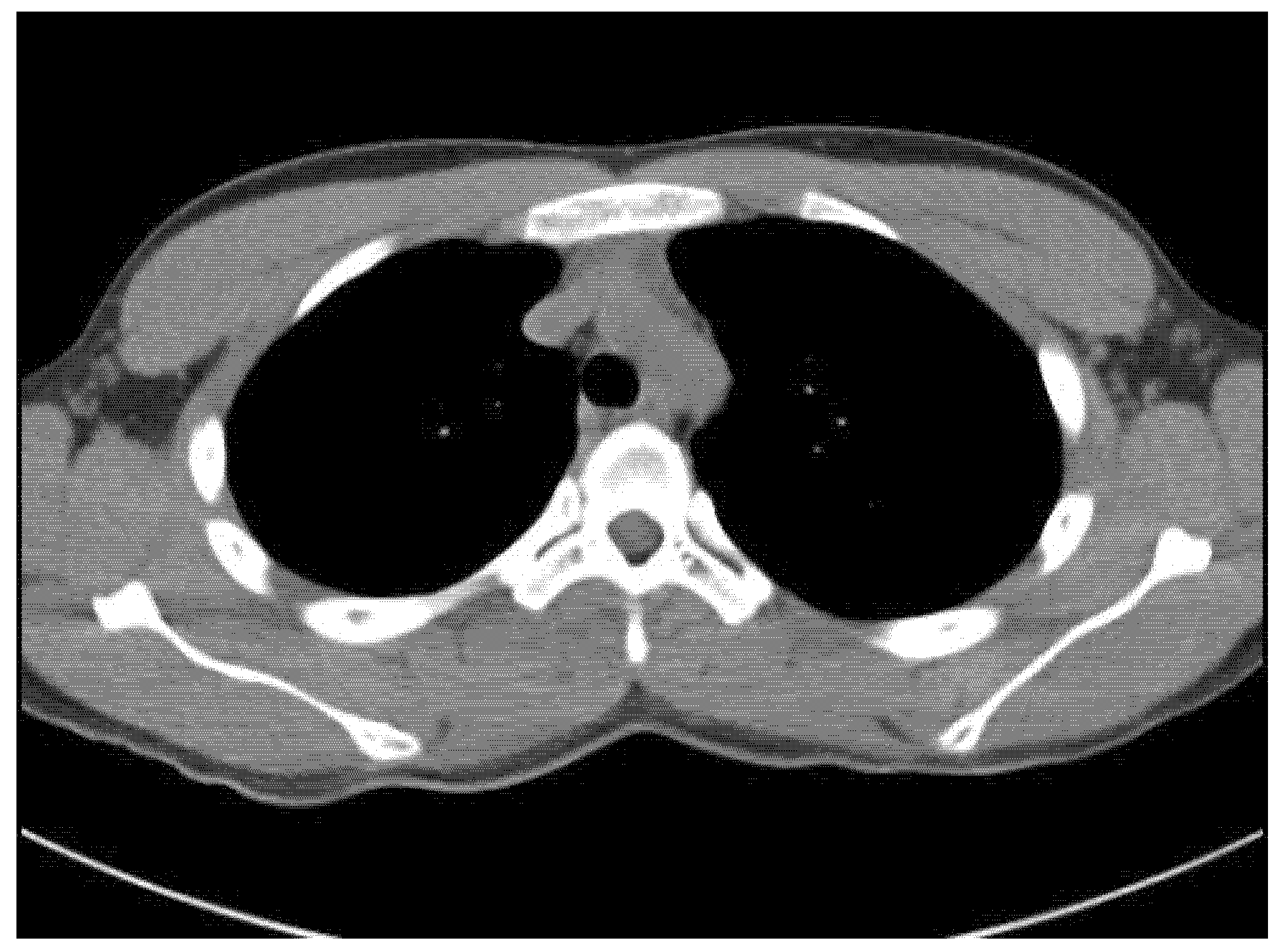
An 18-year-old male student came to our spine center complaining of aggravating right back pain that had started 5 months ago, along with swelling of the mid-thoracic level. At a local hospital, he underwent a chest and heart computed tomography exam for the evaluation of chest and back pain, but there were no abnormal findings on the images (
Figure 1). The physician did extracorporeal shock wave therapy at his trunk for the treatment of vague pain about 6 weeks before visiting our institution. He explained that after the extracorporeal shock wave therapy, the back pain worsened, and swelling at the site of pain was found.
