

Evaluation of Sagittal Spinopelvic Alignment on Analgesic Efficacy of Lumbar Epidural Steroid Injection in Geriatric Patients

Abstract
:1. Introduction
2. Materials and Methods
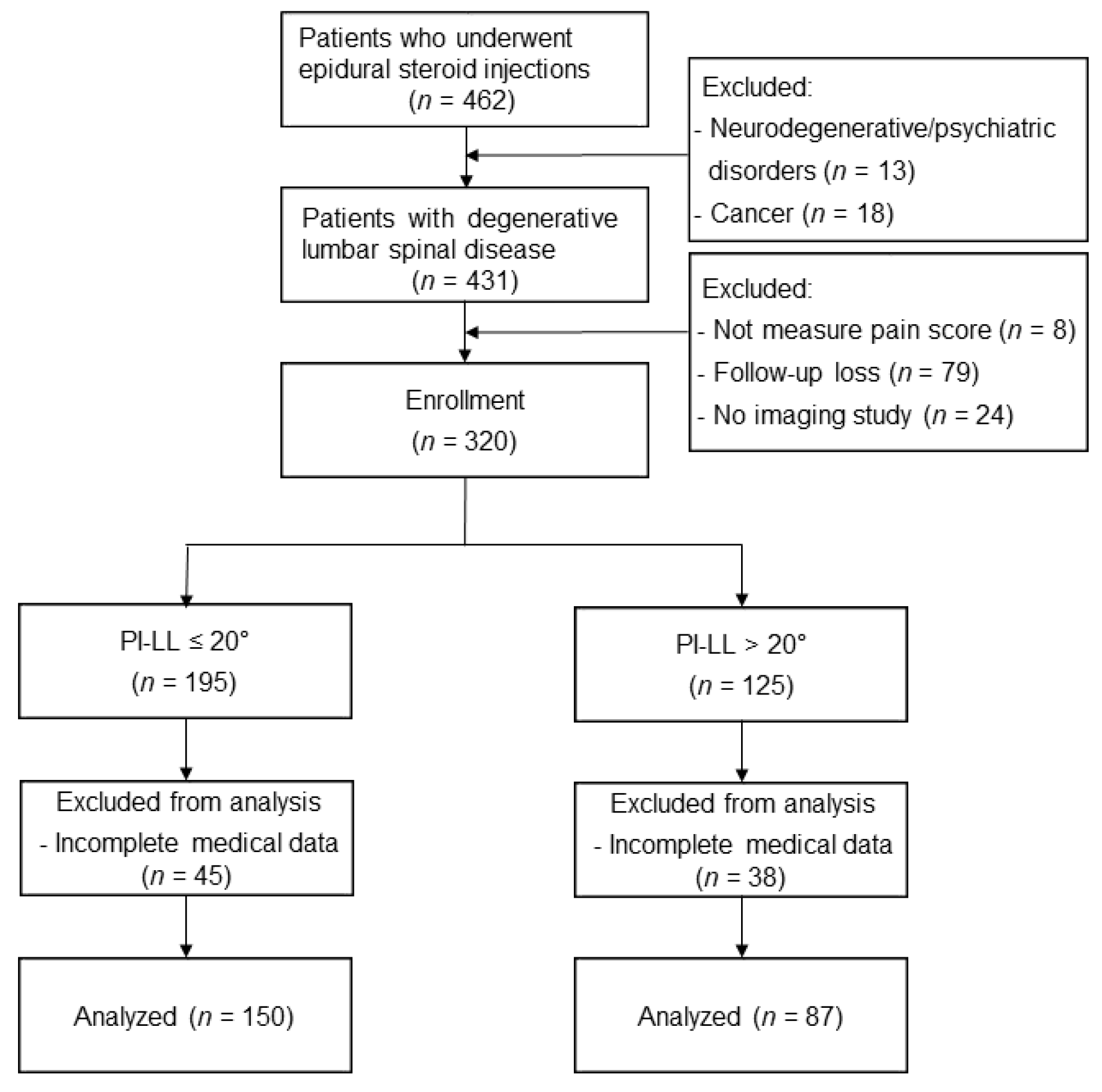
2.1. Study Population
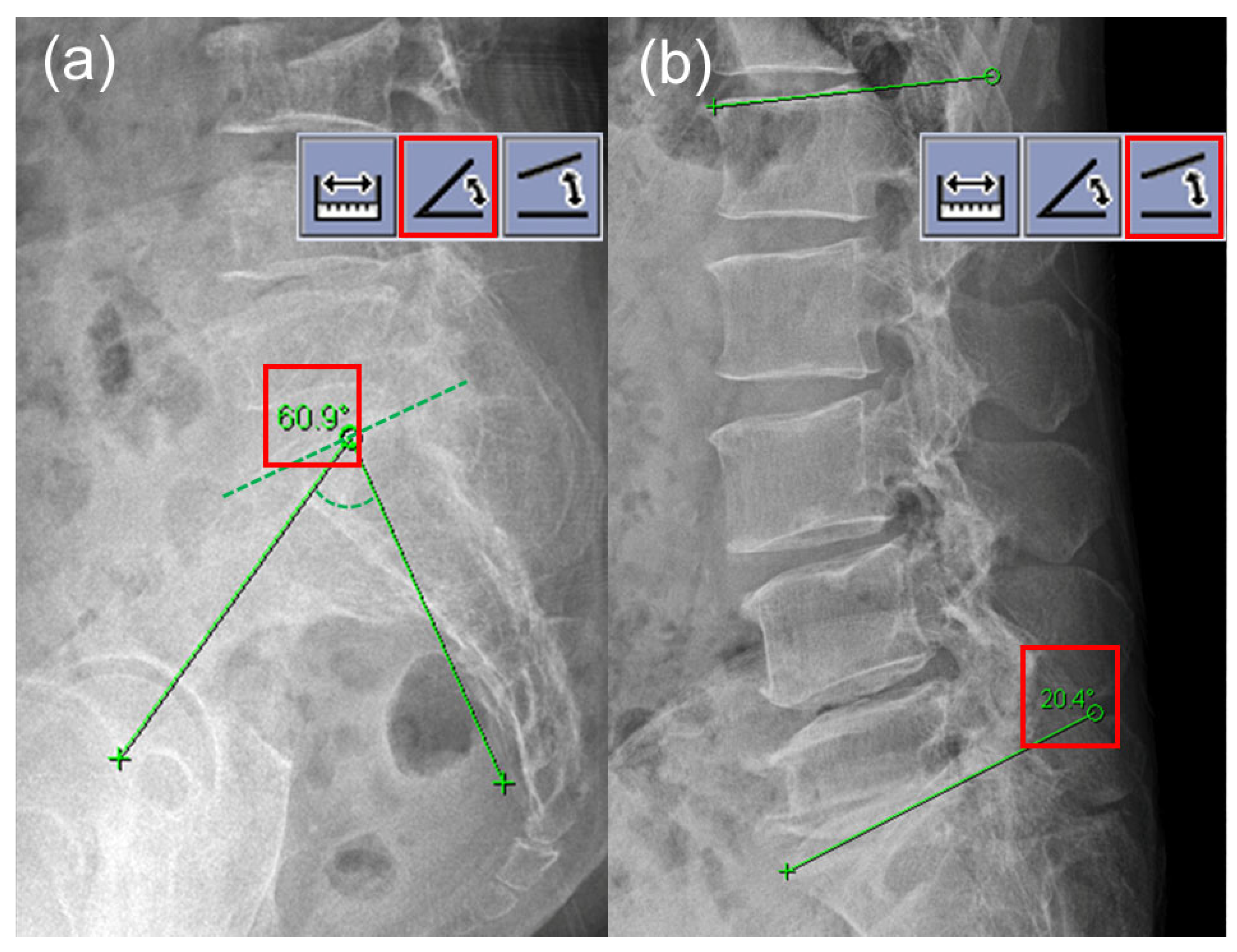
2.2. Spinopelvic Measurements
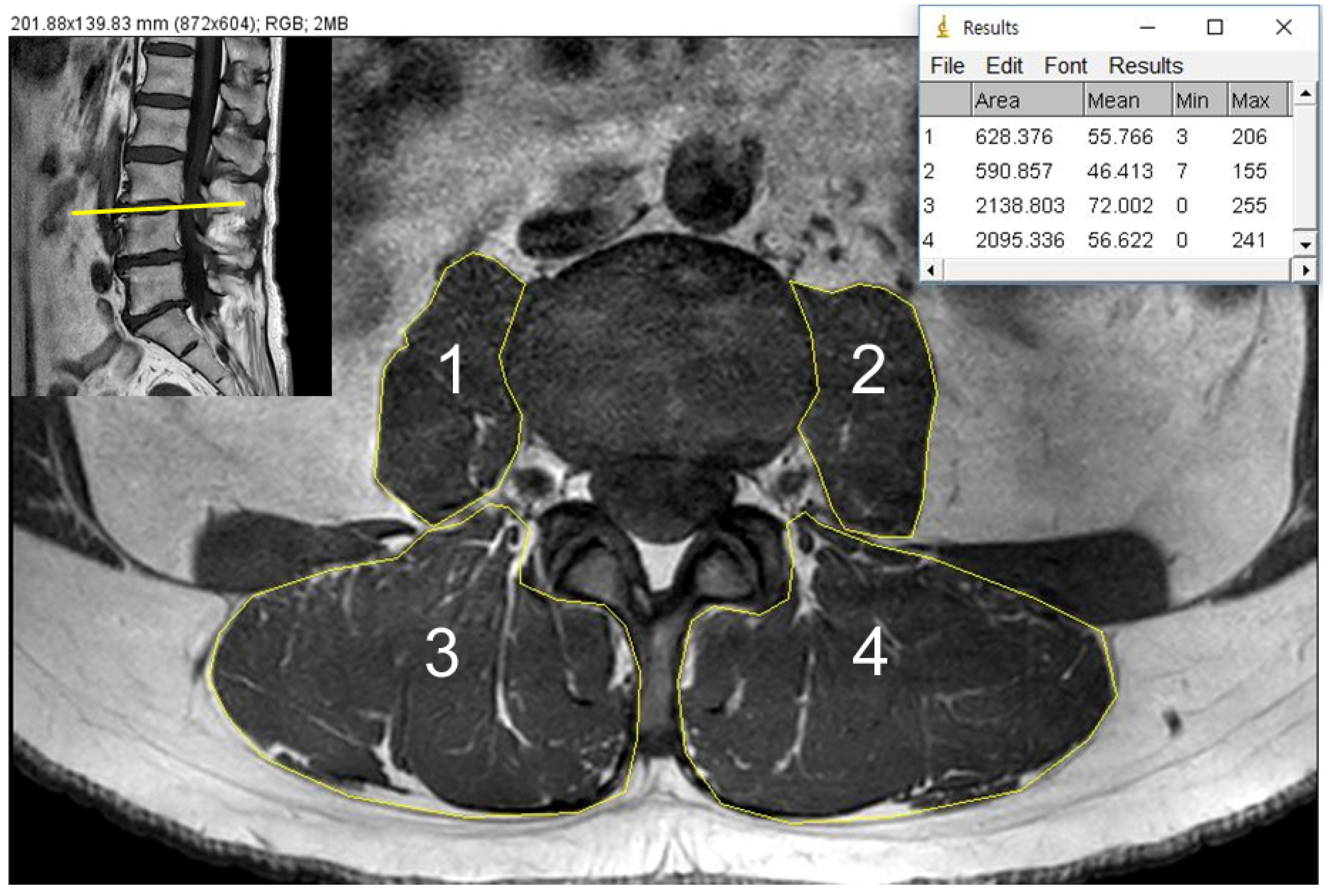
2.3. CSA and Fat Infiltration Measurements
2.4. Fluoroscopy-Guided Lumbar ESI
2.5. Patient Demographics and Clinical Data Measurements
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takemitsu, Y.; Harada, Y.; Iwahara, T.; Miyamoto, M.; Miyatake, Y. Lumbar degenerative kyphosis: Clinical, radiological and epidemiological studies. Spine 1988, 13, 1317–1326. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.J.; Kim, K.T.; Kim, W.J.; Lee, S.H.; Jung, J.H.; Kim, Y.T.; Park, H.B. Pedicle subtraction osteotomy in elderly patients with degenerative sagittal imbalance. Spine 2013, 38, E1561–E1566. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Lee, C.K.; Kim, Y.T.; Hong, Y.M.; Yoo, J.H. Dynamic sagittal imbalance of the spine in degenerative flat back: Significance of pelvic tilt in surgical treatment. Spine 2001, 26, 2029–2035. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.K.; Kim, J.S.; Leven, D.M.; Kim, J.H.; Cho, S.K. Beyond Pelvic Incidence-Lumbar Lordosis Mismatch: The Importance of Assessing the Entire Spine to Achieve Global Sagittal Alignment. Glob. Spine J. 2017, 7, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Rothenfluh, D.A.; Mueller, D.A.; Rothenfluh, E.; Min, K. Pelvic incidence-lumbar lordosis mismatch predisposes to adjacent segment disease after lumbar spinal fusion. Eur. Spine J. 2015, 24, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Nakajima, A.; Takahashi, H.; Sonobe, M.; Terajima, F.; Saito, M.; Takahashi, K.; Ohtori, S.; Watanabe, A.; Nakajima, T.; et al. Influence of pelvic incidence-lumbar lordosis mismatch on surgical outcomes of short-segment transforaminal lumbar interbody fusion. BMC Musculoskelet. Disord. 2015, 16, 213. [Google Scholar] [CrossRef] [Green Version]
