
Evidence for the Efficacy of a High Dose of Vitamin D on the Hyperinflammation State in Moderate-to-Severe COVID-19 Patients: A Randomized Clinical Trial

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Methods
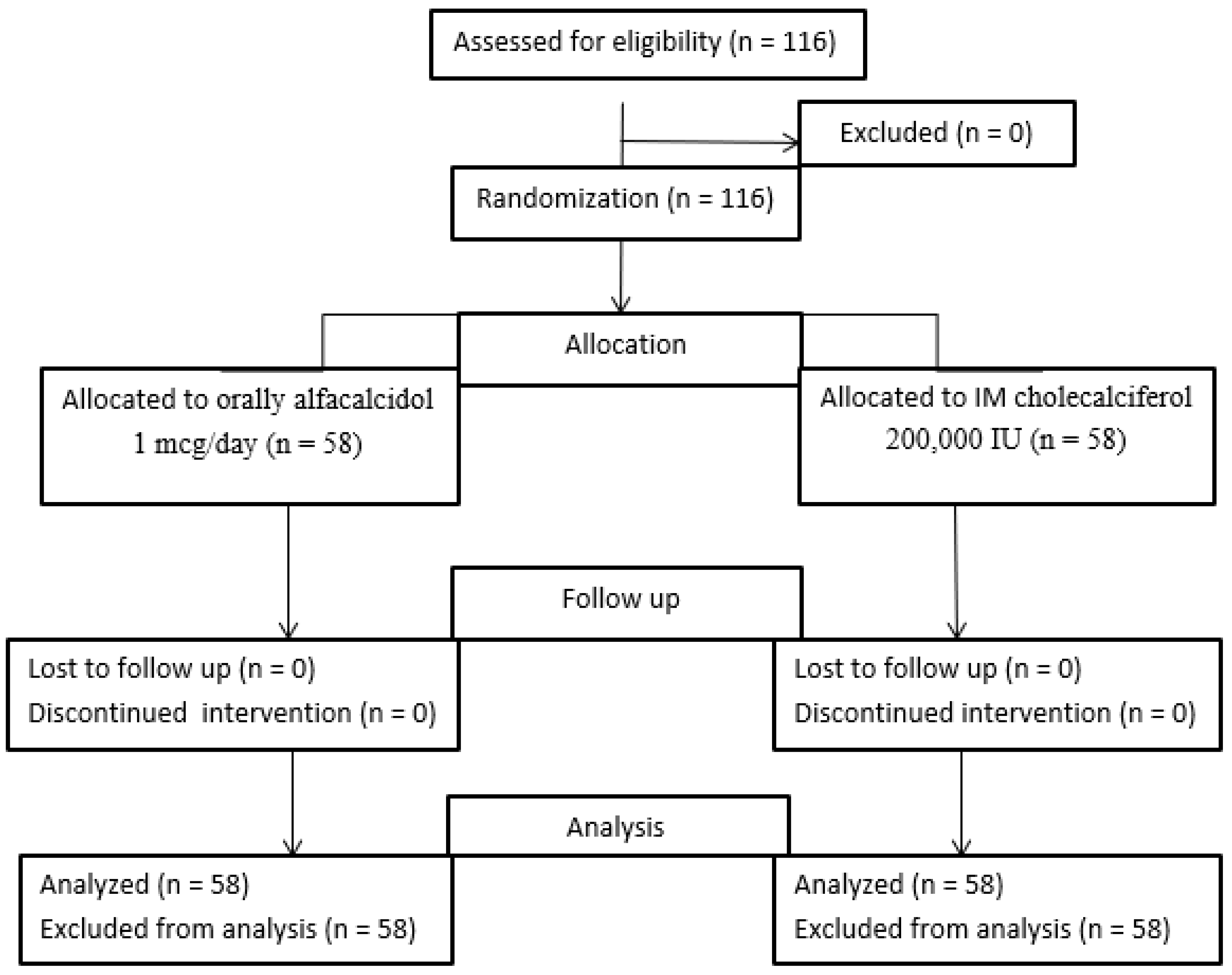
2.1. Study Design and Patients
2.2. Eligibility Criteria
2.3. Treatment
2.4. Study Outcomes
2.5. Sample Size Calculation
2.6. Biochemical Analysis
2.7. Statistical Analysis
3. Results
3.1. Baseline Patients’ Characteristics
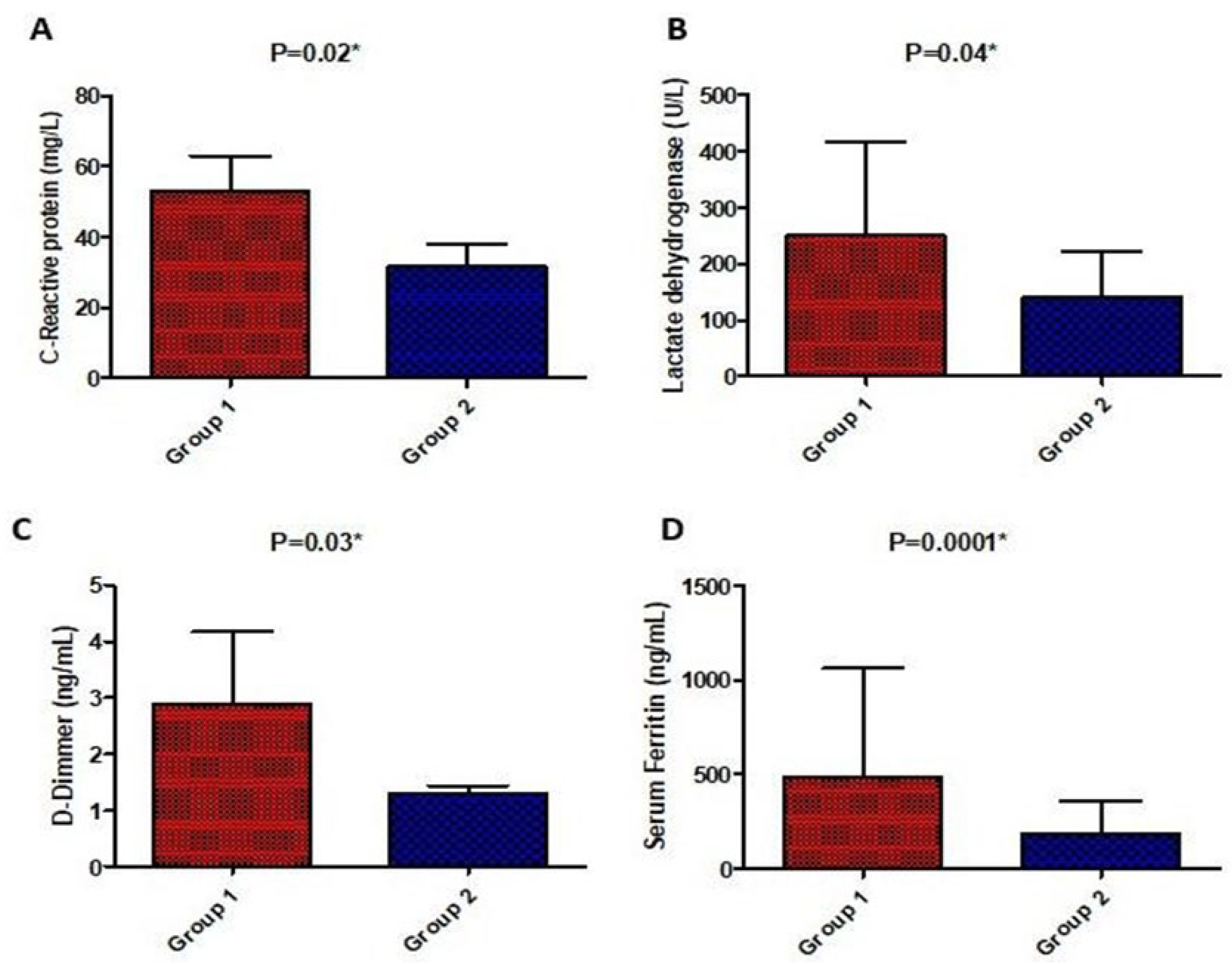
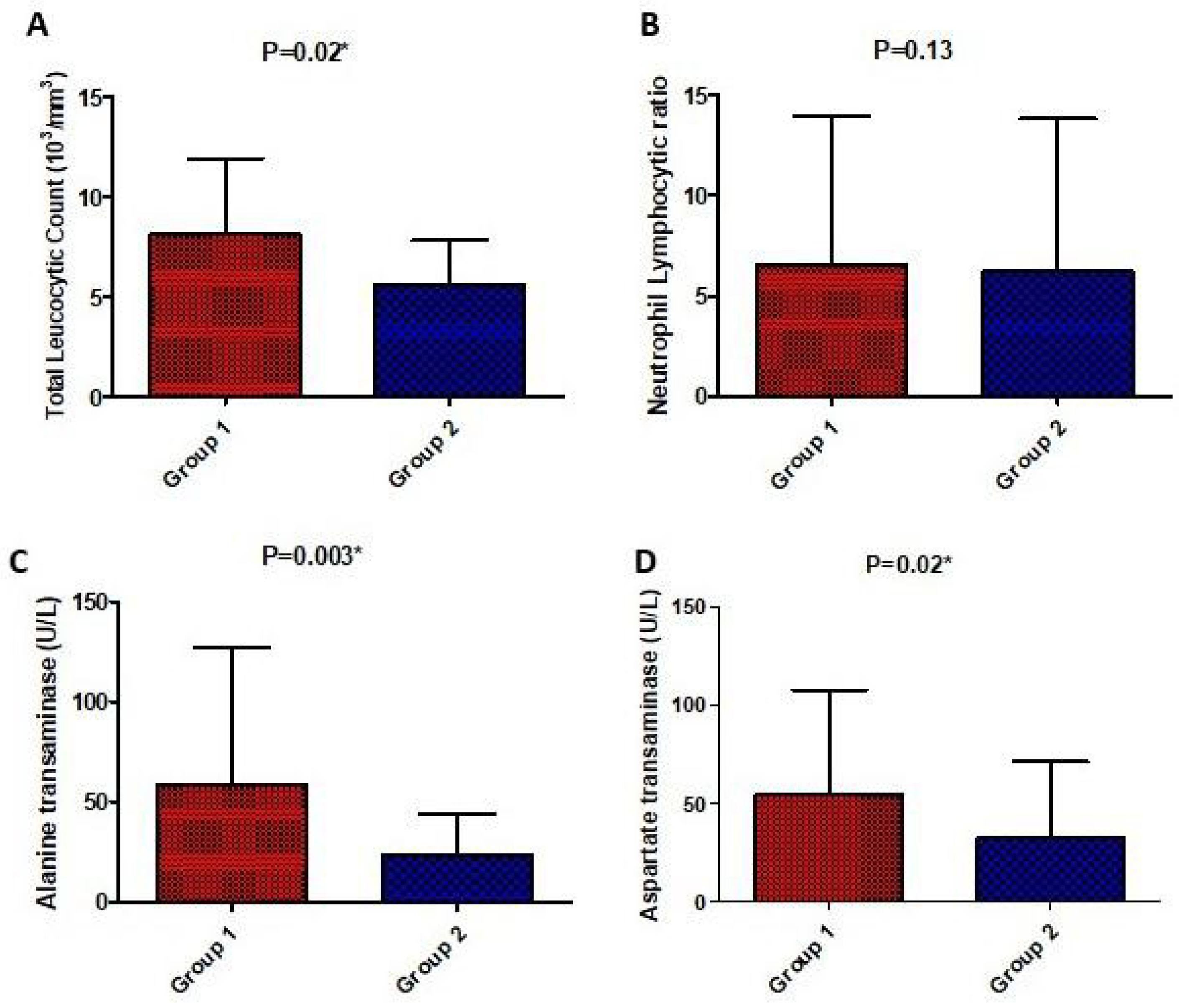
3.2. Changes in Biochemical Parameters between Both Groups
3.3. Impact of Both Treatment Arms on the Clinical Outcomes
3.4. Predictors of Clinical Improvement by Binary Logistic Regression Analysis
3.5. Predictors of Mortality by Binary Logistic Regression Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factor | Odd Ratio | 95%CI | p-Value |
|---|---|---|---|
| Need for low oxygen | 0.16 | 0.05–0.53 | 0.002 * |
| Need for high oxygen/NIMV | 0.19 | 0.025–1.45 | 0.11 |
| Need for invasive MV | 4.93 | 1.1–12.56 | 0.039 * |
| ICU admission | 4.58 | 2.33–9.51 | 0.009 * |
| Hypertension | 1.42 | 0.15–1.21 | 0.11 |
| Diabetes | 1.37 | 0.33–5.56 | 0.45 |
| Heart failure | 1.42 | 0.14–2.31 | 0.42 |
| Chronic kidney disease | 0.63 | 0.31–5.45 | 0.71 |
| Chronic liver disease | 1.49 | 0.03–1.82 | 0.86 |
| Ischemic heart disease | 2.07 | 0.44– 9.76 | 0.35 |
| Atrial fibrillation | 2.39 | 1.7– 2.3 | 0.03 * |
| Chronic obstructive pulmonary disease | 1.93 | 1.7–7.4 | 0.015 * |
| Asthma | 3.07 | 2.4–8.9 | 0.023 * |
| Occurrence of secondary infection | 7.2 | 6.73–13.6 | 0.0003 * |
| Vitamin D dose (high/low) | 0.73 | 0.63–0.83 | 0.002 * |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): A global pandemic and treatment strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef] [PubMed]
- Schaalan, M.; Warda, A.E.A.; Osman, S.M.; Fathy, S.; Sarhan, R.M.; Boshra, M.S.; Sarhan, N.; Gaber, S.; Ali, A.M.A. The Impact of Sociodemographic, Nutritional, and Health Factors on the Incidence and Complications of COVID-19 in Egypt: A Cross-Sectional Study. Viruses 2022, 14, 448. [Google Scholar] [CrossRef] [PubMed]
