
Risk Factors for Delayed Diagnosis of Acute Cholecystitis among Rural Older Patients: A Retrospective Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
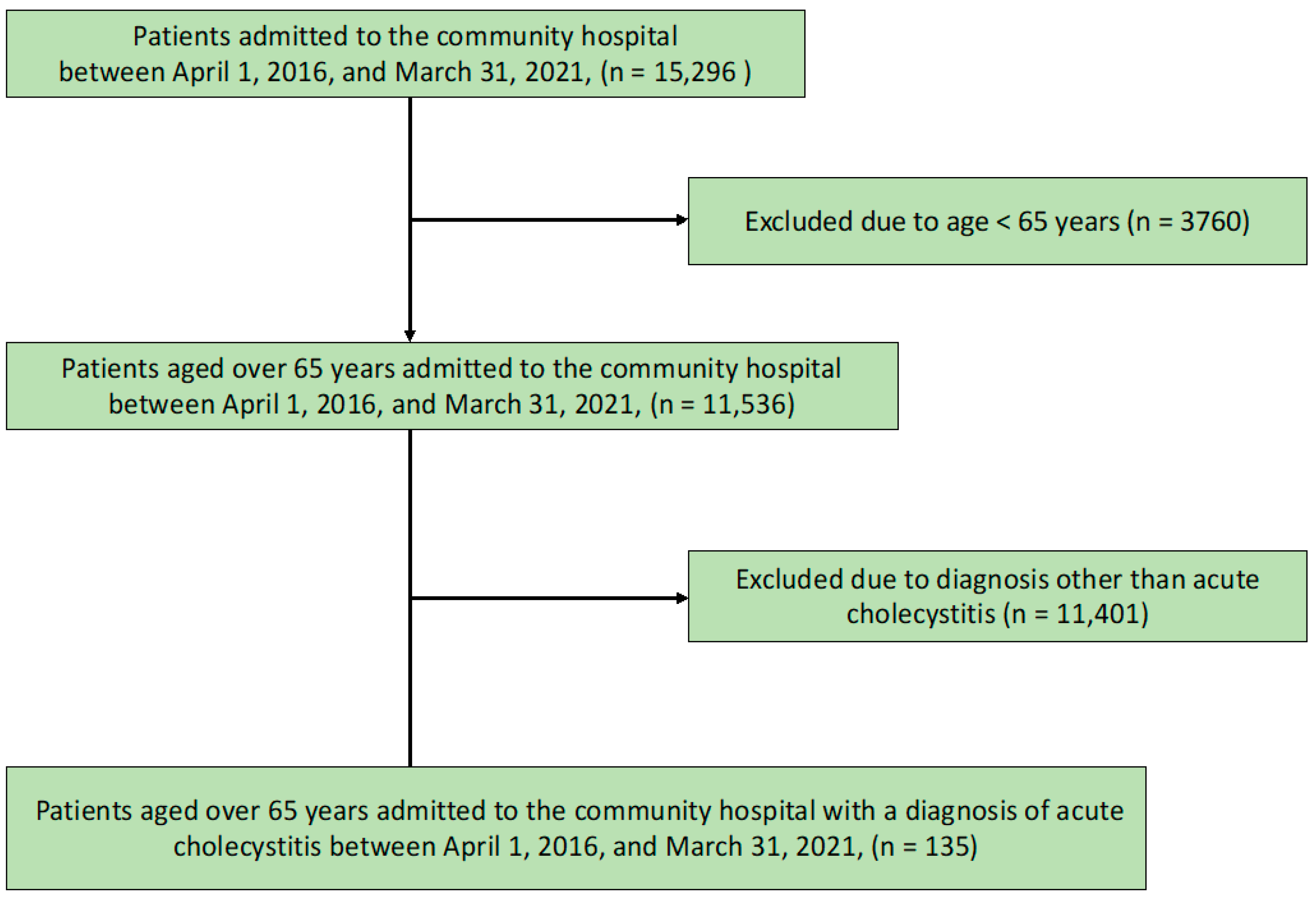
2.2. Participants
2.3. Measurements
2.3.1. Primary Outcome
2.3.2. Independent Variables
2.4. Analyses
2.5. Ethical Considerations
3. Results
3.1. Participant Demographics
3.2. Relationship between the Time to Diagnosis and Demographic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elwood, D.R. Cholecystitis. Surg. Clin. N. Am. 2008, 88, 1241–1252. [Google Scholar] [CrossRef] [PubMed]
- Knab, L.M.; Boller, A.M.; Mahvi, D.M. Cholecystitis. Surg. Clin. N. Am. 2014, 94, 455–470. [Google Scholar] [CrossRef] [PubMed]
- Indar, A.A.; Beckingham, I.J. Acute cholecystitis. BMJ 2002, 325, 639–643. [Google Scholar] [CrossRef]
- Yokoe, M.; Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Mayumi, T.; Gomi, H.; Pitt, H.A.; Gouma, D.J.; Garden, O.J.; Büchler, M.W.; et al. New diagnostic criteria and severity assessment of acute cholecystitis in revised Tokyo Guidelines. J. Hepatobiliary Pancreat. Sci. 2012, 19, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Loozen, C.S.; van Ramshorst, B.; van Santvoort, H.C.; Boerma, D. Early cholecystectomy for acute cholecystitis in the elderly population: A systematic review and meta-analysis. Dig. Surg. 2017, 34, 371–379. [Google Scholar] [CrossRef] [PubMed]
- McGillicuddy, E.A.; Schuster, K.M.; Barre, K.; Suarez, L.; Hall, M.R.; Kaml, G.J.; Davis, K.A.; Longo, W.E. Non-operative management of acute cholecystitis in the elderly. Br. J. Surg. 2012, 99, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Sano, C. Older people’s help-seeking behaviors in rural contexts: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 3233. [Google Scholar] [CrossRef]
- Greco, E.A.; Pietschmann, P.; Migliaccio, S. Osteoporosis and sarcopenia increase frailty syndrome in the elderly. Front. Endocrinol. 2019, 10, 255. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabil. 2017, 39, 1897–1908. [Google Scholar] [CrossRef]
- Ohta, R.; Sano, C. Risk of hospital readmission among older patients discharged from the rehabilitation unit in a rural community hospital: A retrospective cohort study. J. Clin. Med. 2021, 10, 659. [Google Scholar] [CrossRef]
