
Sex Difference in Cutoff and Prevalence of Sarcopenia among 300,090 Urban Korean Population: Association with Metabolic Syndrome


Abstract
:1. Introduction
2. Methods
2.1. Study Subjects
2.2. Laboratory and Anthropometric Measurements
2.3. Sarcopenia Status and Metabolic Syndrome
2.4. Statistical Analysis
3. Results
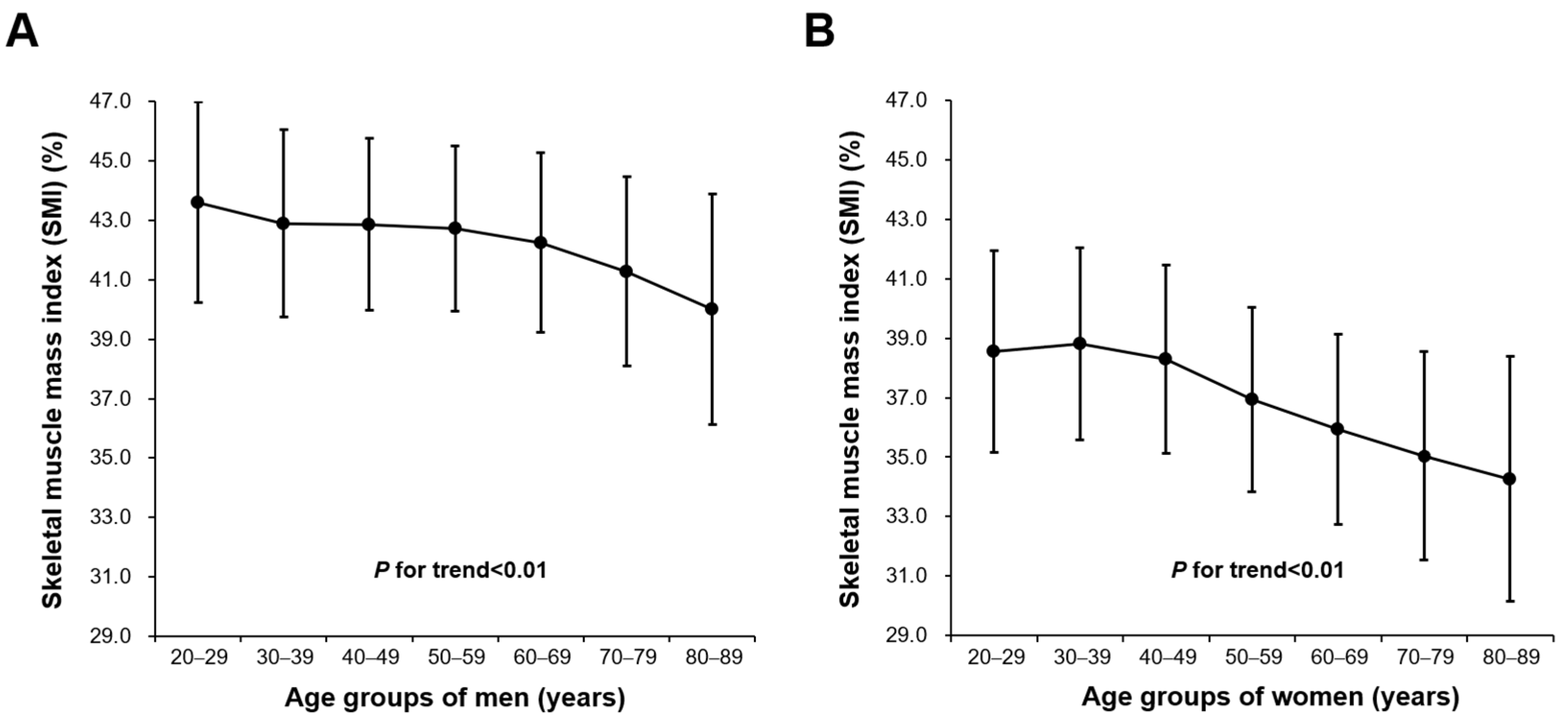
3.1. Baseline Characteristics and SMI Values of Study Participants
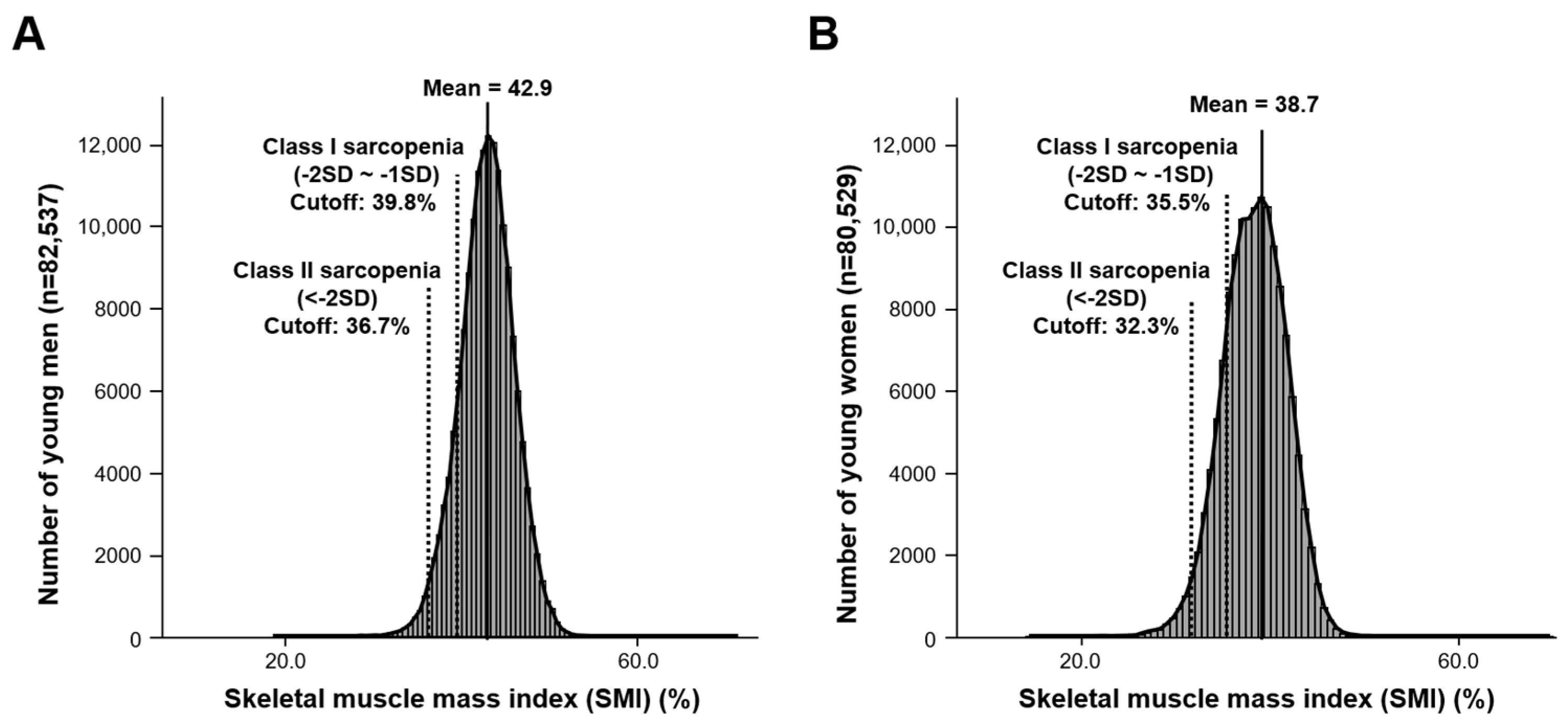
3.2. Threshold Levels for Class I and Class II Sarcopenia Based on Young Reference Group
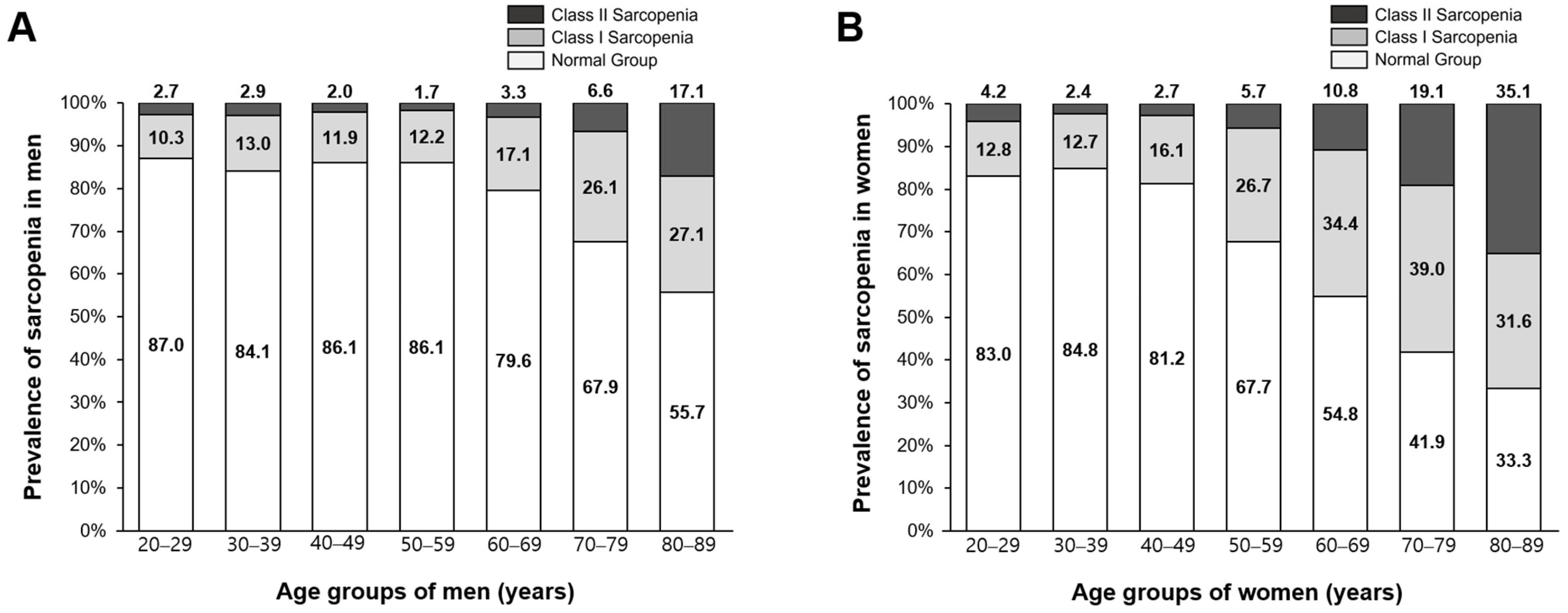
3.3. Prevalence Rate of Sarcopenia by Age Group
3.4. Sarcopenia Status and Metabolic Syndrome
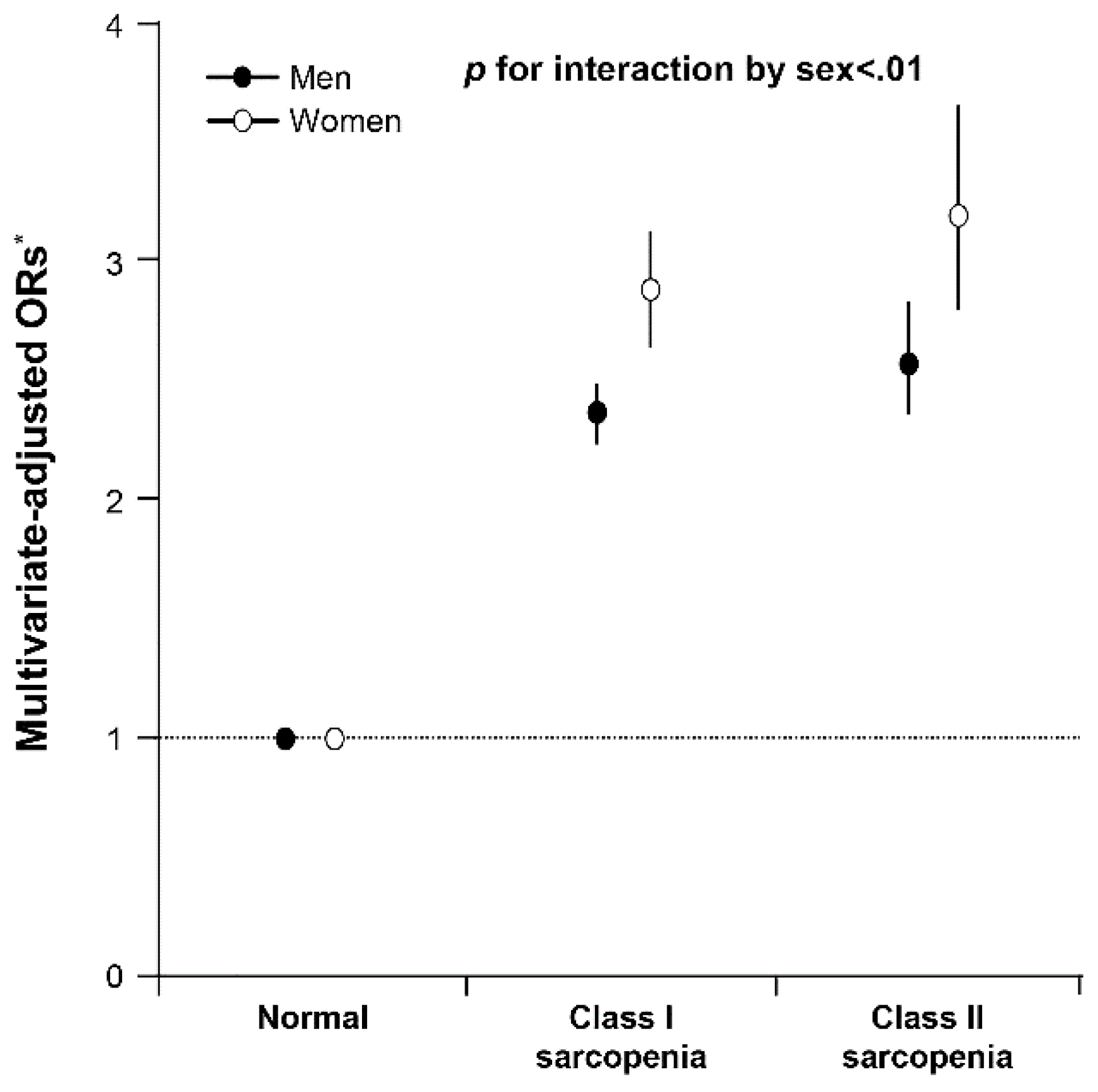
3.5. Sex Differences in the Association between Sarcopenia and Metabolic Syndrome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, W.J.; Campbell, W.W. Sarcopenia and age-related changes in body composition and functional capacity. J. Nutr. 1993, 123, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.C.; Cho, I.J.; Jeong, I.K.; Ahn, K.J.; Chung, H.Y. Differential association between sarcopenia and metabolic phenotype in Korean young and older adults with and without obesity. Obesity 2017, 25, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.J.; Jung, H.; Lee, T.; Kim, J.; Park, J.; Kim, H.; Cho, J.; Lee, W.Y.; Park, S.W.; Rhee, E.J.; et al. Decreased muscle mass in Korean subjects with intracranial arterial stenosis: The Kangbuk Samsung Health Study. Atherosclerosis 2017, 256, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.K.; Roh, E.; Yang, Y.S.; Moon, M.K. Difference between old and young adults in contribution of beta-cell function and sarcopenia in developing diabetes mellitus. J. Diabetes Investig. 2016, 7, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Moorthi, R.N.; Avin, K.G. Clinical relevance of sarcopenia in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2017, 26, 219–228. [Google Scholar] [CrossRef]
- Morley, J.E.; Malmstrom, T.K. Frailty, sarcopenia, and hormones. Endocrinol. Metab. Clin. N. Am. 2013, 42, 391–405. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Malmstrom, T.K.; Rodriguez-Manas, L.; Sinclair, A.J. Frailty, sarcopenia and diabetes. J. Am. Med. Dir. Assoc. 2014, 15, 853–859. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and physical frailty: Two sides of the same coin. Front. Aging Neurosci. 