
Olfactory and Gustatory Function before and after Laparoscopic Sleeve Gastrectomy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
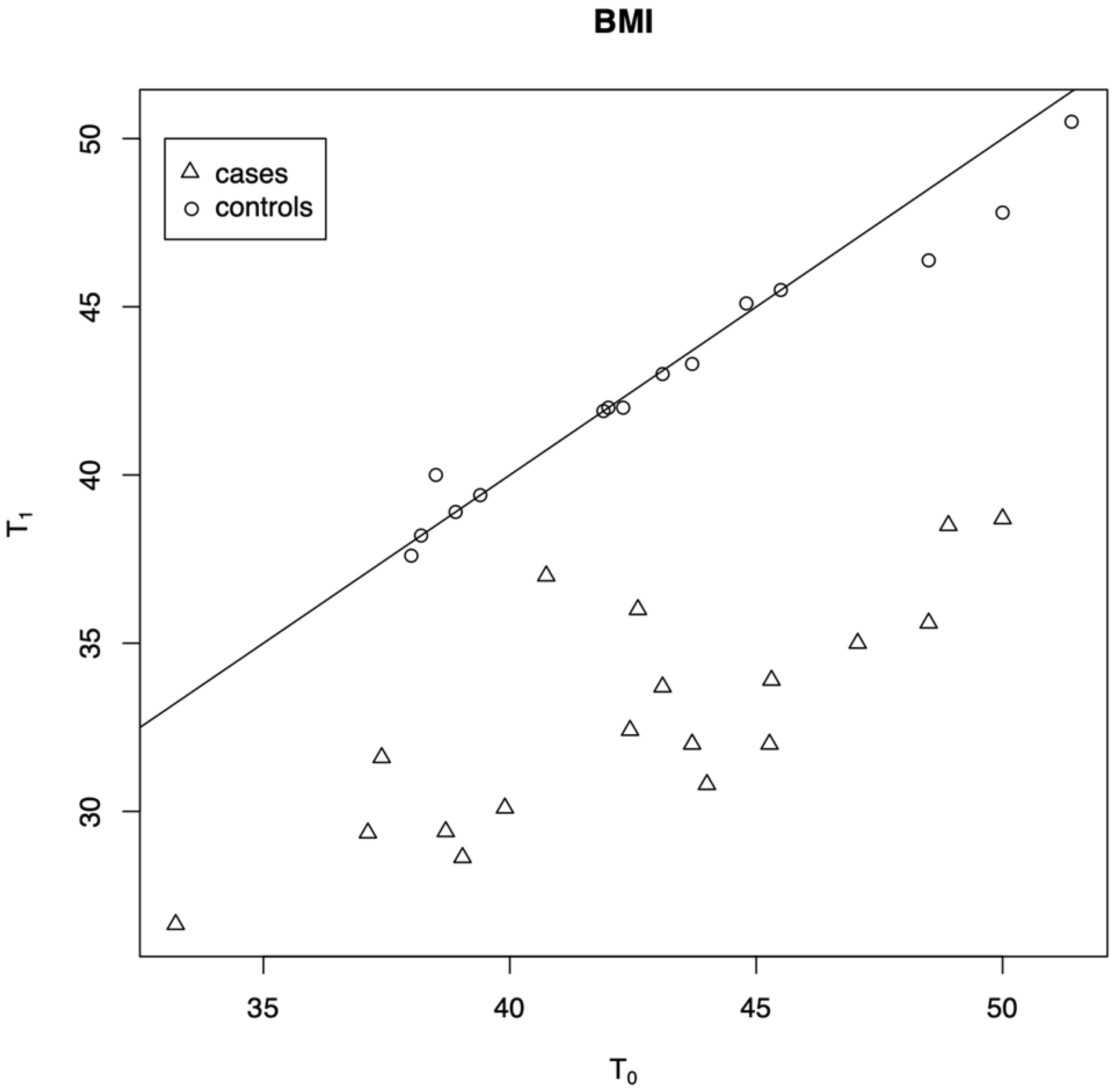
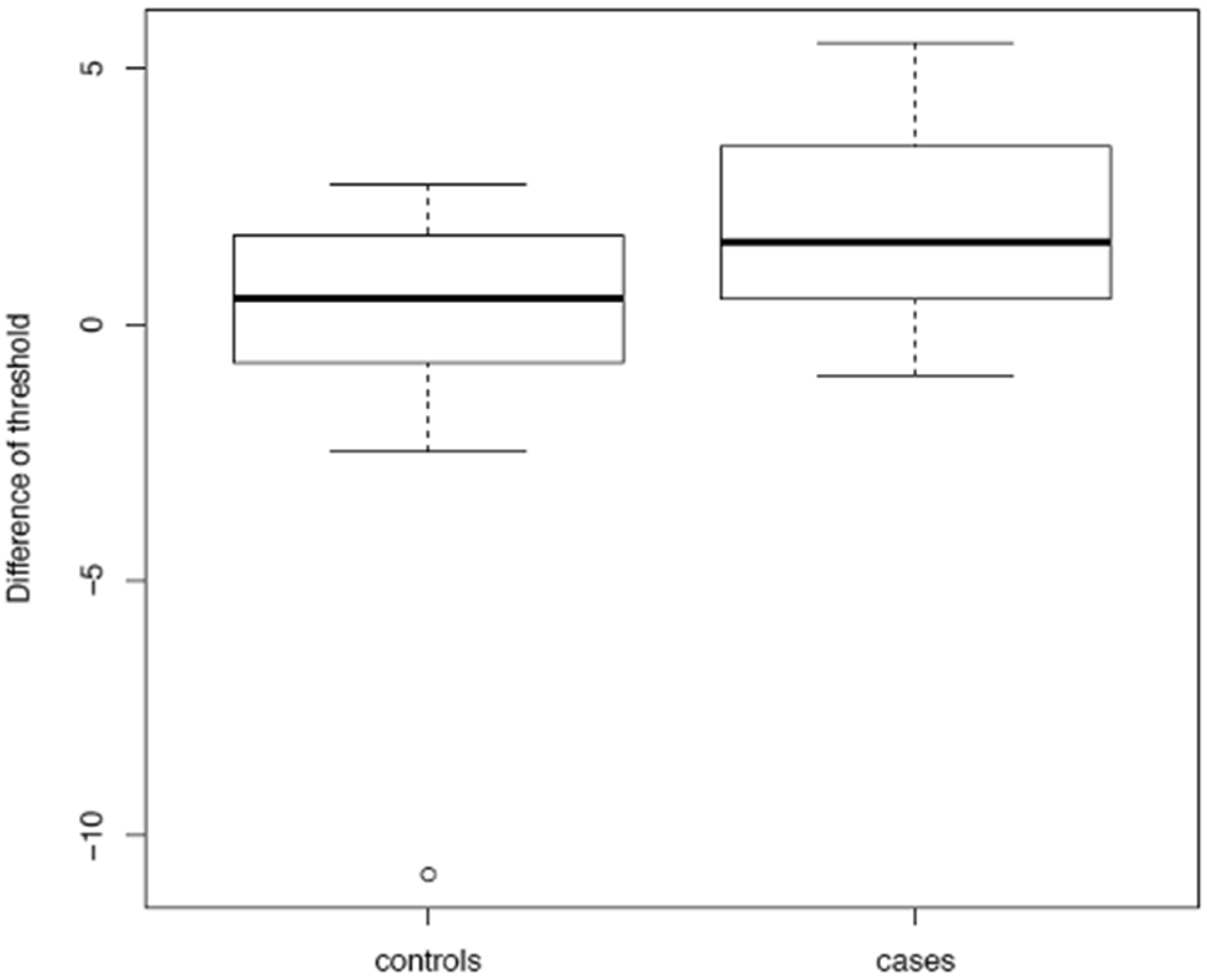
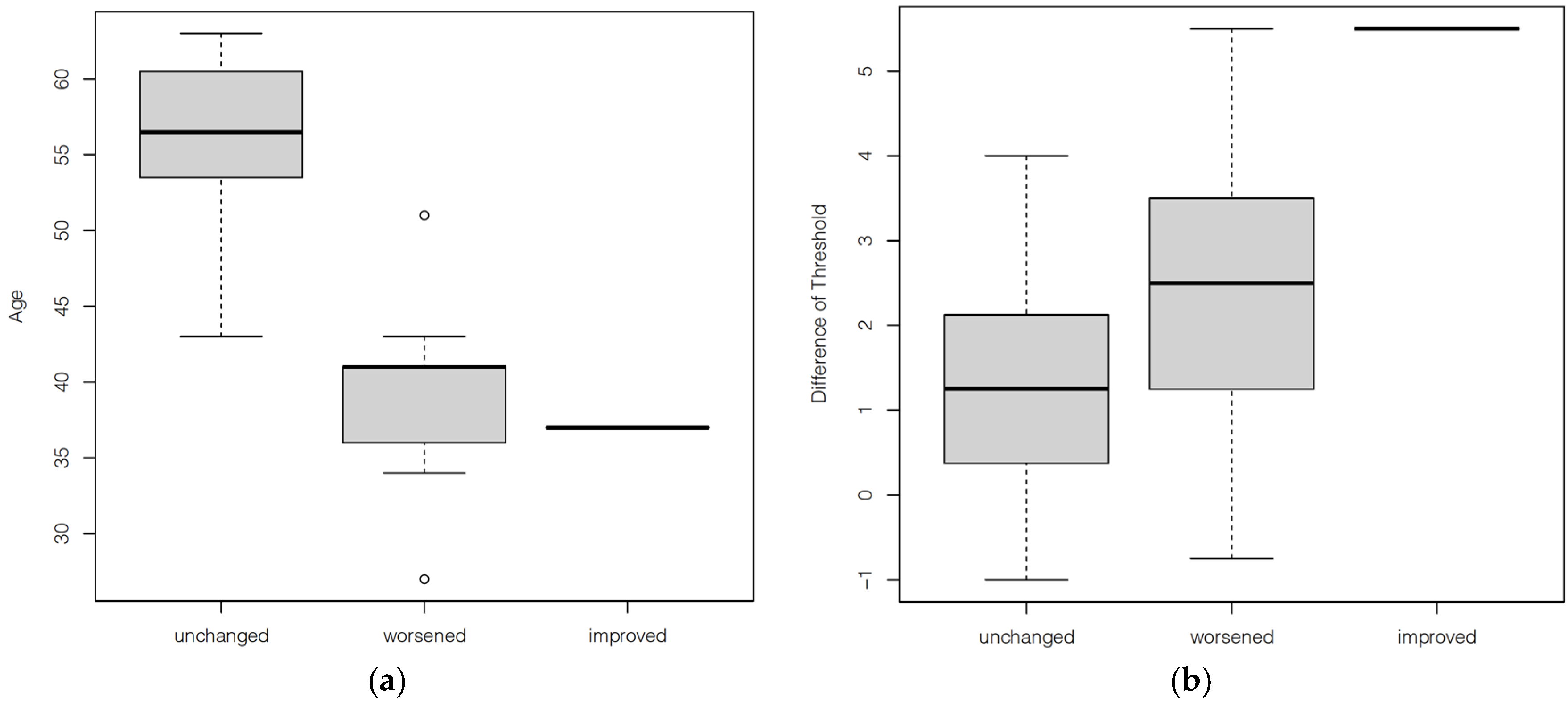
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jurowich, C.; Germer, C.T.; Seyfried, F.; Thalheimer, A. [Metabolic surgery]. Chirurg 2012, 83, 583–600. [Google Scholar] [CrossRef]
- Sjostrom, L. Review of the key results from the Swedish Obese Subjects (SOS) trial—A prospective controlled intervention study of bariatric surgery. J. Intern. Med. 2013, 273, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Hubert, P.A.; Papasavas, P.; Stone, A.; Swede, H.; Huedo-Medina, T.B.; Tishler, D.; Duffy, V.B. Associations between Weight Loss, Food Likes, Dietary Behaviors, and Chemosensory Function in Bariatric Surgery: A Case-Control Analysis in Women. Nutrients 2019, 11, 804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadross, J.A.; le Roux, C.W. The mechanisms of weight loss after bariatric surgery. Int. J. Obes. 2009, 33, S28–S32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brolin, R.E.; LaMarca, L.B.; Kenler, H.A.; Cody, R.P. Malabsorptive gastric bypass in patients with superobesity. J. Gastrointest. Surg. 2002, 6, 195–205. [Google Scholar] [CrossRef]
- Zerrweck, C.; Gallardo, V.C.; Calleja, C.; Sepulveda, E.; Guilber, L. Gross Olfaction Before and After Laparoscopic Gastric Bypass. Obes. Surg. 2017, 27, 2988–2992. [Google Scholar] [CrossRef]
- Holinski, F.; Menenakos, C.; Haber, G.; Olze, H.; Ordemann, J. Olfactory and Gustatory Function After Bariatric Surgery. Obes. Surg. 2015, 25, 2314–2320. [Google Scholar] [CrossRef]
