1. Introduction
The atrial septal defect is, after bicuspid aortic valve disease, the most common congenital cardiac disease present in adult populations. The most common atrial septal defects are the ostium secundum type (75–80%), followed by ostium primum (15%). The sinus venosus atrial septal defects (SV-ASD), defined as a communication in the posterior part of the interatrial septum, account for about 5 to 10% of atrial septal defects [
1,
2,
3,
4]. Approximately 90% of SV-ASDs are associated with partial anomalous pulmonary venous drainage (PAPVD) and are traditionally repaired through a full sternotomy [
5]. The typical superior SV-ASD variant occurs in the upper posterior atrial septum (rostral and posterior to the fossa ovalis) and results from the communication between the superior vena cava (SVC)–right atrial junction and the left atrium, being almost always associated with anomalous pulmonary venous drainage (usually from the right upper and middle lung lobes into the SVC). Due to the position of the defect, sinoatrial node abnormalities are frequently associated [
6,
7,
8,
9,
10].
Inferior SV-ASDs occur less commonly, in the postero-inferior portion of the septum, resulting, in this case, from anomalous communication of the right atrium and inferior vena cava with the left atrium. Atrial septal defects affect females more often than males. The diagnosis is usually made with echocardiography, this being the preferred method [
11,
12,
13].
ASDs were traditionally treated through median sternotomy, with well-known disadvantages. The minimal approach reduces blood loss, postoperative mechanical ventilation time, duration of intensive care stay, and overall hospitalization time. The cosmetical results are also superior [