2014, 6, 192. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, S.; Walston, J.D. Frailty in older adults: Insights and interventions. Cleve. Clin. J. Med. 2005, 72, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Giallauria, F.; Di Lorenzo, A.; Venturini, E.; Pacileo, M.; D’Andrea, A.; Garofalo, U.; De Lucia, F.; Testa, C.; Cuomo, G.; Iannuzzo, G.; et al. Frailty in acute and chronic coronary syndrome patients entering cardiac rehabilitation. J. Clin. Med. 2021, 10, 1696. [Google Scholar] [CrossRef]
- Singh, M.; Stewart, R.; White, H. Importance of frailty in patients with cardiovascular disease. Eur. Heart J. 2014, 35, 1726–1731. [Google Scholar] [CrossRef]
- Fries, J.F. Frailty, heart disease, and stroke: The compression of morbidity paradigm. Am. J. Prev. Med. 2005, 29, 164–168. [Google Scholar] [CrossRef]
- Bazzocchi, A.; Diano, D.; Ponti, F.; Andreone, A.; Sassi, C.; Albisinni, U.; Marchesini, G.; Battista, G. Health and ageing: A cross-sectional study of body composition. Clin. Nutr. 2013, 32, 569–578. [Google Scholar] [CrossRef]
- Guglielmi, G.; Ponti, F.; Agostini, M.; Amadori, M.; Battista, G.; Bazzocchi, A. The role of DXA in sarcopenia. Aging Clin. Exp. Res. 2016, 28, 1047–1060. [Google Scholar] [CrossRef]
- Lee, S.Y.; Gallagher, D. Assessment methods in human body composition. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 566–572. [Google Scholar] [CrossRef]
- Cornish, B. Bioimpedance analysis: Scientific background. Lymphat. Res. Biol 2006, 4, 47–50. [Google Scholar] [CrossRef]
- Donini, L.M.; Poggiogalle, E.; Del Balzo, V.; Lubrano, C.; Faliva, M.; Opizzi, A.; Perna, S.; Pinto, A.; Rondanelli, M. How to estimate fat mass in overweight and obese subjects. Int. J. Endocrinol. 2013, 2013, 285680. [Google Scholar] [CrossRef] [PubMed]
- Bolanowski, M.; Nilsson, B.E. Assessment of human body composition using dual-energy x-ray absorptiometry and bioelectrical impedance analysis. Med. Sci. Monit. 2001, 7, 1029–1033. [Google Scholar] [PubMed]
- Sousa-Santos, A.R.; Barros, D.; Montanha, T.L.; Carvalho, J.; Amaral, T.F. Which is the best alternative to estimate muscle mass for sarcopenia diagnosis when DXA is unavailable? Arch. Gerontol. Geriatr. 2021, 97, 104517. [Google Scholar] [CrossRef]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2015, 15, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, C.; Janssen, I. Ethnic comparisons of sarcopenia and obesity in diabetes. Ethn. Dis. 2005, 15, 664–670. [Google Scholar] [PubMed]