- Hanci, D.; Altun, H.; Altun, H.; Batman, B.; Karip, A.B.; Serin, K.R. Laparoscopic Sleeve Gastrectomy Improves Olfaction Sensitivity in Morbidly Obese Patients. Obes. Surg. 2016, 26, 558–562. [Google Scholar] [CrossRef]
- Zerrweck, C.; Zurita, L.; Alvarez, G.; Maydon, H.G.; Sepulveda, E.M.; Campos, F.; Caviedes, A.; Guilbert, L. Taste and Olfactory Changes Following Laparoscopic Gastric Bypass and Sleeve Gastrectomy. Obes. Surg. 2016, 26, 1296–1302. [Google Scholar] [CrossRef]
- Gopinath, B.; Russell, J.; Sue, C.M.; Flood, V.M.; Burlutsky, G.; Mitchell, P. Olfactory impairment in older adults is associated with poorer diet quality over 5 years. Eur. J. Nutr. 2016, 55, 1081–1087. [Google Scholar] [CrossRef]
- Nordin, S.; Bramerson, A. Complaints of olfactory disorders: Epidemiology, assessment and clinical implications. Curr. Opin. Allergy Clin. Immunol. 2008, 8, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Stafford, L.D.; Welbeck, K. High hunger state increases olfactory sensitivity to neutral but not food odors. Chem. Senses 2011, 36, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Rimmer, J.; Hellings, P.; Lund, V.J.; Alobid, I.; Beale, T.; Dassi, C.; Douglas, R.; Hopkins, C.; Klimek, L.; Landis, B.; et al. European position paper on diagnostic tools in rhinology. Rhinology 2019, 57, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Iacono, V.; Lombardi, G.; Ottaviano, G.; Gambaro, G.; Zaza, G. Impact of renal replacement therapies on olfactory ability: Results of a cross-sectional case control study. J. Nephrol. 2021, 1–10. [Google Scholar] [CrossRef]
- Schopf, V.; Kollndorfer, K.; Pollak, M.; Mueller, C.A.; Freiherr, J. Intranasal insulin influences the olfactory performance of patients with smell loss, dependent on the body mass index: A pilot study. Rhinology 2015, 53, 371–378. [Google Scholar] [CrossRef]