- Soril, L.J.; Leggett, L.E.; Lorenzetti, D.L.; Noseworthy, T.W.; Clement, F.M. Characteristics of frequent users of the emergency department in the general adult population: A systematic review of international healthcare systems. Health Policy 2016, 120, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Pines, J.M.; Mullins, P.M.; Cooper, J.K.; Feng, L.B.; Roth, K.E. National trends in emergency department use, care patterns, and quality of care of older adults in the United States. J. Am. Geriatr. Soc. 2013, 61, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Parker, L.J.; Vukov, L.F.; Wollan, P.C. Emergency department evaluation of geriatric patients with acute cholecystitis. Acad. Emerg. Med. 1997, 4, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Maeki, N.; Maniwa, S.; Miyakoshi, K. Predicting factors of elderly patients’ discharge to home after rehabilitation in rural Japan: A retrospective cohort study. Rural. Remote Health 2021, 21, 6406. [Google Scholar] [CrossRef]
- Gallaher, J.R.; Charles, A. Acute cholecystitis: A review. JAMA 2022, 327, 965–975. [Google Scholar] [CrossRef]
- Sippey, M.; Grzybowski, M.; Manwaring, M.L.; Kasten, K.R.; Chapman, W.H.; Pofahl, W.E.; Pories, W.J.; Spaniolas, K. Acute cholecystitis: Risk factors for conversion to an open procedure. J. Surg. Res. 2015, 199, 357–361. [Google Scholar] [CrossRef]
- Ikegami, N.; Campbell, J.C. Japan’s health care system: Containing costs and attempting reform. Health Aff. (Millwood) 2004, 23, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Touma, E.; Bisharat, N. Trends in admission serum albumin and mortality in patients with hospital readmission. Int. J. Clin. Pract. 2019, 73, e13314. [Google Scholar] [CrossRef]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Holliday, M.A. Extracellular fluid and its proteins: Dehydration, shock, and recovery. Pediatr. Nephrol. 1999, 13, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Ponzetto, M.; Maero, B.; Maina, P.; Rosato, R.; Ciccone, G.; Merletti, F.; Rubenstein, L.Z.; Fabris, F. Risk factors for early and late mortality in hospitalized older patients: The continuing importance of functional status. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 1049–1054. [Google Scholar] [CrossRef] [Green Version]
- Llewellyn, D.J.; Langa, K.M.; Friedland, R.P.; Lang, I.A. Serum albumin concentration and cognitive impairment. Curr. Alzheimer Res. 2010, 7, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.I.; Boyko, E.J.; Ahroni, J.H.; Stensel, V.; Forsberg, R.C.; Smith, D.G. Risk factors for diabetic peripheral sensory neuropathy: Results of the Seattle Prospective Diabetic Foot Study. Diabetes Care 1997, 20, 1162–1167. [Google Scholar] [CrossRef]
- Ozdemir, G.; Ovayolu, N.; Ovayolu, O. The effect of reflexology applied on haemodialysis patients with fatigue, pain and cramps. Int. J. Nurs. Pract. 2013, 19, 265–273. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Sano, C. The relationship between the presence of white nails and mortality among rural, older, admitted patients: A prospective cohort study. Healthcare 2021, 9, 1611. [Google Scholar] [CrossRef]