- Morley, J.E.; Baumgartner, R.N.; Roubenoff, R.; Mayer, J.; Nair, K.S. Sarcopenia. J. Lab. Clin. Med. 2001, 137, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.D. Sarcopenia in older adults. Curr. Opin. Rheumatol. 2012, 24, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Filippin, L.I.; Teixeira, V.N.; da Silva, M.P.; Miraglia, F.; da Silva, F.S. Sarcopenia: A predictor of mortality and the need for early diagnosis and intervention. Aging Clin. Exp. Res. 2015, 27, 249–254. [Google Scholar] [CrossRef]
- Arango-Lopera, V.E.; Arroyo, P.; Gutierrez-Robledo, L.M.; Perez-Zepeda, M.U.; Cesari, M. Mortality as an adverse outcome of sarcopenia. J. Nutr. Health Aging 2013, 17, 259–262. [Google Scholar] [CrossRef]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Holvoet, P. Relations between metabolic syndrome, oxidative stress and inflammation and cardiovascular disease. Verh. K. Acad. Geneeskd. Belg. 2008, 70, 193–219. [Google Scholar] [PubMed]
- Sun, Y.X.; Hu, S.J.; Zhang, X.H.; Sun, J.; Zhu, C.H.; Zhang, Z.J. Plasma levels of vWF and NO in patients with metabolic syndrome and their relationship with metabolic disorders. Zhejiang Da Xue Xue Bao Yi Xue Ban 2006, 35, 315–318. [Google Scholar] [PubMed]
- Starzak, M.; Stanek, A.; Jakubiak, G.K.; Cholewka, A.; Cieslar, G. Arterial stiffness assessment by pulse wave velocity in patients with metabolic syndrome and its components: Is it a useful tool in clinical practice? Int. J. Environ. Res. Public Health 2022, 19, 10368. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Osadnik, T.; Goławski, M.; Lewandowski, P.; Pawlas, N. "Obesity and Insulin Resistance" Is the Component of the Metabolic Syndrome Most Strongly Associated with Oxidative Stress. Antioxidants 2021, 11, 79. [Google Scholar] [CrossRef] [PubMed]
- Stehouwer, C.D.; Henry, R.M.; Ferreira, I. Arterial stiffness in diabetes and the metabolic syndrome: A pathway to cardiovascular disease. Diabetologia 2008, 51, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Brioche, T.; Lemoine-Morel, S. Oxidative stress, sarcopenia, antioxidant strategies and exercise: Molecular aspects. Curr. Pharm. Des. 2016, 22, 2664–2678. [Google Scholar] [CrossRef]