5].
2. Case Report
We describe the case of a 45-year-old woman diagnosed in adolescence with a sinus venosus atrial septal defect (SV-ASD) with partial anomalous pulmonary venous drainage (PAPVD). After postponing the surgical treatment due to fear of surgical intervention, the patient presented with shortness of breath and fatigue after heavy exertions, episodes of paroxysmal nocturnal dyspnea, palpitations both during effort and at rest and had a history of syncope dating from 17 years previously. A series of tests were carried out to determine whether the patient was fit to undergo cardiac surgery to close the septal defect. The patient was diagnosed with heart failure NYHA (New York Heart association) functional class III.
During the physical examination, the patient presented with a typical “gracile habitus”, being thin for her height, with normal skin color and a 95% blood oxygen saturation. She had normal blood pressure (119/80 mmHg) and a good volume pulse. The patient also had a loud S1 and an ejection systolic murmur in the Erb’s point. The jugular venous pressure was not particularly elevated and the chest X-ray was clear. Blood tests showed a hemoglobin concentration of 14.4 g/dL and a normal brain natriuretic peptide concentration of 22.4 pg/mL. There was no evidence of decompensated heart failure or peripheral oedema.
The patient’s preoperative electrocardiography (ECG) at rest demonstrated an inferior atrial rhythm, a right QRS axis deviation (+100 degrees), a narrow QRS complex and a minor right bundle-branch block. The abnormal P-wave axis (negative in leads DII, DIII and aVF) indicated that the depolarization of the atrium was not initiated in the sinus node (ectopic atrial rhythm), suggesting an underlying sinus node disease. The chest X-ray showed no evidence of cardiomegaly, which would have been a prognostic marker for a poor chance of survival.
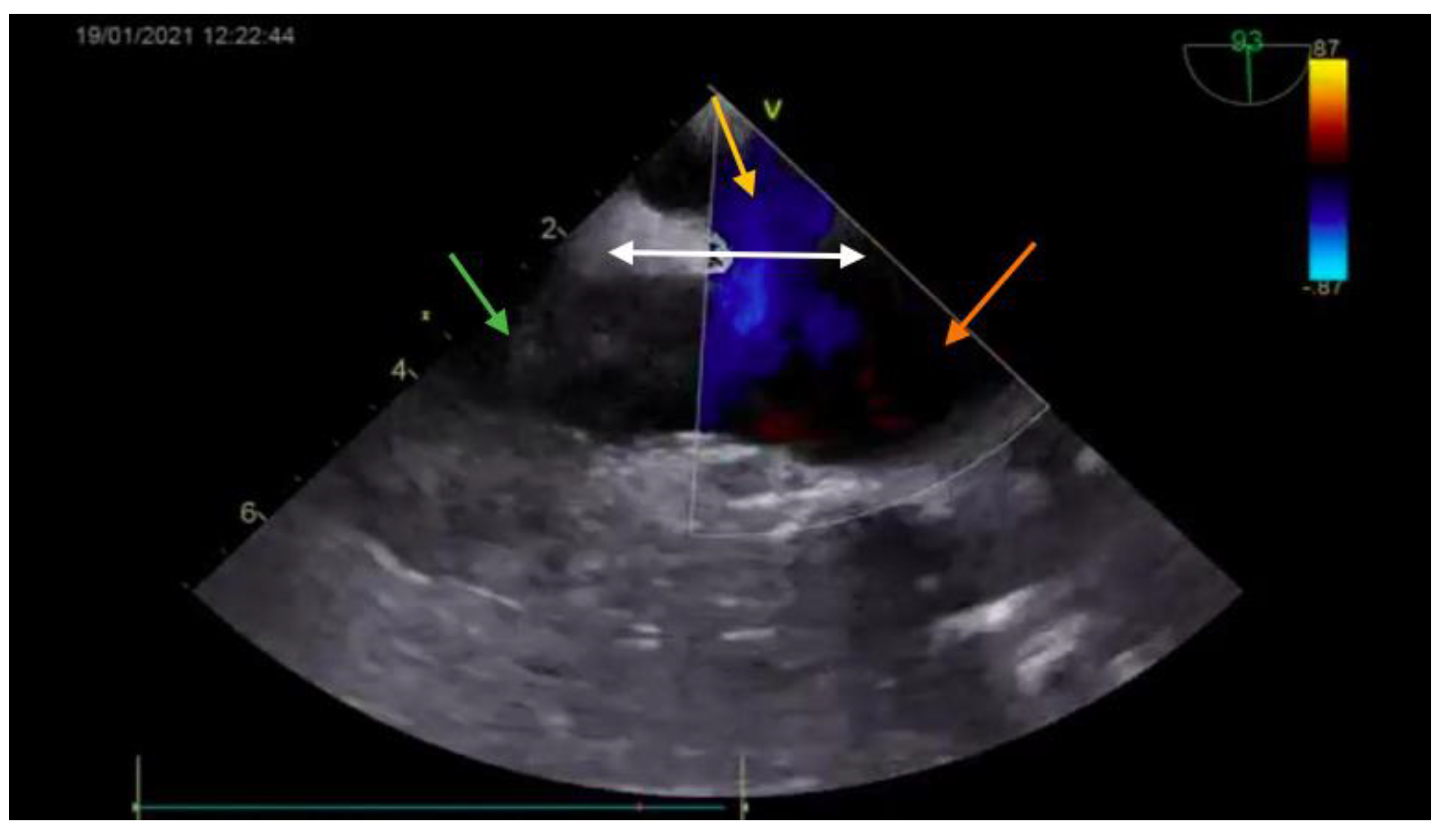
The diagnosis was based on the transthoracic echocardiography (
Figure 1 and
Figure 2). It revealed an SV-ASD with PAPVD which appeared to open in the right atrium, a dilated right atrium and ventricle, and a left-to-right shunt with Qp:Qs of 2.3 (Qp-pulmonary flow/Qs-systemic flow). The patient had normal pulmonary artery pressure, which was measured during echocardiography.
After careful examination, the patient was deemed fit to undergo cardiac surgery. Given the cosmetic concerns of the patient and considering her young age, a minimally invasive approach was preferred.
The incision was made in the fourth right intercostal space. Cardiopulmonary bypass with aortic cross-clamping was used with bicaval and aortic peripheral cannulation. Cardiac arrest was induced with Brett-Schnider cardioplegia at moderate systemic hypothermia (at 32 degrees Celsius).
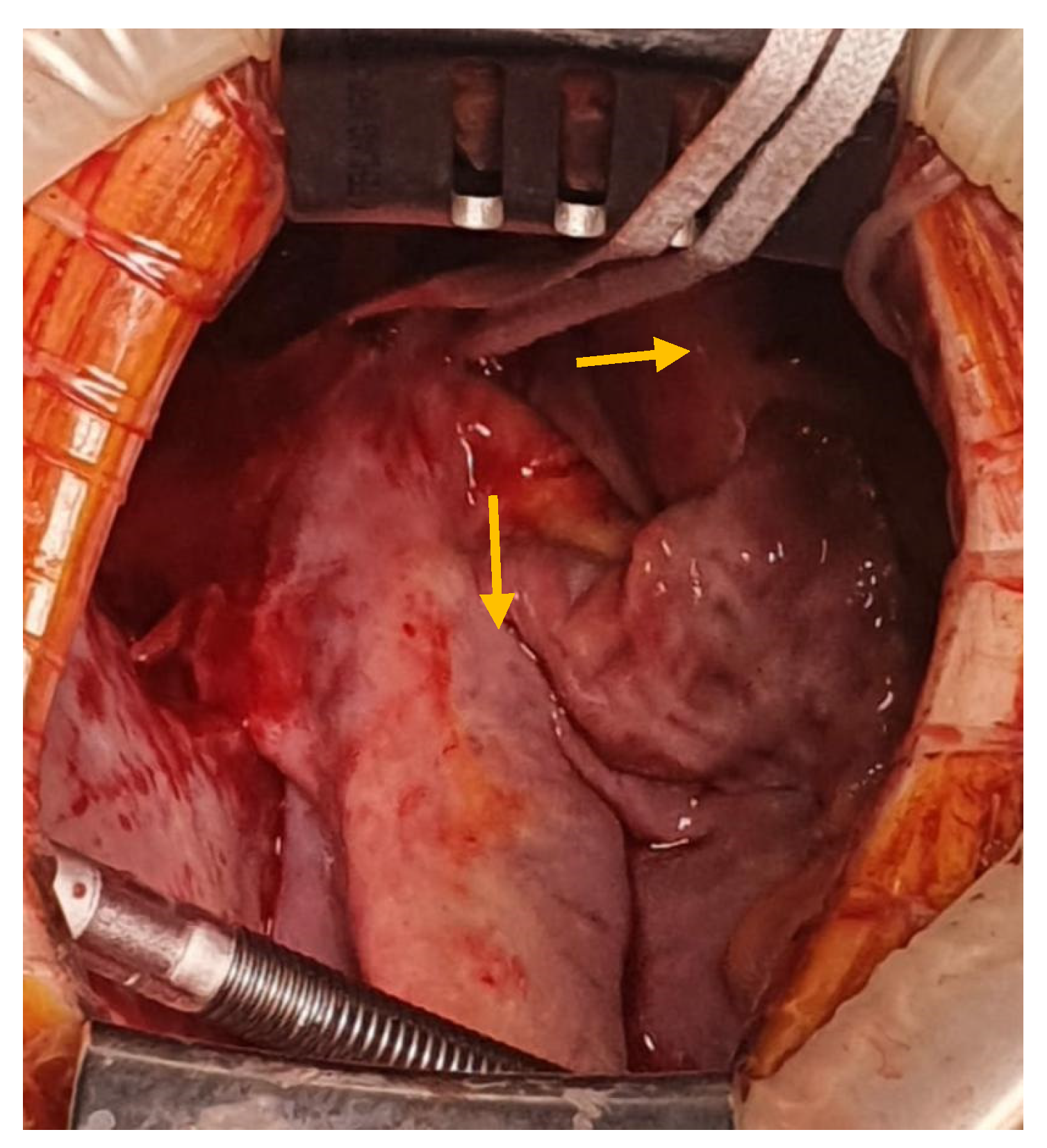
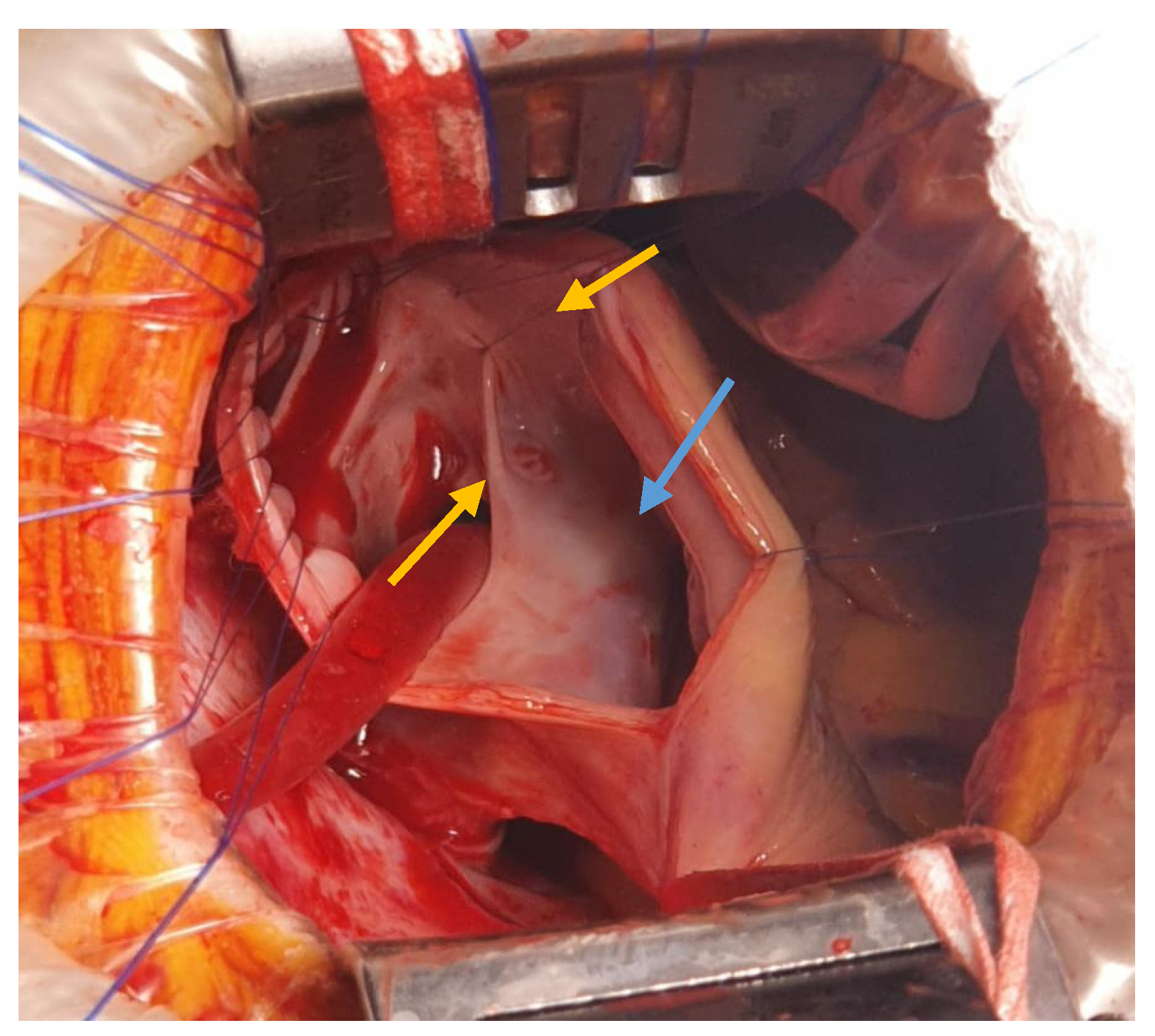
The interatrial defect was exposed through a right atriotomy extended across the cavoatrial junction into the superior vena cava. The examination of the right atrium cavity revealed an atrial septal defect in the proximity of the SVC and both right pulmonary veins draining into the SVC, proximally (
Figure 3 and
Figure 4).