- Baktash, V.; Hosack, T.; Patel, N.; Shah, S.; Kandiah, P.; van den Abbeele, K.; Mandal, A.K.J.; Missouris, C.G. Vitamin D status and outcomes for hospitalized older patients with COVID-19. Postgrad. Med. J. 2021, 97, 442–447. [Google Scholar] [PubMed]
- De La Puente-Yagüe, M.; Cuadrado-Cenzual, M.A.; Ciudad-Cabañas, M.J.; Hernández-Cabria, M.; Collado-Yurrita, L. Vitamin D: And its role in breast cancer. Kaohsiung J. Med. Sci. 2018, 34, 423–427. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2022, 62, 1308–1310. [Google Scholar] [CrossRef]
- Annweiler, C.; Legrand, E.; Souberbielle, J.C. Vitamin D in adults: Update on testing and supplementation. Geriatr. Psychol. Neuropsychiatr. Vieil. 2018, 16, 7–22. [Google Scholar] [CrossRef]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Gil, Á.; Plaza-Diaz, J.; Mesa, M.D. Vitamin D: Classic and novel actions. Ann. Nutr. Metab. 2018, 72, 87–95. [Google Scholar] [CrossRef]
- Bayraktar, N.; Turan, H.; Bayraktar, M.; Ozturk, A.; Erdoğdu, H. Analysis of serum cytokine and protective vitamin D levels in severe cases of COVID-19. J. Med. Virol. 2022, 94, 154–160. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O’Keefe, J.H. Magnesium and vitamin D deficiency as a potential cause of immune dysfunction, cytokine storm, and disseminated intravascular coagulation in COVID-19 patients. Mo. Med. 2021, 118, 68. [Google Scholar]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Zhu, X.; Shi, Y.; Liu, T.; Chen, Y.; Bhan, I.; Zhao, Q.; Thadhani, R.; Li, Y.C. VDR attenuates acute lung injury by blocking Ang-2-Tie-2 pathway and renin-angiotensin system. Mol. Endocrinol. 2013, 27, 2116–2125. [Google Scholar] [CrossRef]
- Yuan, W.; Pan, W.; Kong, J.; Zheng, W.; Szeto, F.L.; Wong, K.E.; Cohen, R.; Klopot, A.; Zhang, Z.; Li, Y.C. 1,25- Dihydroxyvitamin D3 suppresses renin gene transcription by blocking the activity of the cyclic AMP response element in the renin gene promoter. J. Biol. Chem. 2007, 282, 29821–29830. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Dijkman, R.; Jebbink, M.F.; Deijs, M.; Milewska, A.; Pyrc, K.; Buelow, E.; Van Der Bijl, A.; Van Der Hoek, L. Replication-dependent downregulation of cellular angiotensin-converting enzyme 2 protein expression by human coronavirus NL63. J. Gen. Virol. 2012, 93 Pt 9, 1924–1929. [Google Scholar] [CrossRef]