- Matsui, Y.; Hirooka, S.; Kotsuka, M.; Yamaki, S.; Kosaka, H.; Yamamoto, T.; Satoi, S. Prognosis in patients with gallbladder edema misdiagnosed as cholecystitis. JSLS 2019, 23, e2019.00022. [Google Scholar] [CrossRef] [Green Version]
- Ho-A-Tham, N.; Ting-A-Kee, B.; Struyf, N.; Vanlandewijck, Y.; Dankaerts, W. Low back pain prevalence, beliefs and treatment-seeking behaviour in multi-ethnic Suriname. Rheumatol. Adv. Pract. 2021, 5, rkab074. [Google Scholar] [CrossRef]
- Ansar, A.; Lewis, V.; McDonald, C.F.; Liu, C.; Rahman, M.A. Duration of intervals in the care seeking pathway for lung cancer in Bangladesh: A journey from symptoms triggering consultation to receipt of treatment. PLoS ONE 2021, 16, e0257301. [Google Scholar] [CrossRef]
- Xu, W.; Li, Z.; Pan, Z.; He, R.; Zhang, L. Prevalence and associated factors of self-treatment behaviour among different elder subgroups in rural China: A cross-sectional study. Int. J. Equity Health 2020, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Freund, T.; Campbell, S.M.; Geissler, S.; Kunz, C.U.; Mahler, C.; Peters-Klimm, F.; Szecsenyi, J. Strategies for reducing potentially avoidable hospitalizations for ambulatory care-sensitive conditions. Ann. Fam. Med. 2013, 11, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Labra, O.; Wright, R.; Tremblay, G.; Maltais, D.; Bustinza, R.; Gingras-Lacroix, G. Men’s help-seeking attitudes in rural communities affected by a natural disaster. Am. J. Men’s Health 2019, 13, 1557988318821512. [Google Scholar] [CrossRef] [PubMed]
- Creighton, G.; Oliffe, J.; Ogrodniczuk, J.; Frank, B. "You’ve gotta be that tough crust exterior man": Depression and suicide in rural-based men. Qual. Health Res. 2017, 27, 1882–1891. [Google Scholar] [CrossRef]
- Ohta, R.; Sato, M.; Kitayuguchi, J.; Maeno, T.; Sano, C. The association between the self-management of mild symptoms and quality of life of elderly populations in rural communities: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 8857. [Google Scholar] [CrossRef]
- Saint Arnault, D. Cultural determinants of help seeking: A model for research and practice. Res. Theory Nurs. Pract. 2009, 23, 259–278. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.; Mehta, N.; Secko, M.; Schechter, J.; Papanagnou, D.; Pandya, S.; Sinert, R. History, physical examination, laboratory testing, and emergency department ultrasonography for the diagnosis of acute cholecystitis. Acad. Emerg. Med. 2017, 24, 281–297. [Google Scholar] [CrossRef] [Green Version]