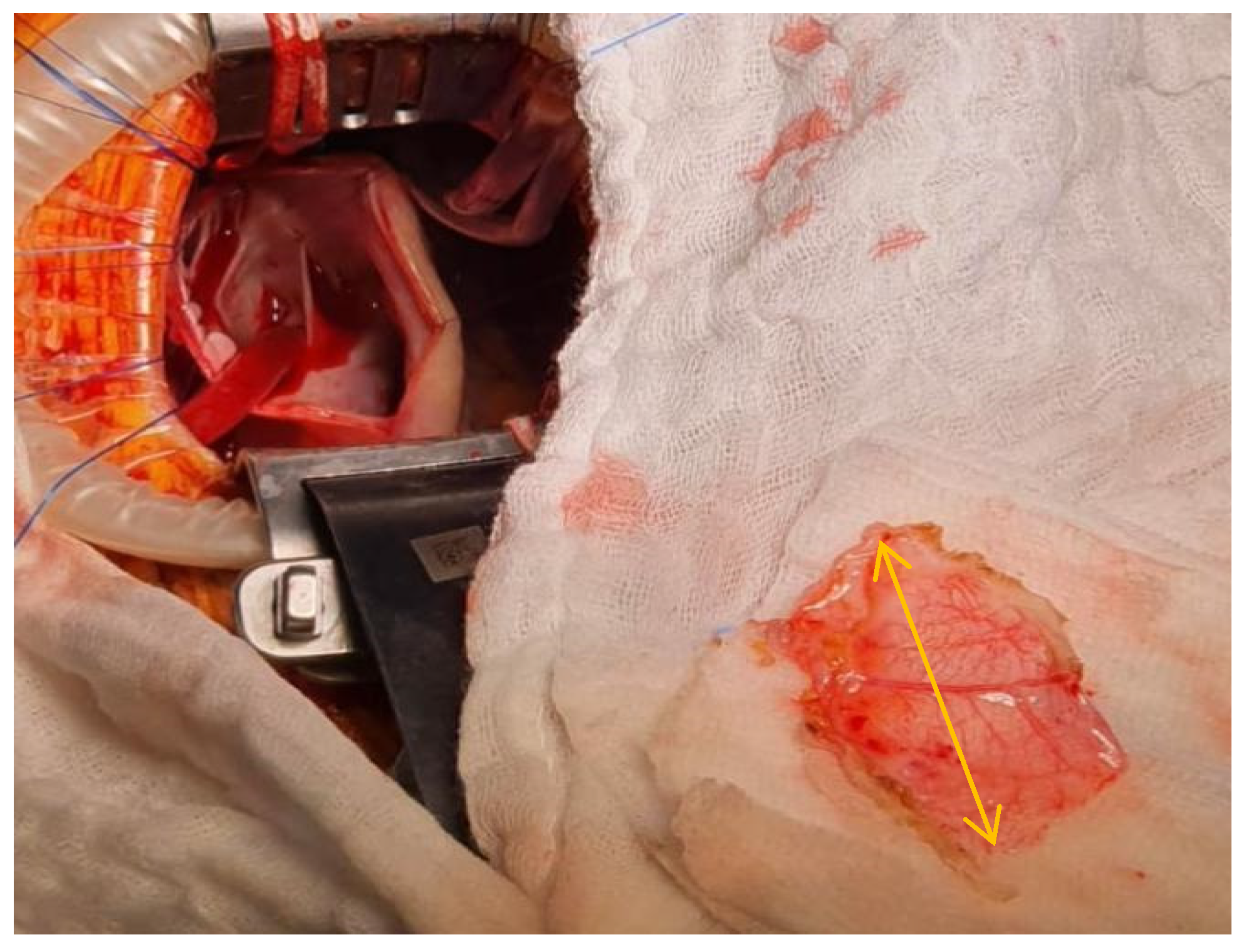
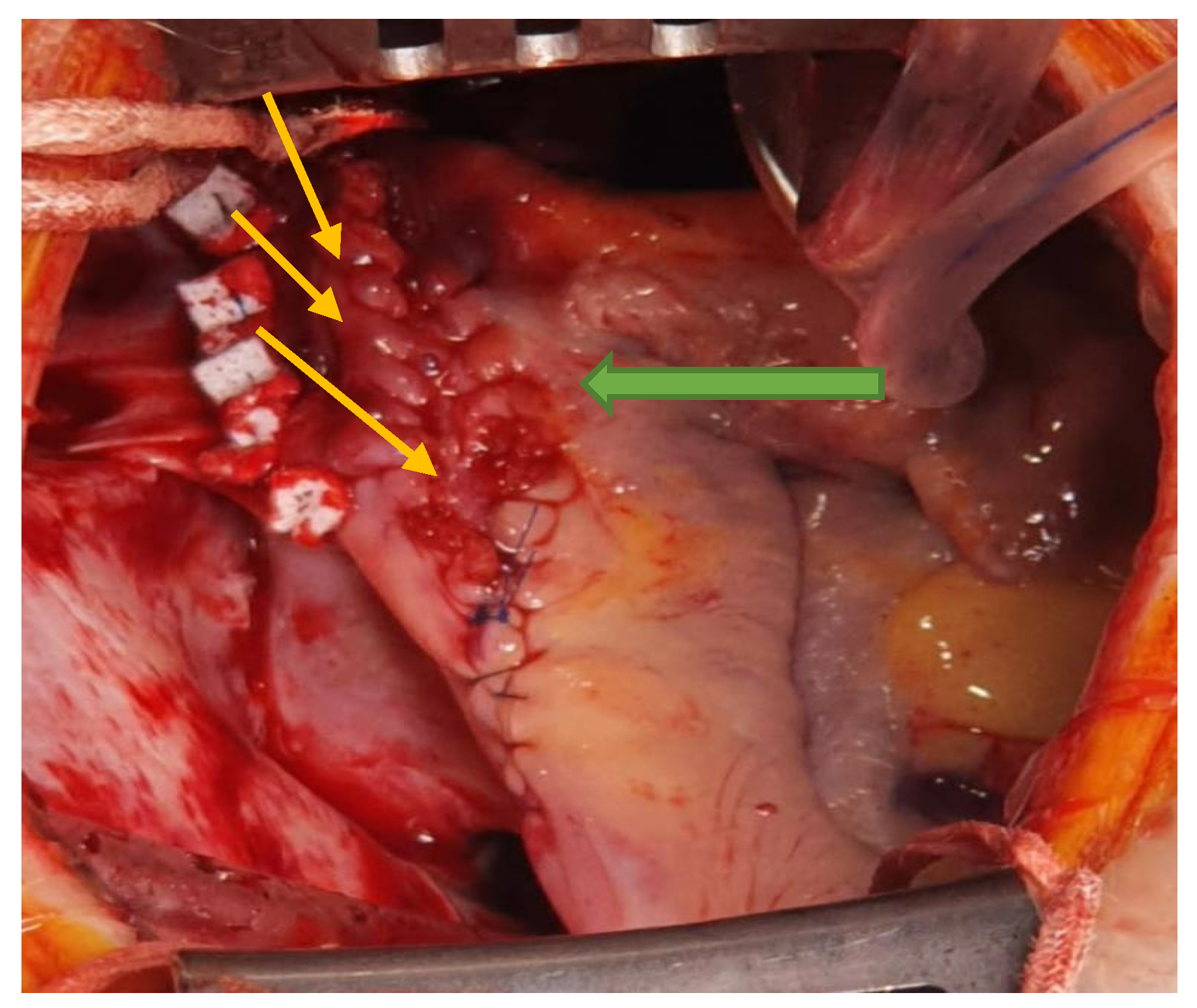
A fresh autologous pericardial patch (
Figure 5) was sutured in with a fine monofilament suture to close the ASD and to redirect the pulmonary venous flow towards the left atrium.