- Ji, X.; Zhang, C.; Zhai, Y.; Zhang, Z.; Zhang, C.; Xue, Y.; Tan, G.; Niu, G. TWIRLS, an automated topic-wise inference method based on massive literature, suggests a possible mechanism via ACE2 for the pathological changes in the human host after coronavirus infection. bioRxiv 2020. [Google Scholar] [CrossRef]
- Chen, I.Y.; Chang, S.C.; Wu, H.Y.; Yu, T.C.; Wei, W.C.; Lin, S.; Chien, C.-L.; Chang, M.-F. Upregulation of the chemokine (C-C motif) ligand 2 via a severe acute respiratory syndrome coronavirus spike-ACE2 signaling pathway. J. Virol. 2010, 84, 7703–7712. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, H.; Xu, J. Effect of vitamin D on ACE2 and vitamin D receptor expression in rats with LPS-induced acute lung injury. Chin. J. Emerg. Med. 2016, 25, 1284–1289. [Google Scholar]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D and its potential benefit for the COVID-19 pandemic. Endocr. Pract. 2021, 27, 484–493. [Google Scholar] [CrossRef]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.M.; Solway, J. Association of vitamin D levels, race/ethnicity, and clinical characteristics with COVID-19 test results. JAMA Netw. Open 2021, 4, e214117. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Sarhan, R.M.; Mohammad, M.F.; Boshra, M.S. Differential clinical diagnosis and prevalence rate of allergic rhinitis, asthma and chronic obstructive pulmonary disease among COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14532. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Nimavat, N.; Singh, A.K.; Ahmad, S.; Sinha, N. Prevalence of Low Level of Vitamin D Among COVID-19 Patients and Associated Risk Factors in India–A Hospital-Based Study. Int. J. Gen. Med. 2021, 14, 2523. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, H.B.; Yaktine, A.L.; Taylor, C.L.; Ross, A.C. (Eds.) Dietary Reference Intakes for Calcium and Vitamin D.; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Biesalski, H.K. Vitamin D deficiency and co-morbidities in COVID-19 patients–A fatal relationship? Nfs J. 2020, 20, 10. [Google Scholar] [CrossRef]