- Ottaviano, G.; Savietto, E.; Scarpa, B.; Bertocco, A.; Maculan, P.; Sergi, G.; Martini, A.; Manzato, E.; Marioni, G. Influence of number of drugs on olfaction in the elderly. Rhinology 2018, 56, 351–357. [Google Scholar] [CrossRef]
- Cecchini, M.P.; Osculati, F.; Ottaviani, S.; Boschi, F.; Fasano, A.; Tinazzi, M. Taste performance in Parkinson’s disease. J. Neural. Transm. 2014, 121, 119–122. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position paper on olfactory dysfunction. Rhinology 2016, 56, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Cantone, E.; Ciofalo, A.; Vodicka, J.; Iacono, V.; Mylonakis, I.; Scarpa, B.; Russo, M.; Iengo, M.; de Vincentiis, M.; Martini, A.; et al. Pleasantness of olfactory and trigeminal stimulants in different Italian regions. Eur. Arch. Otorhinolaryngol. 2017, 274, 3907–3913. [Google Scholar] [CrossRef] [PubMed]
- Richardson, B.E.; Vanderwoude, E.A.; Sudan, R.; Leopold, D.A.; Thompson, J.S. Gastric bypass does not influence olfactory function in obese patients. Obes. Surg. 2012, 22, 283–286. [Google Scholar] [CrossRef]
- Melis, M.; Pintus, S.; Mastinu, M.; Fantola, G.; Moroni, R.; Pepino, M.Y.; Barbarossa, I.T. Changes of Taste, Smell and Eating Behavior in Patients Undergoing Bariatric Surgery: Associations with PROP Phenotypes and Polymorphisms in the Odorant-Binding Protein OBPIIa and CD36 Receptor Genes. Nutrients 2021, 13, 250. [Google Scholar] [CrossRef] [PubMed]
- Pisarska-Adamczyk, M.; Tylec, P.; Gajewska, N.; Wierzbicka, J.; Przeczek, K.; Malczak, P.; Wysocki, M.; Pedziwiatr, M.; Wierdak, M.; Major, P. Postoperative Olfaction Alteration Following Laparoscopic Bariatric Surgery. J. Clin. Med. 2021, 10, 1704. [Google Scholar] [CrossRef]