In order to prevent the SVC narrowing, a right atrial and SVC enlargement plasty was performed using a fresh autologous pericardial patch, reinforced with PTFE (Poly-Tetra-Fluoro-Ethylene) patches (
Figure 6).
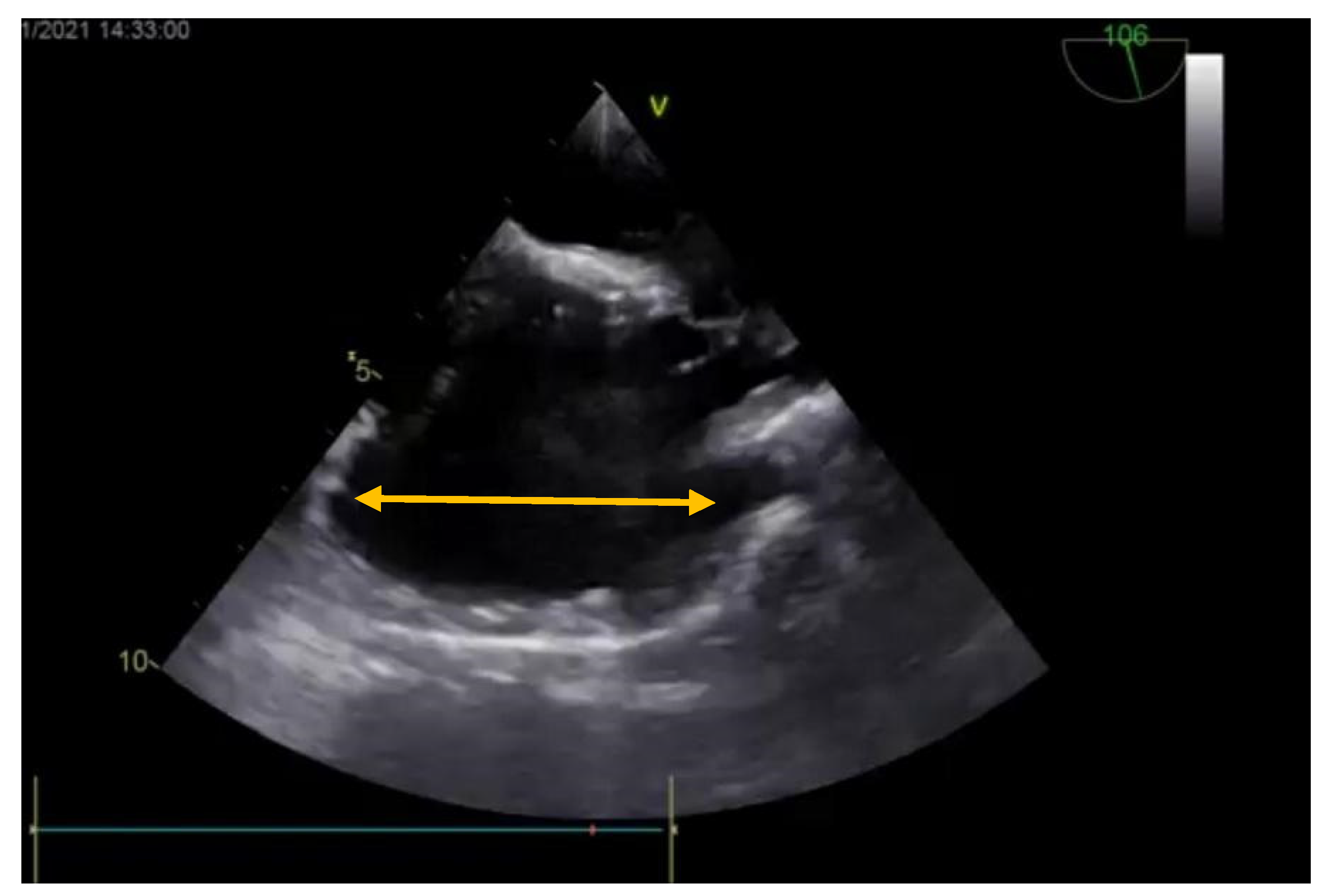
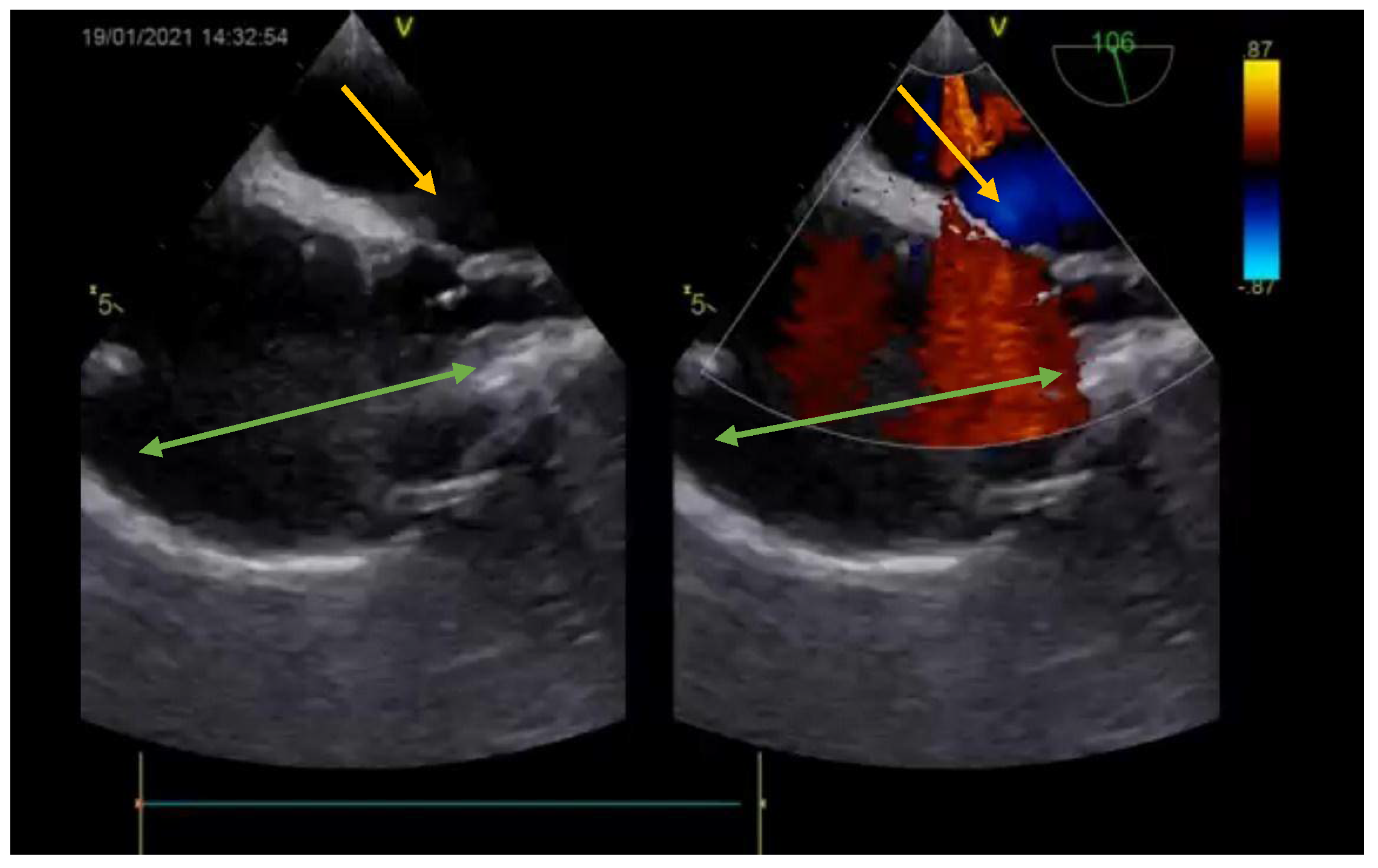
Postoperative transesophageal echocardiography (
Figure 7 and
Figure 8) showed the right heart cavities with no dilation and a minimum degree of tricuspid valve functional regurgitation. The inferior vena cava had a 19 mm diameter, and no residual shunts. Also, there was a small accumulation of fluid in the pericardium. The first ECG showed a normal sinus rhythm with 75 bpm, QRS axis at +120 degrees, minor right bundle-branch block with negative T waves in V1, V2. The patient later developed an accelerated junctional rhythm with 50 bpm and narrowed QRS complex, as is characteristic for a minor right bundle-branch block. The pulmonary artery pressure (measured during echocardiography) was normal.
The patient was extubated 5 h after surgery, with a minimum pneumopericardium, and, after removing the drainage tubes, developed a pneumothorax that required percutaneous insertion of a tube in the pleural space. After the remission of the pneumothorax, the tube was removed. The patient made a good recovery and was discharged on the 7th postoperative day. Medical treatment was recommended with bosentan and aspirin.
3. Discussion
Surgical techniques for ASD repair have developed since the beginning of cardiac surgery, in the late 1940s. Regarding the SV-ASDs with PAPVD, the main techniques that have been historically established are the two-patch technique (or baffle technique) and the Warden procedure, depending on the pulmonary drainage position [
14]. Each has its own advantages and risks; the Warden technique avoids the risk of sinus node dysfunction and cavoatrial incision, whereas the two-patch technique does not carry the risk of SVC obstruction—a rare but serious possible complication with these types of repair [
15]. In our clinic the minimal invasive approach is the preferred method for treating ASDs, as well as mitral and tricuspid valve surgeries. These cases have always evolved properly and there have been no conversions to the classic approach (median sternotomy).