There was no specific finding in his medical history. However, physical examination revealed a firmly palpable, not movable, and clearly demarcated mass at the posterior mid-thoracic level with tenderness. Laboratory data were within the normal range, including C-reactive protein, erythrocyte sedimentation rate, and white blood cell counts.
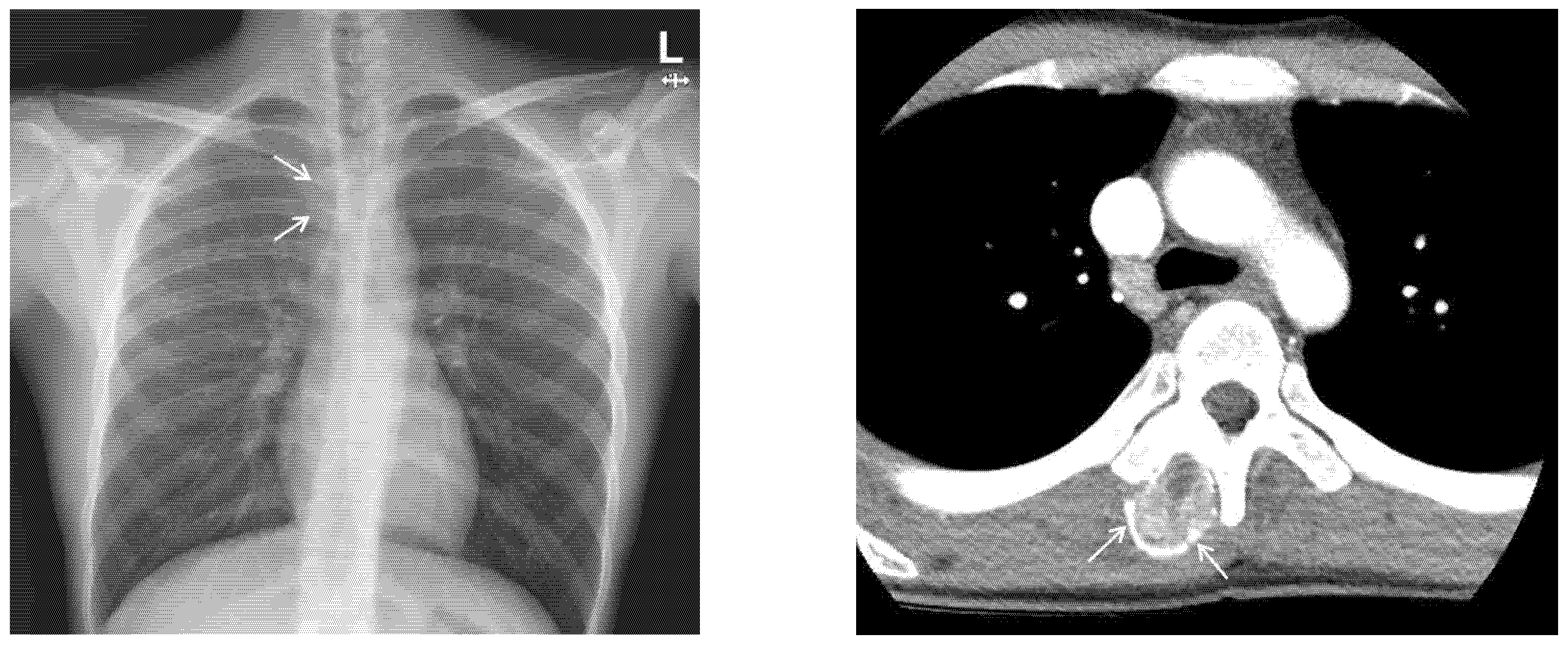
Chest X-ray images showed a radiopaque mass with rim calcification at the T4/5 paraspinal area (