- Le Huec, J.C.; Faundez, A.; Dominguez, D.; Hoffmeyer, P.; Aunoble, S. Evidence showing the relationship between sagittal balance and clinical outcomes in surgical treatment of degenerative spinal diseases: A literature review. Int. Orthop. 2015, 39, 87–95. [Google Scholar] [CrossRef]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; Wijethilake, P.; O’Sullivan, R.; Cicuttini, F.M. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015, 15, 1593–1601. [Google Scholar] [CrossRef]
- Kim, W.J.; Shin, H.M.; Lee, J.S.; Song, D.G.; Lee, J.W.; Chang, S.H.; Park, K.Y.; Choy, W.S. Sarcopenia and Back Muscle Degeneration as Risk Factors for Degenerative Adult Spinal Deformity with Sagittal Imbalance and Degenerative Spinal Disease: A Comparative Study. World Neurosurg. 2021, 148, e547–e555. [Google Scholar] [CrossRef]
- Manchikanti, L.; Knezevic, N.N.; Boswell, M.V.; Kaye, A.D.; Hirsch, J.A. Epidural Injections for Lumbar Radiculopathy and Spinal Stenosis: A Comparative Systematic Review and Meta-Analysis. Pain Physician 2016, 19, E365–E410. [Google Scholar] [CrossRef]
- Schwab, F.; Ungar, B.; Blondel, B.; Buchowski, J.; Coe, J.; Deinlein, D.; DeWald, C.; Mehdian, H.; Shaffrey, C.; Tribus, C.; et al. Scoliosis Research Society-Schwab adult spinal deformity classification: A validation study. Spine 2012, 37, 1077–1082. [Google Scholar] [CrossRef]
- Shen, F.; Kim, H.J.; Jeon, S.W.; Chang, B.S.; Lee, C.K.; Yeom, J.S. Influence of Handgrip Strength and Paraspinal Muscles’ Volume on Clinical Outcomes in the Patients with Each Sagittal Imbalance and Lumbar Spinal Stenosis. Glob. Spine J. 2021, 21925682211001871. [Google Scholar] [CrossRef]