- Tan, C.W.; Ho, L.P.; Kalimuddin, S.; Cherng, B.P.Z.; Teh, Y.E.; Thien, S.Y.; Wong, H.M.; Tern, P.J.W.; Chandran, M.; Chay, J.W.M.; et al. Cohort study to evaluate the effect of vitamin D, magnesium, and vitamin B12 in combination on progression to severe outcomes in older patients with coronavirus (COVID-19). Nutrition 2020, 79, 111017. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Díaz, J.F.A.; Miranda, J.L.; Bouillon, R.; Gomez, J.M.Q. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid. Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Ling, S.F.; Broad, E.; Murphy, R.; Pappachan, J.M.; Pardesi-Newton, S.; Kong, M.F.; Jude, E.B. High-dose cholecalciferol booster therapy is associated with a reduced risk of mortality in patients with COVID-19: A cross-sectional multi-centre observational study. Nutrients 2020, 12, 3799. [Google Scholar] [CrossRef]
- Barrea, L.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D: A Role Also in Long COVID-19? Nutrients 2022, 14, 1625. [Google Scholar] [CrossRef]
- Campi, I.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D and COVID-19 severity and related mortality: A prospective study in Italy. BMC Infect. Dis. 2021, 21, 566. [Google Scholar] [CrossRef]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, e0239252. [Google Scholar] [CrossRef]
- Ghasemian, R.; Shamshirian, A.; Heydari, K.; Malekan, M.; Alizadeh-Navaei, R.; Ebrahimzadeh, M.A.; Warkiani, M.E.; Jafarpour, H.; Bazaz, S.R.; Shahmirzadi, A.R.; et al. The role of vitamin D in the age of COVID-19: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14675. [Google Scholar] [CrossRef]
- Dissanayake, H.A.; de Silva, N.L.; Sumanatilleke, M.; de Silva, S.D.N.; Gamage, K.K.K.; Dematapitiya, C.; Kuruppu, D.C.; Ranasinghe, P.; Pathmanathan, S.; Katulanda, P. Prognostic and therapeutic role of vitamin D in COVID-19: Systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2021, 107, 1484–1502. [Google Scholar] [CrossRef]