- Chin, S.O.; Rhee, S.Y.; Chon, S.; Hwang, Y.C.; Jeong, I.K.; Oh, S.; Ahn, K.J.; Chung, H.Y.; Woo, J.T.; Kim, S.W.; et al. Sarcopenia is independently associated with cardiovascular disease in older Korean adults: The Korea National Health and Nutrition Examination Survey (KNHANES) from 2009. PLoS ONE 2013, 8, e60119. [Google Scholar] [CrossRef]
- Park, H.J.; Kim, J.; Park, S.E.; Park, C.Y.; Lee, W.Y.; Oh, K.W.; Park, S.W.; Rhee, E.J. Increased risk of subclinical atherosclerosis associated with high visceral adiposity index in apparently healthy Korean adults: The Kangbuk Samsung Health Study. Ann. Med. 2016, 48, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Pongchaiyakul, C.; Limpawattana, P.; Kotruchin, P.; Rajatanavin, R. Prevalence of sarcopenia and associated factors among Thai population. J. Bone Miner. Metab. 2013, 31, 346–350. [Google Scholar] [CrossRef]
- Bahat, G.; Tufan, A.; Kilic, C.; Ozturk, S.; Akpinar, T.S.; Kose, M.; Erten, N.; Karan, M.A.; Cruz-Jentoft, A.J. Cut-off points for weight and body mass index adjusted bioimpedance analysis measurements of muscle mass. Aging Clin. Exp. Res. 2019, 31, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Bijlsma, A.Y.; Meskers, C.G.; Ling, C.H.; Narici, M.; Kurrle, S.E.; Cameron, I.D.; Westendorp, R.G.; Maier, A.B. Defining sarcopenia: The impact of different diagnostic criteria on the prevalence of sarcopenia in a large middle aged cohort. Age 2013, 35, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation; Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000; pp. 15–21. [Google Scholar]
- Gallagher, D.; Visser, M.; De Meersman, R.E.; Sepulveda, D.; Baumgartner, R.N.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. Appendicular skeletal muscle mass: Effects of age, gender, and ethnicity. J. Appl. Physiol. 1997, 83, 229–239. [Google Scholar] [CrossRef]
- Bahat, G.; Tufan, A.; Tufan, F.; Kilic, C.; Akpinar, T.S.; Kose, M.; Erten, N.; Karan, M.A.; Cruz-Jentoft, A.J. Cut-off points to identify sarcopenia according to European Working Group on Sarcopenia in Older People (EWGSOP) definition. Clin. Nutr. 2016, 35, 1557–1563. [Google Scholar] [CrossRef]
- Hyun, Y.Y.; Lee, K.B.; Rhee, E.J.; Park, C.Y.; Chang, Y.; Ryu, S. Chronic kidney disease and high eGFR according to body composition phenotype in adults with normal BMI. Nutr. Metab. Cardiovasc. Dis. NMCD 2016, 26, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Feng, X.; Zhou, J.; Gong, H.; Xia, S.; Wei, Q.; Hu, X.; Tao, R.; Li, L.; Qian, F.; et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci. Rep. 2016, 6, 38937. [Google Scholar] [CrossRef] [PubMed]