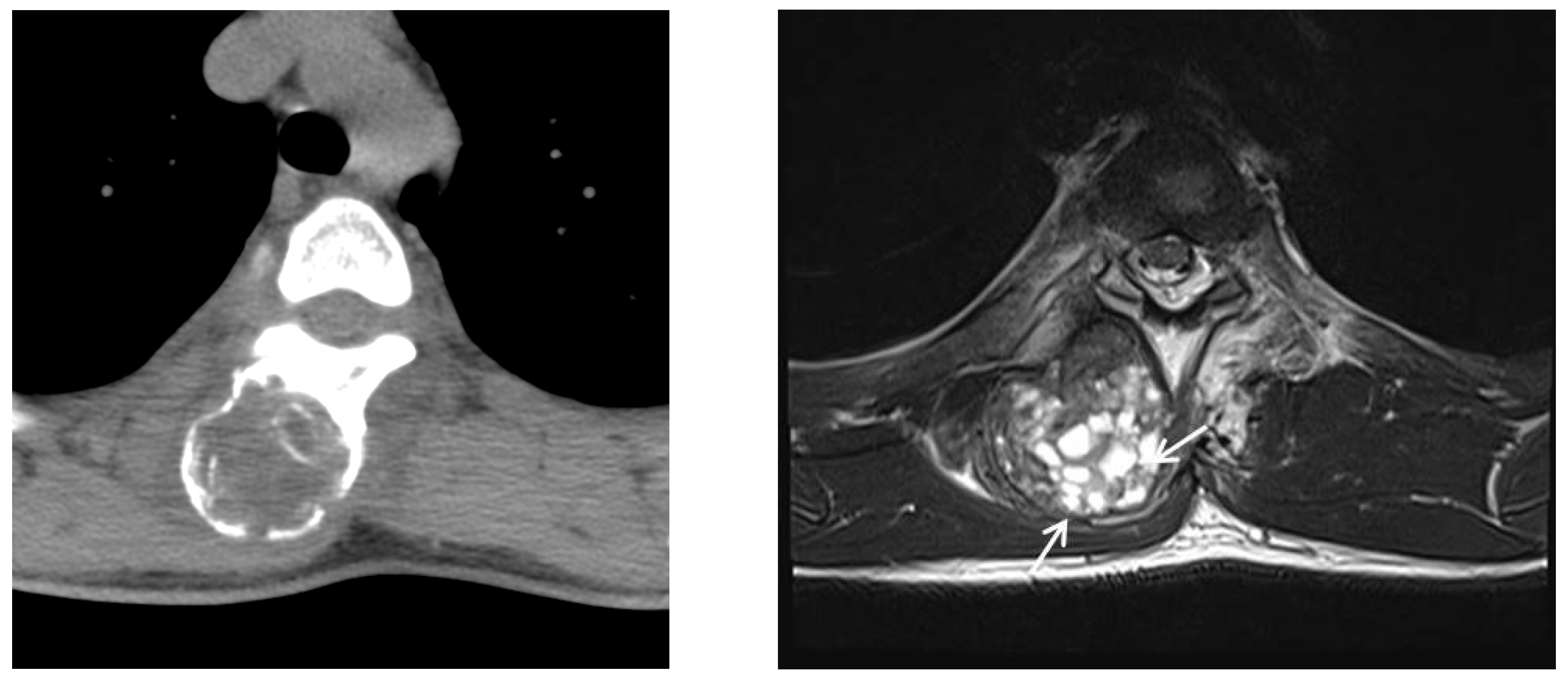
Figure 2). Computed tomography images revealed an approximately 2.8 × 2.5 cm wide, 4.5 cm high oval-shaped mass in the right paraspinal muscle with peripheral rim calcification (
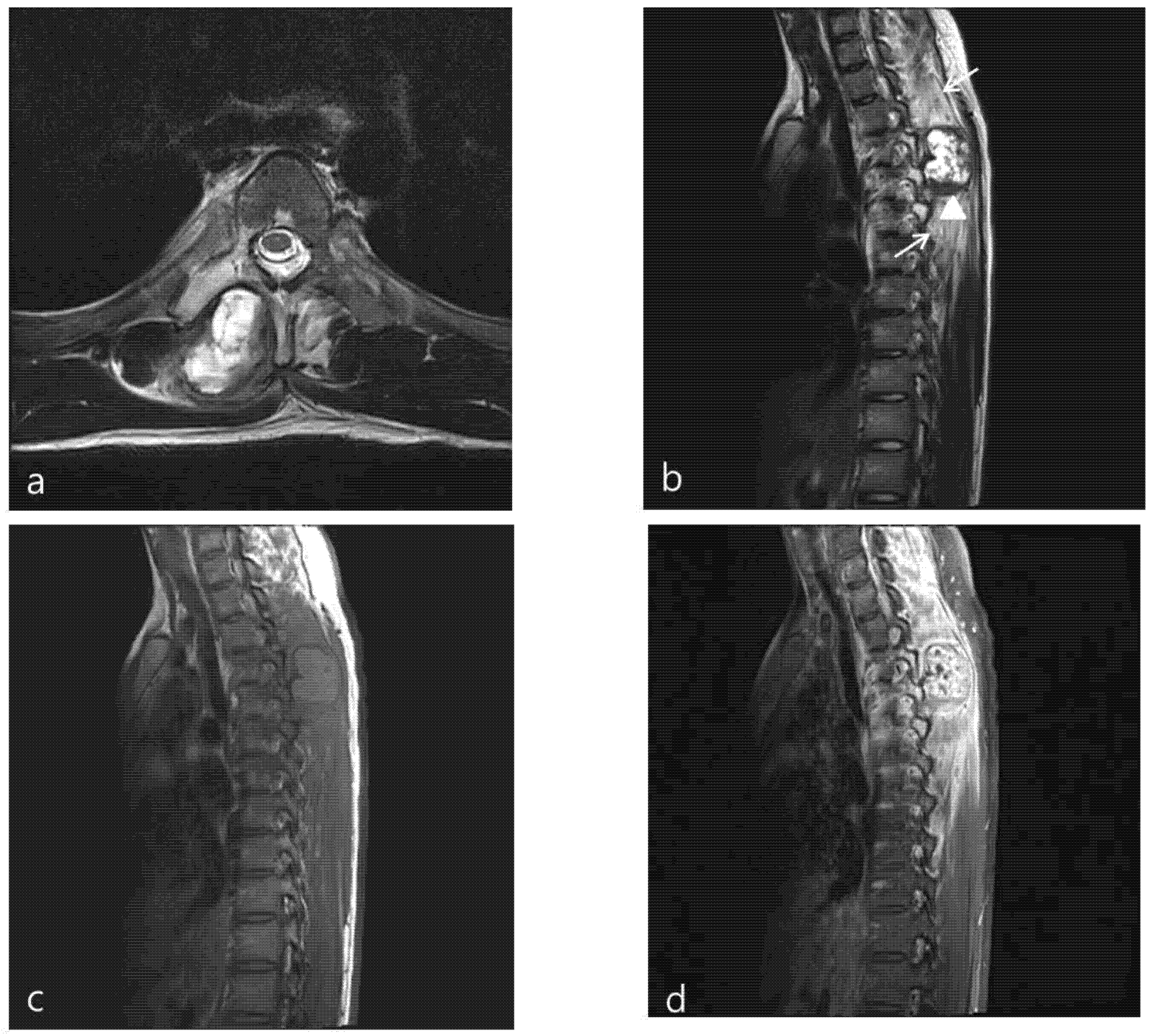
Figure 2) that was not seen on computed tomography images 5 months prior. The cleft between the mass and the adjacent bone was visible. On magnetic resonance imaging (MRI), the mass showed a heterogeneous high signal intensity on T2WI, isointense to muscle on T1WI with a peripheral low signal intensity rim, and homogeneous enhancement. In addition, perilesional soft tissue edema at the adjacent muscle was also noted (
Figure 3). With a history of suspicious trauma (extracorporeal shock wave therapy) and radiologic findings, myositis ossificans was the most suspected diagnosis.