- Honkanen, T.; Mäntysaari, M.; Leino, T.; Avela, J.; Kerttula, L.; Haapamäki, V.; Kyröläinen, H. Cross-sectional area of the paraspinal muscles and its association with muscle strength among fighter pilots: A 5-year follow-up. BMC Musculoskelet. Disord. 2019, 20, 170. [Google Scholar] [CrossRef]
- Stanuszek, A.; Jędrzejek, A.; Gancarczyk-Urlik, E.; Kołodziej, I.; Pisarska-Adamczyk, M.; Milczarek, O.; Trompeta, J.; Chrobak, W. Preoperative paraspinal and psoas major muscle atrophy and paraspinal muscle fatty degeneration as factors influencing the results of surgical treatment of lumbar disc disease. Arch. Orthop. Trauma Surg. 2022, 142, 1375–1384. [Google Scholar] [CrossRef]
- Arbanas, J.; Pavlovic, I.; Marijancic, V.; Vlahovic, H.; Starcevic-Klasan, G.; Peharec, S.; Bajek, S.; Miletic, D.; Malnar, D. MRI features of the psoas major muscle in patients with low back pain. Eur. Spine J. 2013, 22, 1965–1971. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.C.; Lee, D.G. Outcome of Transforaminal Epidural Steroid Injection According to the Severity of Lumbar Foraminal Spinal Stenosis. Pain Physician 2018, 21, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.Y.; Lee, J.W.; Choi, H.S.; Oh, K.J.; Kang, H.S. A new grading system of lumbar central canal stenosis on MRI: An easy and reliable method. Skelet. Radiol. 2011, 40, 1033–1039. [Google Scholar] [CrossRef] [Green Version]
- Cohen, L.; Pappas, E.; Refshauge, K.; Dennis, S.; Simic, M. Associations between potentially modifiable clinical factors and sagittal balance of the spine in older adults from the general population. Spine Deform. 2022, 10, 433–441. [Google Scholar] [CrossRef]
- Hiyama, A.; Katoh, H.; Sakai, D.; Tanaka, M.; Sato, M.; Watanabe, M. The correlation analysis between sagittal alignment and cross-sectional area of paraspinal muscle in patients with lumbar spinal stenosis and degenerative spondylolisthesis. BMC Musculoskelet. Disord. 2019, 20, 352. [Google Scholar] [CrossRef] [PubMed]