- Costa, T.M.; Costa, F.M.; Moreira, C.A.; Rabelo, L.M.; Boguszewski, C.L.; Borba, V.Z. Sarcopenia in COPD: Relationship with COPD severity and prognosis. J. Bras. Pneumol. 2015, 41, 415–421. [Google Scholar] [CrossRef]
- Kim, Y.S.; Lee, Y.; Chung, Y.S.; Lee, D.J.; Joo, N.S.; Hong, D.; Song, G.; Kim, H.J.; Choi, Y.J.; Kim, K.M. Prevalence of sarcopenia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1107–1113. [Google Scholar] [CrossRef]
- Moon, J.H.; Kong, M.H.; Kim, H.J. Implication of sarcopenia and sarcopenic obesity on lung function in healthy elderly: Using Korean National Health and Nutrition Examination Survey. J. Korean Med. Sci. 2015, 30, 1682–1688. [Google Scholar] [CrossRef]
- Wen, X.; Wang, M.; Jiang, C.M.; Zhang, Y.M. Are current definitions of sarcopenia applicable for older Chinese adults? J. Nutr. Health Aging 2011, 15, 847–851. [Google Scholar] [CrossRef]
- Lim, S.; Kim, J.H.; Yoon, J.W.; Kang, S.M.; Choi, S.H.; Park, Y.J.; Kim, K.W.; Lim, J.Y.; Park, K.S.; Jang, H.C. Sarcopenic obesity: Prevalence and association with metabolic syndrome in the Korean Longitudinal Study on Health and Aging (KLoSHA). Diabetes Care 2010, 33, 1652–1654. [Google Scholar] [CrossRef] [PubMed]
- D’Elia, L.; Manfredi, M.; Sabino, P.; Strazzullo, P.; Galletti, F. The olivetti heart study: Predictive value of a new adiposity index on risk of hypertension, blood pressure, and subclinical organ damage. Nutr. Metab. Cardiovasc. Dis. NMCD 2016, 26, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.M. The politics of Ethnicity in Prehistoric Korea. In Contemporary Archaeology in Theory: The New Pragmatism; Preucel, R.W., Mrozowski, S.A., Eds.; John Wiley & Sons: New York, NY, USA, 2011; pp. 290–300. [Google Scholar]
- Massey, D.S. The new immigration and ethnicity in the United States. Popul. Dev. Rev. 1995, 21, 631–652. [Google Scholar] [CrossRef]
- Sahadeo, J.; Zanca, R. Everyday Life in Central Asia: Past and Present; Indiana University Press: Bloomington, IN, USA, 2007. [Google Scholar]
- Lu, C.W.; Yang, K.C.; Chang, H.H.; Lee, L.T.; Chen, C.Y.; Huang, K.C. Sarcopenic obesity is closely associated with metabolic syndrome. Obes. Res. Clin. Pract. 2013, 7, e301–e307. [Google Scholar] [CrossRef] [PubMed]