- Jurowich, C.F.; Seyfried, F.; Miras, A.D.; Bueter, M.; Deckelmann, J.; Fassnacht, M.; Germer, C.T.; Thalheimer, A. Does bariatric surgery change olfactory perception? Results of the early postoperative course. Int. J. Colorectal. Dis. 2014, 29, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Ottaviano, G.; Zuccarello, D.; Frasson, G.; Scarpa, B.; Nardello, E.; Foresta, C.; Marioni, G.; Staffieri, A. Olfactory sensitivity and sexual desire in young adult and elderly men: An introductory investigation. Am. J. Rhinol. Allergy 2013, 27, 157–161. [Google Scholar] [CrossRef]
- Ottaviano, G.; Frasson, G.; Nardello, E.; Martini, A. Olfaction deterioration in cognitive disorders in the elderly. Aging Clin. Exp. Res. 2016, 28, 37–45. [Google Scholar] [CrossRef]
- Ottaviano, G.; Cantone, E.; D’Errico, A.; Salvalaggio, A.; Citton, V.; Scarpa, B.; Favaro, A.; Sinisi, A.A.; Liuzzi, R.; Bonanni, G.; et al. Sniffin’ Sticks and olfactory system imaging in patients with Kallmann syndrome. Int. Forum Allergy Rhinol. 2015, 5, 855–861. [Google Scholar] [CrossRef]
- Ahmed, K.; Penney, N.; Darzi, A.; Purkayastha, S. Taste Changes after Bariatric Surgery: A Systematic Review. Obes. Surg. 2018, 28, 3321–3332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.L.; Yang, Q.; Hajnal, A.; Rogers, A.M. A pilot functional MRI study in Roux-en-Y gastric bypass patients to study alteration in taste functions after surgery. Surg. Endosc. 2016, 30, 892–898. [Google Scholar] [CrossRef]
- Altun, H.; Hanci, D.; Altun, H.; Batman, B.; Serin, R.K.; Karip, A.B.; Akyuz, U. Improved Gustatory Sensitivity in Morbidly Obese Patients After Laparoscopic Sleeve Gastrectomy. Ann. Otol. Rhinol. Laryngol. 2016, 125, 536–540. [Google Scholar] [CrossRef]