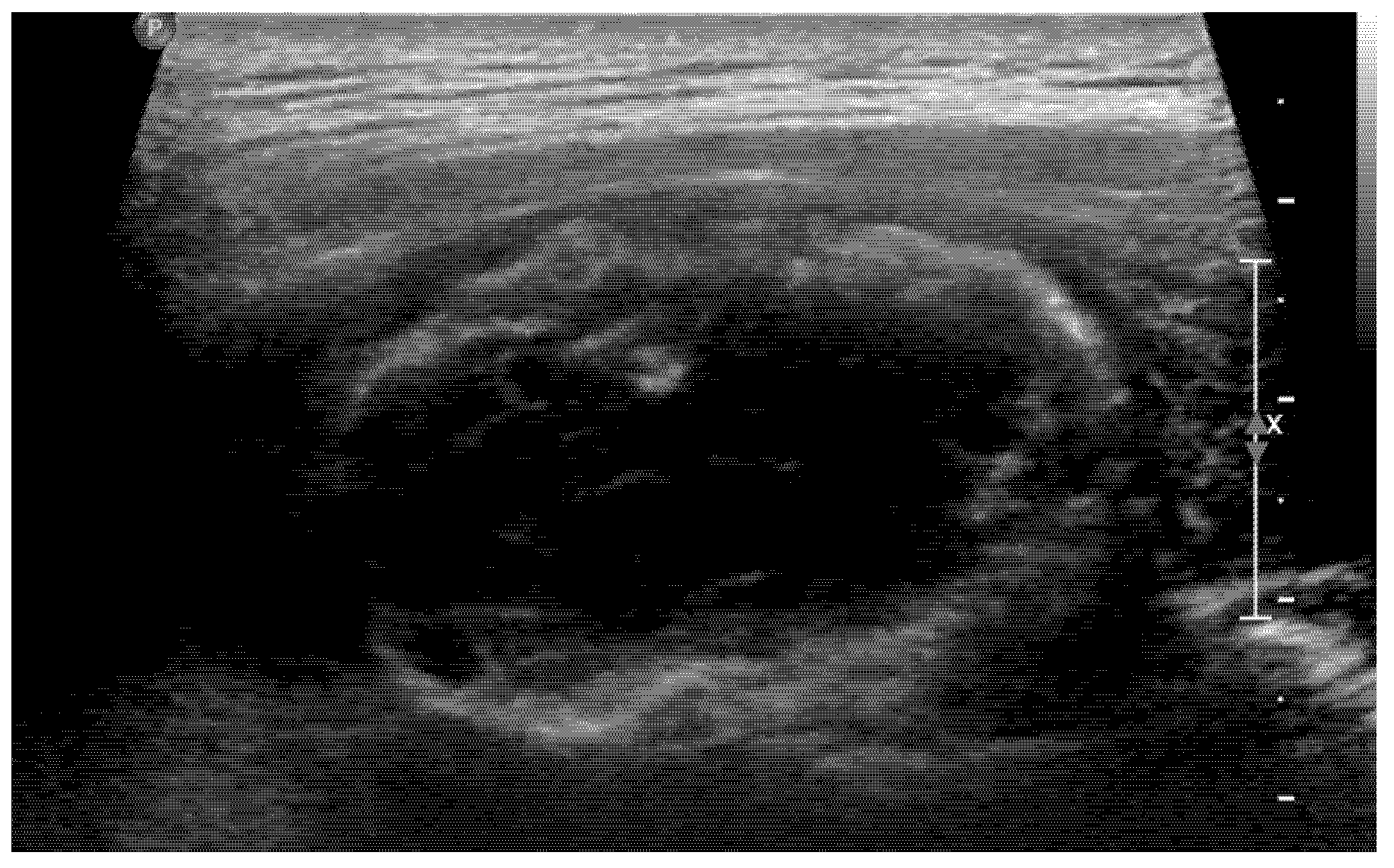
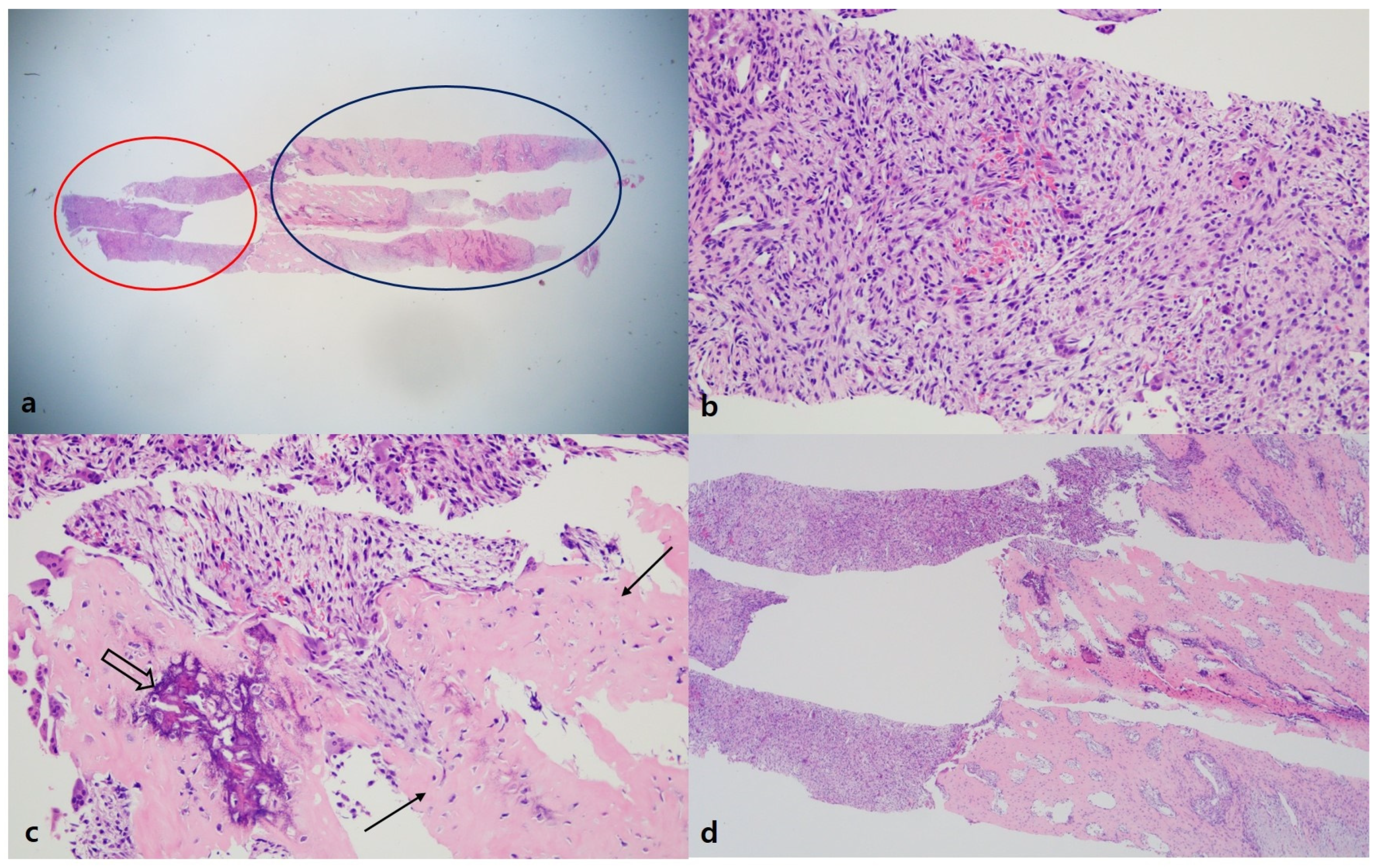
Usually, we do not perform a biopsy when MO is suspected. However, in this case, the patient’s symptoms worsened, and its location was unusual for MO, so both the clinician and patient strongly wanted to perform a biopsy. Therefore, to confirm the diagnosis and exclude the possibility of malignancy, we decided to perform a US-guided biopsy. In the US, hyperechoic peripheral rim calcification with posterior shadowing was noted (
Figure 4). A US-guided needle biopsy was performed, and the pathological report confirmed myositis ossificans with zone phenomenon (
Figure 5).