- Chen, J.; Mei, K.; Xie, L.; Yuan, P.; Ma, J.; Yu, P.; Zhu, W.; Zheng, C.; Liu, X. Low vitamin D levels do not aggravate COVID-19 risk or death, and vitamin D supplementation does not improve outcomes in hospitalized patients with COVID-19: A meta-analysis and GRADE assessment of cohort studies and RCTs. Nutr. J. 2021, 20, 89. [Google Scholar] [CrossRef]
- Annweiler, C.; Beaudenon, M.; Simon, R.; Guenet, M.; Otekpo, M.; Célarier, T.; Gautier, J.; GERIA-COVID Study Group. Vitamin D supplementation prior to or during COVID-19 associated with better 3-month survival in geriatric patients: Extension phase of the GERIA-COVID study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105958. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a single high dose of vitamin D3 on hospital length of stay in patients with moderate to severe COVID-19: A randomized clinical trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N.; Malhotra, P. Short term, high-dose vitamin D supplementation for COVID-19 disease: A randomised, placebo-controlled, study (SHADE study). Postgrad. Med. J. 2022, 98, 87–90. [Google Scholar] [CrossRef]
- Remmelts, H.H.; van de Garde, E.M.; Meijvis, S.C.; Peelen, E.L.; Damoiseaux, J.G.; Grutters, J.C.; Biesma, D.H.; Bos, W.J.; Rijkers, G.T. Addition of vitamin D status to prognostic scores improves the prediction of outcome in community-acquired pneumonia. Clin. Infect. Dis. 2012, 55, 1488–1494. [Google Scholar] [CrossRef]
- Infante, M.; Buoso, A.; Pieri, M.; Lupisella, S.; Nuccetelli, M.; Bernardini, S.; Fabbri, A.; Iannetta, M.; Andreoni, M.; Colizzi, V.; et al. Low Vitamin D status at admission as a risk factor for poor survival in hospitalized patients with COVID-19: An Italian retrospective study. J. Am. Coll. Nutr. 2022, 41, 250–265. [Google Scholar] [CrossRef]
- Lakkireddy, M.; Gadiga, S.G.; Malathi, R.D.; Karra, M.L.; Raju, I.S.S.V.; Chinapaka, S.; Baba, K.S.S.S.; Kandakatla, M. Impact of daily high dose oral vitamin D therapy on the inflammatory markers in patients with COVID 19 disease. Sci. Rep. 2021, 11, 10641. [Google Scholar] [CrossRef]