The newest aspect of surgical ASD repair is robotic technology. Avoiding the thoracotomy incisions and the spreading of the ribs, this approach is said to reduce the pain caused by intercostal nerve damage, reduce postoperative recovery time, and to give greater overall patient satisfaction, as well as better cosmetic results, though it certainly has its limitations. First of all, the technique is challenging and time-consuming, with cardio-pulmonary bypass and aortic cross-clamping times that have been noted to be almost double what they are in the port-access approach. Secondly, when discussing robotic surgery, costs are still a significant barrier, and the duration of the hospital stay of patients has not been significantly reduced compared to the mini-thoracotomy approach. In addition to the above, the absence of tactile feedback as a consequence of using robotic assistance could make a simple suture a technically difficult surgical procedure, which might increase the risk of ASD recurrence.
Representing a complex subset of ASDs, SV-ASDs with PAPVD have traditionally been repaired surgically through a median sternotomy incision [
16]. A minimally invasive surgical approach via anterolateral right mini-thoracotomy has been associated with less blood loss, a shorter hospitalization period, faster recovery, improved healing, and better cosmetic results [
17]. Furthermore, having this type of incision leaves open the possibility for future median sternotomy with fewer adhesions, given the fact that the dissection and tissue trauma are limited [
18].
Patients with SV-ASD demonstrate unique anatomical and surgical features, and are at risk from postoperative complications [
19]. Postoperative sinus node dysfunction is common in patients after SV-ASD repair, potential mechanisms including an anatomic anomaly of the sinus node, intrinsic sinus node dysfunction, or surgical trauma caused by the proximity of the SV-ASD to the sinus node, the internodal tracts and the blood supply for the sinus node. A very significant complication that has been noted with the port-access approach is damage to the phrenic nerve, which could be avoided by carefully establishing the path of the phrenic nerve and opening the pericardium 2 cm away from it. Topical cooling would also have to be avoided [
20].
In the past three decades, mortality from congenital heart disease has decreased. In general this has been due to various improvements in medical and surgical management, and to technological upgrades in extracorporeal circulation [
21]. Regarding imaging techniques, it is recommended to perform transesophageal echocardiography (TEE), not only pre-operatively for diagnostic purposes, but also intraoperatively, due to its ability to help establish the operative plan and to assess the hemodynamic parameters during cardiac de-airing [
22]. It was believed that, despite the complexity of the lesion, repair of SV-ASD with PAPVD is associated with low morbidity and mortality even in patients older than 40 years [
23]. Furthermore, recent studies have concluded that delaying repair until the third decade of life is frequently associated with a decrease in life expectancy [
24]. This case report aims to demonstrate that in experienced centers, patients with isolated complex ASD lesions, such as an SV-ASD with PAPVD, can be repaired using a minimally invasive surgical approach.
4. Conclusions
To conclude, surgical repair of the SV-ASD involves well-known techniques which have proven to be effective. In the superior type of SV-ASD with PAPVD, which is either in the proximity of the cavoatrial junction or on it, the preferred method of treatment involves creating a pulmonary baffle and making a pericardial patch enlargement of the right atrium and SVC, whereas a distal placement of the pulmonary drainage or an inferior type of SV-ASD would benefit more from the Warden technique. In this case, the SV-ASD was closed and the PAPVD redirected to the left atrium with an SVC and right atrium baffle. Intraoperative transesophageal echocardiography confirmed the desired surgical result. Furthermore, the minimally invasive approach has shown itself to be a valid option, improving cosmetic results, as well as recovery time.
Author Contributions
Conceptualization, H.M., O.Z. and A.M.; methodology, H.M., G.V., D.G. and V.S.C.; software, R.Ț., D.G. and A.-M.S.; validation, H.M., V.S.C. and A.M.; formal analysis, A.-M.S., D.G. and O.Z.; investigation, H.M., A.-M.S., R.Ț., A.M., A.G. and B.-Ș.P.; resources, A.-M.S., R.Ț. and A.G.; data curation G.V., D.G., O.Z. and A.G.; writing—original draft preparation, A.-M.S., R.Ț., B.-Ș.P., G.V. and A.G.; writing—review and editing, H.M., D.G., O.Z. and A.M.; visualization, H.M., A.-M.S., R.Ț., B.-Ș.P., G.V., D.G., O.Z., V.S.C., A.G. and A.M.; supervision, H.M., O.Z., V.S.C. and A.M.; project administration, H.M. and A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Clinical Emergency Hospital of Bucharest (protocol code 647 and date of approval: 6 July 2021).
Informed Consent Statement
Informed consent was obtained from the patient involved in the study.