- Banno, T.; Yamato, Y.; Hasegawa, T.; Kobayashi, S.; Togawa, D.; Oe, S.; Mihara, Y.; Kurosu, K.; Yamamoto, N.; Matsuyama, Y. Assessment of the Cross-Sectional Areas of the Psoas Major and Multifidus Muscles in Patients with Adult Spinal Deformity: A Case-Control Study. Clin. Spine Surg. 2017, 30, E968–E973. [Google Scholar] [CrossRef]
- Menezes-Reis, R.; Bonugli, G.P.; Salmon, C.E.G.; Mazoroski, D.; Herrero, C.F.P.D.S.; Nogueira-Barbosa, M.H. Relationship of spinal alignment with muscular volume and fat infiltration of lumbar trunk muscles. PLoS ONE 2018, 13, e0200198. [Google Scholar] [CrossRef]
- Jermy, J.E.; Copley, P.C.; Poon, M.T.C.; Demetriades, A.K. Does pre-operative multifidus morphology on MRI predict clinical outcomes in adults following surgical treatment for degenerative lumbar spine disease? A systematic review. Eur. Spine J. 2020, 29, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Wang, W.; Kong, C.; Wang, Y.; Pan, F.; Lu, S. Lumbar Muscle Fat Content Has More Correlations with Living Quality than Sagittal Vertical Axis in Elderly Patients with Degenerative Lumbar Disorders. Clin. Interv. Aging 2020, 15, 1717–1726. [Google Scholar] [CrossRef]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; O’Sullivan, R.; Jones, G.; Cicuttini, F.M. Physical inactivity is associated with narrower lumbar intervertebral discs, high fat content of paraspinal muscles and low back pain and disability. Arthritis Res. Ther. 2015, 17, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosgrove, J.L.; Bertolet, M.; Chase, S.L.; Cosgrove, G.K. Epidural steroid injections in the treatment of lumbar spinal stenosis efficacy and predictability of successful response. Am. J. Phys. Med. Rehabil. 2011, 90, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.J.; Chotai, S.; Sivaganesan, A.; Archer, K.R.; Schneider, B.J.; Yang, A.J.; Devin, C.J. Effect of pre-injection opioid use on post-injection patient-reported outcomes following epidural steroid injections for radicular pain. Spine J. 2018, 18, 788–796. [Google Scholar] [CrossRef]