- Scruggs, D.M.; Buffington, C.; Cowan, G.S., Jr. Taste Acuity of the Morbidly Obese before and after Gastric Bypass Surgery. Obes. Surg. 1994, 4, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Tichansky, D.S.; Boughter, J.D., Jr.; Madan, A.K. Taste change after laparoscopic Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding. Surg. Obes. Relat. Dis. 2006, 2, 440–444. [Google Scholar] [CrossRef]
- Thiebaud, N.; Johnson, M.C.; Butler, J.L.; Bell, G.A.; Ferguson, K.L.; Fadool, A.R.; Fadool, J.C.; Gale, A.M.; Gale, D.S.; Fadool, D.A. Hyperlipidemic diet causes loss of olfactory sensory neurons, reduces olfactory discrimination, and disrupts odor-reversal learning. J. Neurosci. 2014, 34, 6970–6984. [Google Scholar] [CrossRef] [Green Version]
- Uygun, B.; Kiyici, S.; Ozmen, S.; Gul, Z.; Sigirli, D.; Cavun, S. The Association Between Olfaction and Taste Functions with Serum Ghrelin and Leptin Levels in Obese Women. Metab. Syndr. Relat. Disord. 2019, 17, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Gerspach, A.C.; Steinert, R.E.; Schonenberger, L.; Graber-Maier, A.; Beglinger, C. The role of the gut sweet taste receptor in regulating GLP-1, PYY, and CCK release in humans. Am. J. Physiol. Endocrinol. Metab. 2011, 301, E317–E325. [Google Scholar] [CrossRef]
- Shin, Y.K.; Martin, B.; Golden, E.; Dotson, C.D.; Maudsley, S.; Kim, W.; Jang, H.J.; Mattson, M.P.; Drucker, D.J.; Egan, J.M.; et al. Modulation of taste sensitivity by GLP-1 signaling. J. Neurochem. 2008, 106, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Peterli, R.; Steinert, R.E.; Woelnerhanssen, B.; Peters, T.; Christoffel-Courtin, C.; Gass, M.; Kern, B.; von Fluee, M.; Beglinger, C. Metabolic and hormonal changes after laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy: A randomized, prospective trial. Obes. Surg. 2012, 22, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Ramon, J.M.; Salvans, S.; Crous, X.; Puig, S.; Goday, A.; Benaiges, D.; Trillo, L.; Pera, M.; Grande, L. Effect of Roux-en-Y