- Annweiler, C.; Beaudenon, M.; Gautier, J.; Simon, R.; Dubée, V.; Gonsard, J.; Parot-Schinkel, E.; COVIT-TRIAL Study Group. COvid-19 and high-dose VITamin D supplementation TRIAL in high-risk older patients (COVIT-TRIAL): Study protocol for a randomized controlled trial. Trials 2020, 21, 1031. [Google Scholar] [CrossRef]
- Mariani, J.; Tajer, C.; Antonietti, L.; Inserra, F.; Ferder, L.; Manucha, W. High-dose vitamin D versus placebo to prevent complications in COVID-19 patients: A structured summary of a study protocol for a randomised controlled trial (CARED-TRIAL). Trials 2021, 22, 111. [Google Scholar] [CrossRef]




| Variable | Group 1 (Low-Dose Vitamin D) n = 58 | Group 2 (High-Dose Vitamin D) n = 58 | Significance p < 0.05 |
|---|---|---|---|
| Age (mean ± SD) | 65.7 ± 12.6 | 66.1 ± 11.2 | p = 0.16 |
| Male gender (n) | 46 | 38 | p = 0.07 |
| Oxygenation (mean ± SD) | |||
| Oxygen saturation | 88.3 ± 8.8 | 86.4 ± 13.4 | p = 0.2 |
| P/F ratio | 197.3 ± 112.8 | 180.8 ± 99.7 | p = 0.56 |
| Respiratory rate | 24.2 ± 4.4 | 25.9 ± 5.7 | p = 0.21 |
| Biochemical markers (mean ± SD) | |||
| Baseline C- reactive protein (CRP) | 120.5 ± 100.4 | 145.5 ± 101.2 | p = 0.18 |
| Baseline interleukin-6 (IL-6) | 15.7 ± 2.3 | 17.1 ± 1.6 | p = 0.21 |
| Baseline lactate dehydrogenase (LDH) | 350.1 ± 140.6 | 360.6 ± 136.5 | p = 0.72 |
| Baseline D-Dimer | 1.39 ± 1.8 | 1.1 ± 1.4 | p = 0.29 |
| Baseline ferritin | 886.5 ± 87.2 | 704.1 ± 59.3 | p = 0.17 |
| Serum creatinine | 1.26 ± 0.96 | 1.41 ± 0.59 | p = 0.31 |
| Total leucocytes count (TLC) | 7.8 ± 3.6 | 8.2 ± 3.9 | p = 0.60 |
| Neutrophil lymphocytic ratio (NLR) | 9.8 ± 8.8 | 7.2 ± 3.8 | p = 0.06 |
| Alanine transaminase (ALT) | 52.1 ± 6.7 | 41.6 ± 3.2 | p = 0.29 |
| Aspartate transaminase (AST) | 52.6 ± 4.3 | 45.2 ± 3.1 | p = 0.28 |
| Comorbidities (n) | |||
| Hypertension | 31 | 31 | p = 0.57 |
| Diabetes | 22 | 23 | p = 0.6 |
| Heart failure | 0 | 2 | p = 0.25 |
| Chronic kidney disease | 4 | 0 | p = 0.07 |
| Chronic liver disease | 2 | 0 | p = 25 |
| Ischemic heart disease | 10 | 10 | p = 0.6 |
| Atrial fibrillation | 4 | 0 | p = 0.07 |