- Crawford, R.J.; Filli, L.; Elliott, J.M.; Nanz, D.; Fischer, M.A.; Marcon, M.; Ulbrich, E.J. Age- and Level-Dependence of Fatty Infiltration in Lumbar Paravertebral Muscles of Healthy Volunteers. AJNR Am. J. Neuroradiol. 2016, 37, 742–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urrutia, J.; Besa, P.; Lobos, D.; Andia, M.; Arrieta, C.; Uribe, S. Is a single-level measurement of paraspinal muscle fat infiltration and cross-sectional area representative of the entire lumbar spine? Skelet. Radiol. 2018, 47, 939–945. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | PI-LL ≤ 20° (n = 150) | PI-LL > 20° (n = 87) | p-Value |
|---|---|---|---|
| Patient characteristics | |||
| Age, years | 73.68 ± 5.52 | 73.48 ± 6.58 | 0.814 |
| Sex, M/F | 62 (41.3)/88 (58.7) | 19 (21.8)/68 (78.2) | 0.002 |
| Body mass index, kg/m2 | 24.45 (22.61–26.39) | 24.55 (22.52–27.10) | 0.899 |
| Spine surgery history, n | 29 (19.3) | 31 (35.6) | 0.005 |
| Pain-related data | |||
| Pain duration, months | 6.00 (1.00–18.75) | 7.00 (2.00–36.00) | 0.227 |
| Baseline pain score, NRS 0–10 | 7.13 ± 1.75 | 7.11 ± 1.59 | 0.936 |
| Opioid use before injection, n | 44 (29.3) | 34 (39.1) | 0.124 |
| Pre-procedural MRI findings, n | |||
| Herniated disc | 146 (97.3) | 85 (97.7) | 0.862 |
| Foraminal stenosis | 0.572 | ||
| No to mild | 34 (22.7) | 17 (19.5) | |
| Moderate to severe | 116 (77.3) | 70 (80.5) | |
| Central stenosis | 0.816 | ||
| No to mild | 110 (73.3) | 65 (74.7) | |
| Moderate to severe | 40 (26.7) | 22 (25.3) | |
| Compression fracture | 22 (14.7) | 18 (20.7) | 0.233 |
| Spondylolisthesis | 34 (22.7) | 14 (16.1) | 0.225 |