- Le Couteur, D.G.; Blyth, F.M.; Creasey, H.M.; Handelsman, D.J.; Naganathan, V.; Sambrook, P.N.; Seibel, M.J.; Waite, L.M.; Cumming, R.G. The association of alanine transaminase with aging, frailty, and mortality. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 712–717. [Google Scholar] [CrossRef]
- Foley, R.N.; Wang, C.; Ishani, A.; Collins, A.J.; Murray, A.M. Kidney function and sarcopenia in the United States general population: NHANES III. Am. J. Nephrol. 2007, 27, 279–286. [Google Scholar] [CrossRef]
- Kim, T.N.; Park, M.S.; Lim, K.I.; Choi, H.Y.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Choi, H.; Baik, S.H.; et al. Relationships between sarcopenic obesity and insulin resistance, inflammation, and vitamin D status: The Korean Sarcopenic Obesity Study. Clin. Endocrinol. 2013, 78, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Do, J.G.; Lee, Y.T.; Yoon, K.J. Sarcopenic obesity associated with high-sensitivity C-reactive protein in age and sex comparison: A two-center study in South Korea. BMJ Open 2018, 8, e021232. [Google Scholar] [CrossRef] [PubMed]
- Mannion, A.F.; Dumas, G.A.; Cooper, R.G.; Espinosa, F.J.; Faris, M.W.; Stevenson, J.M. Muscle fibre size and type distribution in thoracic and lumbar regions of erector spinae in healthy subjects without low back pain: Normal values and sex differences. J. Anat. 1997, 190 Pt 4, 505–513. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.M.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesinovic, J.; McMillan, L.B.; Shore-Lorenti, C.; De Courten, B.; Ebeling, P.R.; Scott, D. Metabolic syndrome and its associations with components of sarcopenia in overweight and obese older adults. J. Clin. Med. 2019, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.O.; Unroe, K.T.; Xu, H.; Keith, N.R.; Callahan, C.M.; Tu, W. Sex and race differences in the relationship between obesity and C-reactive protein. Ethn. Dis. 2016, 26, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Choi, O.J.; Cho, Y.G.; Kang, J.H.; Park, H.A.; Kim, K.W.; Hur, Y.I.; Yim, H.J. Weight control attempts in underweight korean adults: Korea National Health and Nutrition Examination Survey, 2007–2010. Korean J. Fam. Med. 2013, 34, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.Y.; Kang, H.T. Recent trends in the prevalence of underweight, overweight, and obesity in Korean adults: The Korean National Health and Nutrition Examination Survey from 1998 to 2014. J. Epidemiol. 2017, 27, 413–419. [Google Scholar] [CrossRef]