We decided to discharge and observe the patient without surgical intervention. However, follow-up thoracic spine computed tomography, 5 months after the biopsy, showed the lesion was larger than was seen on previous computed tomography (
Figure 6). Moreover, the patient still complained about persistent back pain. Follow-up magnetic resonance imaging (MRI) revealed an increased size of the mass (2.8 × 2.5 × 4.5 cm → 4.3 × 4.2 × 6.3 cm) and multiple new small cystic lesions with a fluid–fluid level in the mass. Those findings suggested aneurismal bone cystic change. Furthermore, perilesional soft tissue edema of adjacent muscle was still noted (
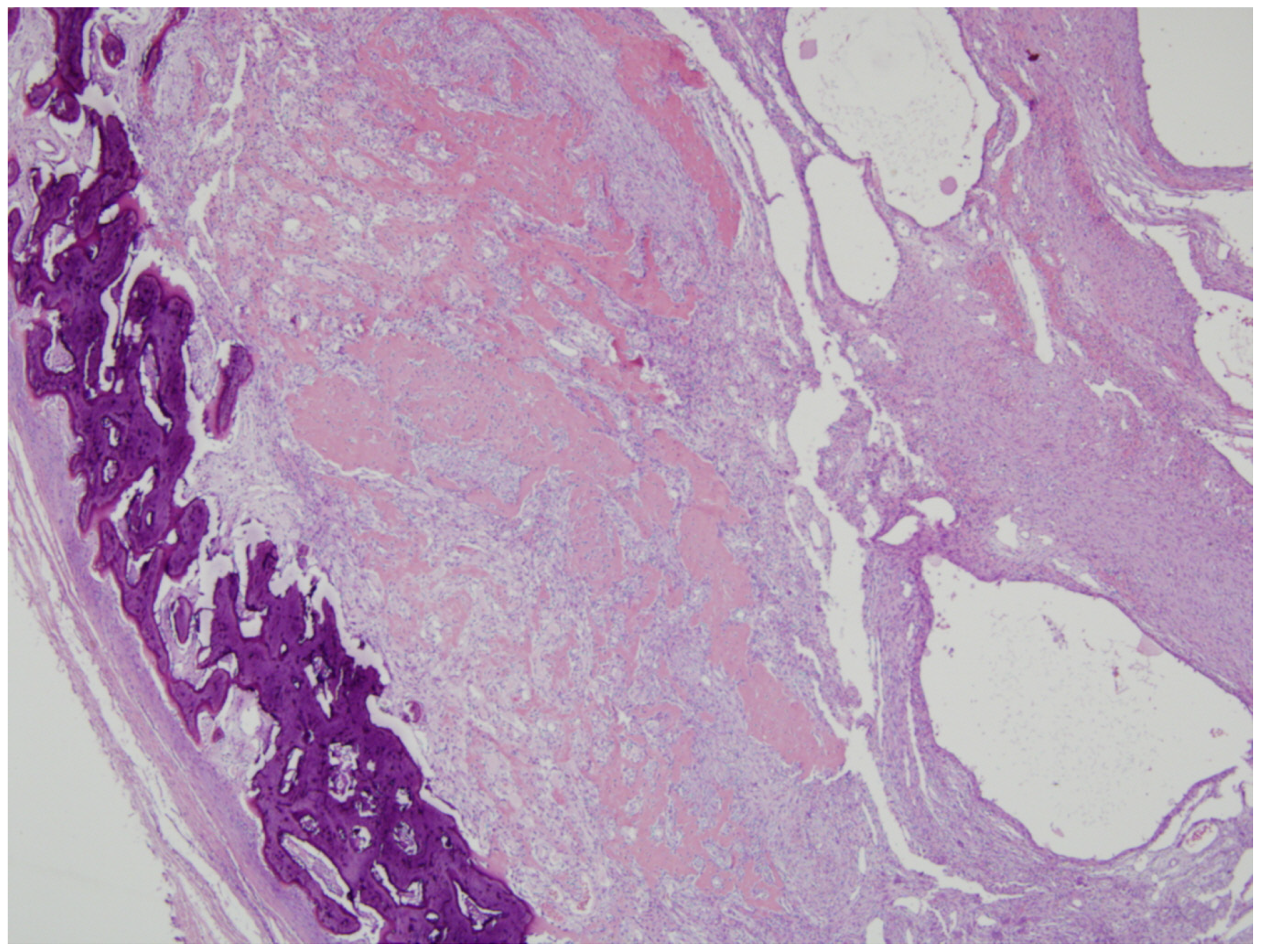
Figure 6). Because the mass did not follow the natural history of myositis ossificans, considered the possibility of a malignant tumor, such as extraskeletal osteosarcoma or parosteal osteosarcoma. So, we performed surgical excision through the posterior approach. A midline vertical incision that extended between the spinous processes of the T4 to T5 vertebrae was made. Above the left spinous process, lamina, and transverse process of T4 and T5, a well-circumscribed, gray-yellow colored, and peripheral calcified mass with gritty areas was located. The mass was somewhat fused to the left spinous process, lamina, and transverse process of T4 andT5. So, the mass was near-totally removed. On histologic exam, the lesion showed a central cellular spindle cells area associated with immature woven bone formation and more organized mature lamellar bone at the periphery that was consistent with myositis ossificans, and extensive aneurysmal bone cystic changes were also seen in the mass (
Figure 7). The patient had no neurological deficits after surgical treatment. Unfortunately, the patient’s back pain had not completely disappeared, but the symptom gradually improved over a period of several months. The patient had an annual follow-up about 2 years later, and there was no evidence of recurrence of MO in the same location, and symptoms improved.