gastric bypass vs sleeve gastrectomy on glucose and gut hormones: A prospective randomised trial. J. Gastrointest. Surg. 2012, 16, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Dotson, C.D.; Geraedts, M.C.; Munger, S.D. Peptide regulators of peripheral taste function. Semin Cell Dev. Biol. 2013, 24, 232–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, A.M.; Griffin, S.M. Postoperative taste and smell deficit after upper gastrointestinal cancer surgery—An unreported complication. J. Surg. Oncol. 2003, 82, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Althuwaini, S.; Bamehriz, F.; Aldohayan, A.; Alshammari, W.; Alhaidar, S.; Alotaibi, M.; Alanazi, A.; Alsahabi, H.; Almadi, M.A. Prevalence and Predictors of Gastroesophageal Reflux Disease After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2018, 28, 916–922. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Treatment Group (n = 18) | T0 | T1 | ||||
| Mean | SD | Range | Mean | SD | Range | |
| Age (year) | 46.4 | 10.6 | 27–63 | - | - | - |
| BMI (Kg/m2) | 42.6 | 4.5 | 32.2–50 | 32.9 | 3.5 | 26.6–38.7 |
| Identification | 12.4 | 1.5 | 10–15 | 12.1 | 1.4 | 10–14 |
| Threshold | 7.3 | 1.6 | 4.25–10.25 | 9.3 | 2.2 | 4.75–12.75 |
| Discrimination | 12.3 | 1.3 | 10–15 | 12.3 | 1.7 | 8–16 |
| TDI | 32 | 2.6 | 27.25–36.5 | 33.8 | 3.1 | 27.75–38.75 |
| Taste identification | 3.9 | 0.3 | 3–4 | 3.8 | 0.4 | 3–4 |
| MMSE | 29 | 0.78 | 28–30 | - | - | - |
| VAS smell | 0.06 | 0.24 | 0–1 | 0.06 | 0.24 | 0–1 |
| VAS taste | 0 | 0 | 0 | 0 | ||
| Control Group (n = 16) | T0 | T1 | ||||
| Mean | SD | Range | Mean | SD | Range | |
| Age (year) | 48.9 | 11.6 | 21–67 | - | - | - |
| BMI (Kg/m2) | 43.1 | 4.3 | 38–51.4 | 42.8 | 3.7 | 37.6–50.5 |
| Identification | 12.6 | 1.1 | 11–14 | 12.9 | 1.3 | 10–15 |