- Messier, V.; Rabasa-Lhoret, R.; Barbat-Artigas, S.; Elisha, B.; Karelis, A.D.; Aubertin-Leheudre, M. Menopause and sarcopenia: A potential role for sex hormones. Maturitas 2011, 68, 331–336. [Google Scholar] [CrossRef]
- Gligoroska, J.P.; Todorovska, L.; Mancevska, S.; Karagjozova, I.; Petrovska, S. Biolectrical impedance analysis in karate athletes: BIA parameters obtained with InBody 720 regarding the age. Res. Phys. Educ. Sport Health 2016, 5, 117–121. [Google Scholar]
- Saito, M.; Seshimo, A.; Miyake, K.; Yamaguchi, R.; Okamoto, T. Efficiency of bioelectric impedance analysis as an evaluation method of skeletal muscle mass after gastrectomy. Int. Surg. 2018, 102, 422–426. [Google Scholar] [CrossRef]
- Chertow, G.M. Estimates of body composition as intermediate outcome variables: Are DEXA and BIA ready for prime time? J. Ren. Nutr. 1999, 9, 138–141. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Men (n = 160,664) | Women (n = 139,426) | p Value |
|---|---|---|---|
| Age (years) | 40.3 (9.4) | 39.4 (10.2) | <0.01 |
| Height (cm) | 173.1 (5.8) | 160.3 (5.3) | <0.01 |
| Weight (kg) | 73.4 (10.2) | 56.1 (8.2) | <0.01 |
| Body mass index (kg/m2) | 24.4 (2.9) | 21.8 (3.1) | <0.01 |
| Waist circumference (cm) | 86.2 (7.9) | 76.2 (8.3) | <0.01 |
| Fat mass (kg) | 17.2 (6.0) | 17.0 (5.7) | <0.01 |
| Skeletal muscle mass (kg) | 31.4 (3.6) | 21.3 (2.3) | <0.01 |
| SMI (%) 1 | 42.8 (3.0) | 38.2 (3.4) | <0.01 |
| SBP (mmHg) | 113.2 (11.5) | 100.9 (11.6) | <0.01 |
| DBP (mmHg) | 73.9 (9.4) | 64.9 (8.7) | <0.01 |
| Total cholesterol (mg/dL) | 199.3 (34.5) | 188.4 (33.0) | <0.01 |
| Triglycerides (mg/dL) | 114 (81–164) | 71 (54–98) | <0.01 |
| LDL-C (mg/dL) | 126.8 (31.4) | 110.9 (30.2) | <0.01 |
| HDL-C (mg/dL) | 52.6 (12.8) | 64.5 (14.8) | <0.01 |
| Fasting glucose (IU/L) | 95 (90–102) | 91 (86–96) | <0.01 |
| Creatinine (mg/dL) | 1.0 (0.9–1.1) | 0.7 (0.6–0.8) | <0.01 |
| ALT (U/L) | 29.1 (24.1) | 15.8 (14.3) | <0.01 |
| hs-CRP (mg/L) | 0.05 (0.03–0.10) | 0.03 (0.02–0.07) | <0.01 |
| Total vitamin D (nmol/L) | 17.6 (6.7) | 14.2 (6.6) | <0.01 |
| Hypertension (%) | 12.4 | 5.8 | <0.01 |
| Hyperlipidemia (%) | 17.7 | 8.5 | <0.01 |
| Diabetes mellitus (%) | 4.0 | 1.7 | <0.01 |
| Current smoker (%) | 37.0 | 2.6 | <0.01 |
| Heavy drinking (%) | 28.5 | 3.8 | <0.01 |
| Regular physical activity (%) | 14.8 | 12.6 | <0.01 |