| Spinopelvic parameters | |||
| PI | 46.50 ± 11.36 | 58.06 ± 10.30 | <0.001 |
| LL | 38.75 ± 10.64 | 29.28 ± 10.69 | <0.001 |
| PI-LL | 7.75 ± 9.16 | 28.78 ± 6.83 | <0.001 |
| Muscle degeneration | |||
| Cross-sectional area, cm2/m2 | |||
| Psoas muscles | 5.40 ± 1.61 | 4.76 ± 1.39 | 0.001 |
| Paraspinal muscles | 18.61 ± 3.04 | 18.03 ± 3.25 | 0.163 |
| Psoas + paraspinal muscles | 24.01 ± 3.70 | 22.78 ± 3.84 | 0.016 |
| Paraspinal fat infiltration grade | 0.238 | ||
| Grade 0, normal | 32 (21.3) | 10 (11.5) | |
| Grade 1, mild | 73 (48.7) | 50 (57.5) | |
| Grade 2, severe | 45 (30.0) | 27 (31.0) | |
| Epidural approaches, n | 0.235 | ||
| Interlaminar | 5 (3.3) | 1 (1.1) | |
| Transforaminal | 132 (88.0) | 73 (83.9) | |
| Caudal | 13 (8.7) | 13 (14.9) | |
| PI-LL ≤ 20° (n = 150) | PI-LL > 20° (n = 87) | p-Value | |
|---|---|---|---|
| 4 weeks follow-up, n | 0.889 | ||
| Good analgesia | 90 (60.0) | 53 (60.9) | |
| Poor analgesia | 60 (40.0) | 34 (39.1) | |
| 1 year follow-up, n | 0.421 | ||
| Transition to spine surgery | 17 (11.3) | 13 (14.9) |
| Crude OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Patient characteristics | ||||||
| Age, ≥ 75 years | 1.742 | 1.029–2.950 | 0.039 | 1.278 | 0.707–2.308 | 0.417 |
| Female | 1.506 | 0.860–2.637 | 0.152 | 0.931 | 0.478–1.812 | 0.833 |
| BMI, ≥ 25 kg/m2 | 1.134 | 0.669–1.920 | 0.641 | |||
| Spine surgery history, yes | 1.118 | 0.616–2.028 | 0.714 | |||
| Pain-related data | ||||||
| Pain duration, ≥ 1 years | 1.514 | 0.893–2.565 | 0.123 | 1.461 | 0.824–2.589 | 0.194 |
| Pain score, ≥ 7 on NRS | 1.155 | 0.672–1.985 | 0.601 | |||
| Opioid usage, yes | 1.891 | 1.090–3.281 | 0.023 | 2.021 | 1.127–3.622 | 0.018 |
| Pre-procedural MRI findings | ||||||
| Herniated disc, yes | 0.650 | 0.128–3.291 | 0.603 | |||
| Central stenosis, yes | 1.360 | 0.757–2.444 | 0.304 | |||