| Asthma | 0 | 2 | p = 0.24 |
| Chronic obstructive pulmonary disease | 2 | 2 | p = 0.67 |
| Medications (n) | |||
| Hydroxychloroquine | 10 | 12 | p = 0.15 |
| Remdesivir | 50 | 58 | p = 0.12 |
| Lopinavir/ritonavir | 15 | 21 | p = 0.23 |
| Ivermectin | 15 | 13 | p = 0.41 |
| Infliximab | 58 | 56 | p = 0.828 |
| Tocilizumab | 46 | 50 | p = 0.34 |
| Variable | Group 1 (Low-Dose Vitamin D) n = 58 | Group 2 (High-Dose Vitamin D) n = 58 | Significance |
|---|---|---|---|
| Primary Outcomes | |||
| Clinical improvement (%); | ꭓ2 = 4.7 | ||
| No/Yes | 71/29 | 45/55 | p = 0.03 * |
| Need for low oxygen (%); | ꭓ2 = 0.16 | ||
| No/Yes | 49/51 | 53/47 | p = 0.42 |
| Need for NIMV (%); | χ2 = 2.21 | ||
| No/Yes | 67/33 | 33/67 | p = 0.03 * |
| Need for invasive MV (%); | χ2 = 3.1 | ||
| No/Yes | 33/67 | 75/25 | p = 0.03 * |
| Oxygen saturation | 88.4 ± 8.3 | 95.2 ± 5.7 | p = 0.04 * |
| Respiratory rate | 16.9 ± 5.7 | 14.2 ± 4.4 | p = 0.38 |
| P/F ratio | 321 ± 97.3 | 156.1 ± 58.9 | p = 0.003 * |
| Secondary Outcomes | |||
| ICU admission (%); | χ2 = 5.5 | ||
| No/Yes | 35/65 | 58/42 | p = 0.016 * |
| Death (%); | χ2 = 1.4 | ||
| No/Yes | 49/51 | 55/45 | p = 0.49 |
| Occurrence of sepsis (%); | χ2 = 4.1 | ||
| No/Yes | 36/64 | 67/33 | p = 0.04 * |
| Length of hospital stay | 8.9 ± 5.1 | 6.1 ± 3.4 | p = 0.04 * |
| Time to improvement | 8.8 ± 4.7 | 6.27 ± 2.5 | p = 0.002 * |
| Risk Factor | Odd Ratio | 95%CI | p-Value |
|---|---|---|---|
| Need for low oxygen | 6.67 | 2.07–21.35 | 0.001 * |
| Need for high oxygen/NIMV | 0.19 | 0.41–0.86 | 0.03 * |
| Need for invasive MV | 0.83 | 0.64–0.98 | 0.01 * |
| ICU admission | 0.24 | 0.45–11.1 | 0.81 |
| Hypertension | 0.55 | 0.91–7.14 | 0.074 |
| Diabetes | 0.37 | 0.33–0.56 | 0.04 * |
| Heart failure | 0.719 | 0.65–1.79 | 0.94 |
| Chronic kidney disease | 0.63 | 0.31–5.45 | 0.71 |
| Chronic liver disease | 0.71 | 0.64–0.79 | 0.58 |
| Ischemic heart disease | 0.45 | 0.07–2.11 | 0.31 |
| Atrial fibrillation | 0.41 | 0.15–0.38 | 0.008 * |
| Chronic obstructive pulmonary disease | 0.85 | 0.09–8.4 | 0.98 |
| Asthma | 0.30 | 0.04–2.5 | 0.45 |