- Trowbridge, R.L.; Rutkowski, N.K.; Shojania, K.G. Does this patient have acute cholecystitis? JAMA 2003, 289, 80–86. [Google Scholar] [CrossRef]
- Franssen, F.M.E. Overweight and obesity are risk factors for COPD misdiagnosis and overtreatment. Chest 2014, 146, 1426–1428. [Google Scholar] [CrossRef]
- Forster, M.J.; Akoh, J.A. Perforated appendicitis masquerading as acute pancreatitis in a morbidly obese patient. World J. Gastroenterol. 2008, 14, 1795–1796. [Google Scholar] [CrossRef]
- Newman-Toker, D.E.; Pronovost, P.J. Diagnostic errors—the next frontier for patient safety. JAMA 2009, 301, 1060–1062. [Google Scholar] [CrossRef] [PubMed]
- Cifu, A.S. Diagnostic errors and diagnostic calibration. JAMA 2017, 318, 905–906. [Google Scholar] [CrossRef]
- Cassel, C.; Fulmer, T. Achieving diagnostic excellence for older patients. JAMA 2022, 327, 919–920. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Sano, C. Improvement in quality of life through self-management of mild symptoms during the COVID-19 pandemic: A prospective cohort study. Int. J. Environ. Res. Public Health 2022, 19, 6652. [Google Scholar] [CrossRef] [PubMed]
- McDonald, K.M. Achieving equity in diagnostic excellence. JAMA 2022, 327, 1955–1956. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Time to Diagnosis | |||
|---|---|---|---|
| Factor | ≤3 Days (Control) | >3 Days (Exposure) | p-Value |
| N | 96 | 39 | |
| Age, mean (SD) | 77.71 (14.62) | 80.13 (13.95) | 0.379 |
| Age ≥ 80 years (%) | 51 (53.1) | 24 (61.5) | 0.446 |
| Male sex (%) | 40 (41.7) | 25 (64.1) | 0.023 |
| Albumin level, mean (SD) | 3.74 (0.67) | 3.29 (0.73) | 0.001 |
| BMI, mean (SD) | 23.68 (4.13) | 21.70 (3.09) | 0.008 |
| Creatinine level (SD) | 0.91 (0.48) | 0.90 (0.92) | 0.947 |
| eGFR (SD) | 64.48 (20.87) | 64.16 (19.79) | 0.935 |
| Hemoglobin level, mean (SD) | 12.96 (2.00) | 12.39 (1.60) | 0.119 |
| White blood cell count (median) | 10.15 (3.00, 29.70) | 9.70 (3.60, 19.30) | 0.638 |
| Total bilirubin level (median) | 1.30 (0.30, 7.00) | 1.20 (0.30, 7.20) | 0.602 |
| Direct bilirubin level (median) | 0.50 (0.10, 5.30) | 0.60 (0.10, 4.40) | 0.196 |
| AST level (median) | 34 (11, 2319) | 56 (15, 1199) | 0.187 |
| ALT level (median) | 34 (7, 849) | 56 (8, 726) | 0.437 |
| ALP level (median) | 284(53, 1719) | 328 (70, 3232) | 0.197 |
| FIM score at discharge | |||
| Total FIM score (median) | 120 (18, 126) | 80 (18, 126) | 0.03 |
| Motor domain score (median) | 85 (11, 91) | 63 (13, 91) | 0.054 |
| Cognitive domain score (median) | 35.00 (5, 35) | 32 (5, 35) | 0.019 |
| Abdominal pain (%) | 70 (72.9) | 19 (48.7) | 0.009 |
| Systolic blood pressure (SD) | 130.23 (25.51) | 126.92 (21.63) | 0.478 |