3. Discussion
Myositis ossificans (MO) is a benign, localized heterotopic bone formation in soft tissues, especially muscles. Although the pathophysiologic factors of myositis ossificans are not well known, an inciting event and signaling agents such as bone morphogenic protein (BMP) play an important role in the formation of heterotopic bone [
1]. There are two different types of MO, including genetic form and acquired form. Several genetic diseases are associated with heterotopic ossification at multiple sites, including fibrodysplasia ossificans progressiva (FOP), progressive osseous heteroplasia (POH), and Albright’s hereditary osteodystrophy (AHO) [
4]. Nongenetic forms are triggered by trauma or injury, including myositis ossificans traumatica (MOT) and neurogenic heterotopic ossification (NHO) [
4]. The types of trauma include blunt trauma, penetrating wounds, fractures, dislocations, or surgical incisions [
5]. Possible nontraumatic sources of provocation include infection, burns, neuromuscular disorders, hemophilia, and drug abuse [
6]. There is also a report about an unusual cause of MOT, such as acupuncture [
7], but there was no report that stated the cause of MOT was extracorporeal shock wave therapy. Usually, extracorporeal shock wave therapy does not cause the formation of MO, and it is even used as a treatment for post-traumatic MO [
8] In our case, the site of the lesion was not the usual location of MOT. MOT can occur anywhere in the body; however, it usually occurs in the extremities, which are prone to trauma. The paraspinal muscle, as in our case, was reported as a rare site of MOT in some case reports [
2,
7], and most of the lesions occurred atraumatically.
The usual, natural course of MO is as follows: One or two days after trauma, a painful, tender soft tissue mass appears, which may be associated with a periosteal reaction in 7–10 days. An ossification pattern may be seen on computed tomography as early as in 2 weeks. Flocculent dens lesions arise in the mass from 2 to 6 weeks after trauma. The dense calcific areas gradually increase in size, and circumscribed peripheral calcification may be seen within a week. Maturity is reached in 5–6 months, and the lesion then shrinks [
5]. Unlike the natural course of other MO, in our case, the lesion increased in size after 5 months. Because we knew the histologic result was MO, we expected the lesion would regress after 5 to 6 months. However, the lesion showed an increase in size, and the imaging represented a change inside the lesion. Sometimes, it is difficult to differentiate between MO and sarcomas since these two diseases have similar imaging findings. Łuczyńska E. et al. [
9] attempted to differentiate MO from parosteal osteosarcoma, synovial sarcoma, and malignant fibrous histiocytoma. The important points for differentiation are the presence of bone erosion or destruction and the appearance of calcification. Bone erosion or destruction may be seen in sarcomas; however, it is rare in MO. In MO, calcification is usually seen in the periphery of the lesion, whereas in parosteal osteosarcoma, it is seen more centrally [
9]. In our case, there was no evidence of bone erosion or destruction, and calcification was seen in the periphery of the mass. Therefore, radiologically it was more likely MO rather than sarcomas. However, considering the unusual course of progression and the few cases that were reported about the evolution to osteosarcoma from MO [
10], we decided to perform an excision.
The reason for the increase in the size of the lesion was explained by the pathologic result of the excised specimen. The pathologic report represented an aneurysmal bone cystic change of the previously confirmed MO. A correlative case with our case was reported in 1992 by Amir et al. [
11]. In that case, MO that occurred around the hip joint doubled in size after open biopsy, and the excised lesion was interpreted as myositis ossificans with aneurysmal bone cyst-like (ABC) changes. They emphasized that the trauma associated with the first biopsy could have initiated the formation of a hematoma in MO, and ABC-like changes in the center of the MO can be explained in terms of cystic degeneration of the hematoma. In our case, the needle biopsy can be a causative factor of hematoma formation in MO, and this could be an ABC-like change. Thus, we can learn from our case that if a lesion is thought to be MO, a needle biopsy should not be attempted to avoid the aggravation of the lesion.
In summary, this is a very rare case of MO that showed an unusual cause, location, clinical course, and pathologic result on follow-up. This can be an instructive case for radiologists as it is a common disease entity with unusual manifestations.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