| Occurrence of secondary infection | 0.33 | 0.16–0.94 | 0.004 * |
| Vitamin D dose (high/low) | 4.3 | 3.2–6.9 | 0.001 * |
| Variables | Adjusted OR | Adjusted 95%CI | Adjusted p-Value |
|---|---|---|---|
| Factors associated with clinical improvement | |||
| Need for low oxygen | 5.35 | 2.41–15.12 | 0.005 * |
| Need for high oxygen/NIMV | 0.23 | 0.31–0.78 | 0.041 * |
| Need for invasive MV | 0.71 | 0.58–0.81 | 0.038 * |
| Diabetes | 0.42 | 0.28–0.74 | 0.048 * |
| Occurrence of secondary infection | 0.46 | 0.31–0.83 | 0.02 * |
| Vitamin D dose (high/low) | 3.9 | 2.4–5.7 | 0.03 * |
| Factors associated with clinical mortality | |||
| Need for invasive MV | 5.01 | 3.6–10.9 | 0.002 * |
| ICU admission | 6.4 | 3.71–11.4 | 0.009 * |
| Atrial fibrillation | 3.1 | 2.09–4.2 | 0.041 * |
| Chronic obstructive pulmonary disease | 1.82 | 1.3–8.9 | 0.03 * |
| Occurrence of secondary infection | 3.3 | 2.8–11.6 | 0.009 * |
| Vitamin D dose (high/low) | 0.68 | 0.59–0.81 | 0.003 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarhan, N.; Abou Warda, A.E.; Sarhan, R.M.; Boshra, M.S.; Mostafa-Hedeab, G.; ALruwaili, B.F.; Ibrahim, H.S.G.; Schaalan, M.F.; Fathy, S. Evidence for the Efficacy of a High Dose of Vitamin D on the Hyperinflammation State in Moderate-to-Severe COVID-19 Patients: A Randomized Clinical Trial. Medicina 2022, 58, 1358. https://doi.org/10.3390/medicina58101358
Sarhan N, Abou Warda AE, Sarhan RM, Boshra MS, Mostafa-Hedeab G, ALruwaili BF, Ibrahim HSG, Schaalan MF, Fathy S. Evidence for the Efficacy of a High Dose of Vitamin D on the Hyperinflammation State in Moderate-to-Severe COVID-19 Patients: A Randomized Clinical Trial. Medicina. 2022; 58(10):1358. https://doi.org/10.3390/medicina58101358
Chicago/Turabian StyleSarhan, Neven, Ahmed E. Abou Warda, Rania M. Sarhan, Marian S. Boshra, Gomaa Mostafa-Hedeab, Bashayer F. ALruwaili, Haytham Soliman Ghareeb Ibrahim, Mona F. Schaalan, and Shaimaa Fathy. 2022. "Evidence for the Efficacy of a High Dose of Vitamin D on the Hyperinflammation State in Moderate-to-Severe COVID-19 Patients: A Randomized Clinical Trial" Medicina 58, no. 10: 1358. https://doi.org/10.3390/medicina58101358