| Foraminal stenosis, yes | 2.255 | 1.127–4.510 | 0.022 | 2.672 | 1.274–5.603 | 0.009 |
| Compression fracture, yes | 1.017 | 0.508–2.036 | 0.962 | |||
| Spondylolisthesis, yes | 1.700 | 0.898–3.218 | 0.103 | 1.447 | 0.730–2.869 | 0.289 |
| Spinopelvic parameters | ||||||
| PI | 1.008 | 0.987–1.030 | 0.465 | |||
| LL | 1.003 | 0.981–1.026 | 0.765 | |||
| PI-LL | 1.004 | 0.985–1.024 | 0.674 | |||
| PI-LL mismatch >20°, yes | 0.962 | 0.560–1.652 | 0.889 | |||
| Muscle degeneration | ||||||
| Cross-sectional area, cm2/m2 | ||||||
| Psoas muscles | 0.902 | 0.761–1.070 | 0.237 | |||
| Paraspinal muscles | 1.026 | 0.944–1.115 | 0.549 | |||
| Psoas + paraspinal muscles | 1.001 | 0.934–1.071 | 0.995 | |||
| Paraspinal fat infiltration grade | ||||||
| Grade 0, normal | 1.000 | 1.000 | ||||
| Grade 1, mild | 2.042 | 0.896–4.656 | 0.089 | 2.032 | 0.876–4.713 | 0.098 |
| Grade 2, severe | 4.849 | 2.027–11.601 | <0.001 | 5.021 | 2.057–12.258 | <0.001 |
| Epidural approach | ||||||
| Caudal | 1.000 | |||||
| Interlaminar | 0.500 | 0.078–3.223 | 0.466 | |||
| Transforaminal | 0.627 | 0.277–1.422 | 0.264 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Ban, M.G.; Rho, M.; Jeon, W.; Kim, S.H. Evaluation of Sagittal Spinopelvic Alignment on Analgesic Efficacy of Lumbar Epidural Steroid Injection in Geriatric Patients. Medicina 2022, 58, 1383. https://doi.org/10.3390/medicina58101383
Kim HJ, Ban MG, Rho M, Jeon W, Kim SH. Evaluation of Sagittal Spinopelvic Alignment on Analgesic Efficacy of Lumbar Epidural Steroid Injection in Geriatric Patients. Medicina. 2022; 58(10):1383. https://doi.org/10.3390/medicina58101383
Chicago/Turabian StyleKim, Hee Jung, Min Gi Ban, Miribi Rho, Woohyuk Jeon, and Shin Hyung Kim. 2022. "Evaluation of Sagittal Spinopelvic Alignment on Analgesic Efficacy of Lumbar Epidural Steroid Injection in Geriatric Patients" Medicina 58, no. 10: 1383. https://doi.org/10.3390/medicina58101383