Data Availability Statement
The study did not report any data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Suchoń, E.; Podolec, P.; Tracz, W.; Przewłocki, T.; Wilkołek, P.; Kabłak-Ziembicka, A. Atrial septal defect in adults--opinions, procedures and controversies. Prz. Lek. 2001, 58, 131–135. (In Polish) [Google Scholar]
- Theodoropoulos, K.C.; Papachristidis, A.; Masoero, G.; Papitsas, M.; Cospite, V.; Demir, F.A.; Sado, D.M.; Monaghan, M.J. Superior sinus venosus atrial septal defect. J. Geriatr. Cardiol. 2018, 15, 649–652. [Google Scholar] [PubMed]
- Vodusek, Z.; Khaliqdina, S.; Borz-Baba, C.; Scandrett, R. Sinus Venosus Atrial Septal Defect: A Challenging Diagnosis. Cureus 2019, 11, e5936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobritoiu, F.; Moldovan, H.; Oncica, R.; Vasile, G.; Nechifor, E.; Copaescu, C. Giant Cavernous Hemangioma of the Right Atrium—A Rare Case and Literature Review. Chirurgia 2020, 115, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Matthew, L.; Kalfa, D. Surgical closure of atrial septal defects. J. Thorac. Dis. 2018, 10 (Suppl. 24), S2931–S2939. [Google Scholar]
- Webb, G.; Gatzoulis, M.A. Atrial Septal Defects in the Adult: Recent Progress and Overview. Circulation 2006, 114, 1645–1653. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.R.; Perry, J.C. Arrhythmias and conduction disorders associated with atrial septal defects. J. Thorac. Dis. 2018, 10 (Suppl. 24), S2940–S2944. [Google Scholar] [CrossRef]
- Moldovan, H.; Popescu, D.; Buliga, T.; Filip, A.; Antoniac, I.; Gheorghita, D.; Molnar, A. Gastric adenocarcinoma associated with acute endocarditis of the aortic valve and coronary artery disease in a 61-year-old male with multiple comorbidities-combined surgical management-case report. Medicina 2019, 55, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurcut, R.; Savu, O.; Popescu, B.A.; Florian, A.; Herlea, V.; Moldovan, H.; Ginghina, C. Primary Cardiac Leiomyosarcoma When Valvular Disease Becomes a Vascular Surgical Emergency. Circulation 2010, 121, E415–E418. [Google Scholar] [CrossRef] [Green Version]
- Gajjar, T.P.; Hiremath, C.S.; Desai, N.B. Surgical Closure of Sinus Venosus Atrial Septal Defect Using a Single Patch-Transcaval Repair Technique. J. Card. Surg. 2011, 26, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Kessel-Schaefer, A.; Linka, A.; Pretre, R.; Buser, P. Inferior sinus venosus defect associated with incomplete cor triatriatum dexter and patent foramen ovale. Eur. J. Echocardiogr. 2006, 7, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Vella, S.; Reichmuth, L.; Eynaud, S.M.; Manche, A. Superior sinus venosus atrial septal defect with anomalous pulmonary venous drainage. BMJ Case Rep. 2018, 11, e225596. [Google Scholar] [CrossRef]
- Baumgartner, H.; Bonhoeffer, P.; De Groot, N.M.F.; de Haan, F.; Deanfield, J.E.; Galie, N.; Gatzoulis, M.A.; Gohlke-Baerwolf, C.; Kaemmerer, H.; Kilner, P.; et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010): The Task Force on the Management of Grown-up Congenital Heart Disease of the European Society of Cardiology (ESC). Eur. Heart J. 2010, 31, 2915–2957. [Google Scholar] [PubMed] [Green Version]
- Vladimir, V.; Alexi-Meskishvili, M.D.; Igor, E.; Konstantinov, M.D. Surgical heritage Alexi-Meskishvili and Konstantinov- History of atrial septal defect surgery. Ann. Thorac. Surg. 2003, 76, 322–327. [Google Scholar]
- Mohite, P.N.; Rana, S.S.; Singh, J.; Kotkar, K.D.; Puri, G.D.; Sodhi, S.K. Acute superior vena cava obstruction due to tight pericardial closure following congenital defect repair. J. Cardiovasc. Dis. Res. 2012, 3, 135–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozso, S.J.; Evans, B.; Chu, M.W.A. Minimally invasive periareoral approach to repair sinus venosus atrial septal defect with partial anomalous pulmonary venous connection. J. Card. Surg. 2020, 35, 1653–1656. [Google Scholar] [CrossRef]
- Guariento, A.; Cattapan, C.; Bertelli, F.; Vida, V. Minimally invasive congenital cardiac surgery with unsnared inferior vena cava. Authorea 2020. [Google Scholar] [CrossRef]
- Chen, C.A.; Wang, J.K.; Hsu, J.Y.; Hsu, H.H.; Chen, S.J.; Wu, M.H. Diagnosis of inferior sinus venosus atrial septal defects using transthoracic three-dimensional echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, e4–e6. [Google Scholar] [CrossRef]
- Sojak, V.; Sagat, M.; Balazova, E.; Siman, J. Outcomes after surgical repair of sinus venosus atrial septal defect in children. Bratisl. Lek. Listy 2008, 109, 215–219. [Google Scholar]
- Jost, C.H.A.; Connolly, H.M.; Danielson, G.K.; Bailey, K.R.; Schaff, H.V.; Shen, W.K.; Warnes, C.A.; Seward, J.B.; Puga, F.J.; Tajik, A.J. Patterns of Anomalous pulmonary Venous Connection as Seen at Care Hospital, Hyderabad–India. East Cent. Afr. J. Surg. 2007, 12, 18–22. [Google Scholar]
- Chira, M.; Ciotlaus, D.F.; Tinica, G.; Manole, S.; Sacui, D.M.; Molnar, A. Early Repair Benefits in Cognitive Development of Patients with Tetralogy of Fallot. Rev. Cercet. Interv. Soc. 2017, 57, 78–88. [Google Scholar]
- Molnar, A.; Sacui, D.; Manole, S.; Radulescu, A.; Beyer, R. The value of transthoracic and transesophageal echocardiography for the diagnosis of the native aortic infective endocarditis valve complications: A case report and literature review. Med. Ultrason. 2016, 18, 253–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jost, C.H.A.; Connolly, H.M.; Danielson, G.K.; Bailey, K.R.; Schaff, H.V.; Shen, W.K.; Warnes, C.A.; Seward, J.B.; Puga, F.J.; Tajik, A.J. Sinus venosus atrial septal defect: Long-term postoperative outcome for 115 patients. Circulation 2005, 112, 1953–1958. [Google Scholar] [CrossRef]
- Vistarini, N.; Aiello, M.; Mattiucci, G.; Alloni, A.; Cattadori, B.; Tinelli, C.; Pellegrini, C.; D’Armini, A.M.; Viganò, M. Port-access minimally invasive surgery for atrial septal defects: A 10-year single-center experience in 166 patients. J. Thorac. Cardiovasc. Surg. 2010, 139, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