| Threshold | 8.6 | 2.4 | 7–15.25 | 8.4 | 2.5 | 4.5–14 |
| Discrimination | 11.7 | 1.4 | 9–14 | 12.2 | 1.4 | 10–15 |
| TDI | 32.9 | 2.7 | 31–40.25 | 33.5 | 2.4 | 32.5–40.75 |
| Taste identification | 3.9 | 0.26 | 3–4 | 3.9 | 0.26 | 3–4 |
| MMSE | 29 | 1 | 27–30 | - | - | - |
| VAS smell | 0 | 0 | 0 | 0 | ||
| VAS taste | 0 | 0 | 0 | 0 | ||
| Coefficients | Estimate | Std. Error | T Value | Pr (>|t|) |
|---|---|---|---|---|
| (Intercept) | 7.5148 | 14.5831 | 0.515 | 0.6109 |
| Cases | −4.2924 | 2.5770 | −1.666 | 0.1083 |
| MMSE | 1.0540 | 0.4547 | 2.318 | 0.0289 * |
| BMI T0 | −0.1966 | 0.1172 | −1.677 | 0.1061 |
| Δ BMI | −0.4027 | 0.2399 | −1.678 | 0.1057 |
| Olfactory threshold T0 | −0.4377 | 0.2943 | −1.487 | 0.1495 |
| TDI T0 | −0.2902 | 0.2304 | −1.260 | 0.2195 |
| Taste identification T0 | −3.8598 | 1.4202 | −2.718 | 0.0118 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berro, C.; Pendolino, A.L.; Foletto, M.; Facciolo, M.C.; Maculan, P.; Prevedello, L.; Giuntoli, D.G.; Scarpa, B.; Pavan, C.; Andrews, P.J.; et al. Olfactory and Gustatory Function before and after Laparoscopic Sleeve Gastrectomy. Medicina 2021, 57, 913. https://doi.org/10.3390/medicina57090913
Berro C, Pendolino AL, Foletto M, Facciolo MC, Maculan P, Prevedello L, Giuntoli DG, Scarpa B, Pavan C, Andrews PJ, et al. Olfactory and Gustatory Function before and after Laparoscopic Sleeve Gastrectomy. Medicina. 2021; 57(9):913. https://doi.org/10.3390/medicina57090913
Chicago/Turabian StyleBerro, Cecilia, Alfonso Luca Pendolino, Mirto Foletto, Maria Cristina Facciolo, Pietro Maculan, Luca Prevedello, Diletta Giulia Giuntoli, Bruno Scarpa, Chiara Pavan, Peter J. Andrews, and et al. 2021. "Olfactory and Gustatory Function before and after Laparoscopic Sleeve Gastrectomy" Medicina 57, no. 9: 913. https://doi.org/10.3390/medicina57090913