| Age subgroups (years) | |||
| 20–29 (n) | 10,359 | 15,858 | |
| 30–39 (n) | 72,178 | 64,671 | |
| 40–49 (n) | 53,269 | 37,427 | |
| 50–59 (n) | 17,671 | 14,359 | |
| 60–69 (n) | 5792 | 5800 | |
| 70–79 (n) | 1325 | 1254 | |
| ≥80 (n) | 70 | 57 |
| Young Men | Young Women | |
|---|---|---|
| No. of participants (n) | 82,537 | 80,529 |
| Mean value of SMI (%) | 42.9 (3.1) | 38.7 (3.2) |
| SMI cutoff levels (%) of sarcopenia | ||
| Class I sarcopenia | 39.8 | 35.5 |
| Class II sarcopenia | 36.7 | 32.3 |
| Age Adjusted OR | Model 1 | Model 2 | |
|---|---|---|---|
| All | |||
| Normal body composition | 1 (reference) | 1 (reference) | 1 (reference) |
| Class I sarcopenia | 3.76 (3.66–3.86) | 2.42 (2.33–2.52) | 2.43 (2.33–2.54) |
| Class II sarcopenia | 6.82 (6.51–7.15) | 2.62 (2.45–2.80) | 2.69 (2.49–2.91) |
| Men | |||
| Normal body composition | 1 (reference) | 1 (reference) | 1 (reference) |
| Class I sarcopenia | 4.20 (4.06–4.35) | 3.48 (3.33–3.64) | 2.36 (2.25–2.49) |
| Class II sarcopenia | 7.39 (6.93–7.87) | 5.36 (4.96–5.80) | 2.57 (2.34–2.82) |
| Women | |||
| Normal body composition | 1 (reference) | 1 (reference) | 1 (reference) |
| Class I sarcopenia | 4.46 (4.23–4.69) | 4.56 (4.26–4.88) | 2.87 (2.62–3.16) |
| Class II sarcopenia | 8.76 (8.12–9.45) | 8.55 (7.74–9.45) | 3.17 (2.76–3.64) |
| Men | Women | |
|---|---|---|
| Present study | ||
| Class I | 39.8 | 35.5 |
| Class II | 36.7 | 32.3 |
| Janssen et al. [3] from US | ||
| Class I | 37.0 | 28.0 |
| Class II | 31.0 | 22.0 |
| Bahat et al. [40] from Turkey | ||
| Class I | 40.4 | 37.2 |
| Class II | 37.4 | 33.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.-H.; Do, J.G.; Lee, Y.-T.; Yoon, K.J. Sex Difference in Cutoff and Prevalence of Sarcopenia among 300,090 Urban Korean Population: Association with Metabolic Syndrome. Medicina 2022, 58, 1361. https://doi.org/10.3390/medicina58101361
Park C-H, Do JG, Lee Y-T, Yoon KJ. Sex Difference in Cutoff and Prevalence of Sarcopenia among 300,090 Urban Korean Population: Association with Metabolic Syndrome. Medicina. 2022; 58(10):1361. https://doi.org/10.3390/medicina58101361
Chicago/Turabian StylePark, Chul-Hyun, Jong Geol Do, Yong-Taek Lee, and Kyung Jae Yoon. 2022. "Sex Difference in Cutoff and Prevalence of Sarcopenia among 300,090 Urban Korean Population: Association with Metabolic Syndrome" Medicina 58, no. 10: 1361. https://doi.org/10.3390/medicina58101361