| Diastolic blood pressure (SD) | 76.49 (14.70) | 75.46 (16.34) | 0.722 |
| Heart rate (SD) | 86.28 (18.65) | 84.67 (17.85) | 0.645 |
| Fever (%) | 32 (33.3) | 14 (35.9) | 0.842 |
| Respiratory rate (SD) | 20.07 (4.52) | 20.44 (5.36) | 0.76 |
| SpO2 (SD) | 96.09 (2.20) | 95.51 (2.53) | 0.194 |
| CCI score ≥ 5 (%) | 53 (55.2) | 23 (59.0) | 0.707 |
| CCI score (%) | |||
| 1 | 7 (7.3) | 2 (5.2) | |
| 2 | 9 (9.4) | 2 (5.1) | |
| 3 | 6 (6.2) | 4 (10.3) | |
| 4 | 21 (21.9) | 8 (20.5) | |
| 5 | 14 (14.6) | 8 (20.5) | |
| 6 | 16 (16.7) | 6 (15.4) | |
| 7 | 10 (10.4) | 4 (10.3) | |
| 8 | 6 (6.2) | 3 (7.7) | |
| 9 | 2 (2.1) | 2 (5.1) | |
| 10 | 4 (4.2) | 0 (0.0) | |
| 11 | 1 (1.0) | 0 (0.0) | |
| Heart failure (%) | 13 (13.5) | 7 (17.9) | 0.594 |
| MI (%) | 6 (6.2) | 1 (2.6) | 0.673 |
| Asthma (%) | 5 (5.2) | 2 (5.1) | 1 |
| Peptic ulcer (%) | 19 (19.8) | 8 (20.5) | 1 |
| Kidney disease (%) | 13 (13.5) | 2 (5.1) | 0.23 |
| Liver disease (%) | 5 (5.2) | 4 (10.3) | 0.281 |
| COPD (%) | 3 (3.1) | 1 (2.6) | 1 |
| DM (%) | 19 (19.8) | 7 (17.9) | 1 |
| Brain infarction (%) | 22 (22.9) | 4 (10.3) | 0.147 |
| Brain hemorrhage (%) | 0 (0.0) | 1 (2.6) | 0.289 |
| Hemiplegia (%) | 8 (8.3) | 3 (7.7) | 1 |
| Connective tissue disease (%) | 2 (2.1) | 1 (2.6) | 1 |
| Dementia (%) | 21 (21.9) | 11 (28.2) | 0.504 |
| Cancer (%) | 17 (17.7) | 3 (7.7) | 0.184 |
| Living with family | 86 (89.6) | 30 (76.9) | 0.098 |
| Dependent condition (%) | 27 (28.1) | 16 (41.0) | 0.158 |
| Care level (%) | |||
| 0 | 69 (71.9) | 23 (59.0) | 0.336 |
| 1 | 5 (5.2) | 3 (7.7) | |
| 2 | 7 (7.3) | 6 (15.4) | |
| 3 | 7 (7.3) | 2 (5.1) | |
| 4 | 6 (6.2) | 2 (5.1) | |
| 5 | 2 (2.1) | 3 (7.7) | |
| Factor | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Abdominal pain | 0.57 | 0.24–1.39 | 0.22 |
| Male sex | 0.43 | 0.18–1.01 | 0.05 |
| Albumin | 0.51 | 0.28–0.94 | 0.032 |
| BMI | 0.90 | 0.80–1.01 | 0.07 |
| Total FIM score | 1.00 | 0.99–1.01 | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, H.; Ohta, R.; Sano, C. Risk Factors for Delayed Diagnosis of Acute Cholecystitis among Rural Older Patients: A Retrospective Cohort Study. Medicina 2022, 58, 1392. https://doi.org/10.3390/medicina58101392
Ikeda H, Ohta R, Sano C. Risk Factors for Delayed Diagnosis of Acute Cholecystitis among Rural Older Patients: A Retrospective Cohort Study. Medicina. 2022; 58(10):1392. https://doi.org/10.3390/medicina58101392
Chicago/Turabian StyleIkeda, Hirotaka, Ryuichi Ohta, and Chiaki Sano. 2022. "Risk Factors for Delayed Diagnosis of Acute Cholecystitis among Rural Older Patients: A Retrospective Cohort Study" Medicina 58, no. 10: 1392. https://doi.org/10.3390/medicina58101392