
Neuroinflammation in Autism and Supplementation Based on Omega-3 Polyunsaturated Fatty Acids: A Narrative Review

 ,
,
Abstract
:1. Introduction
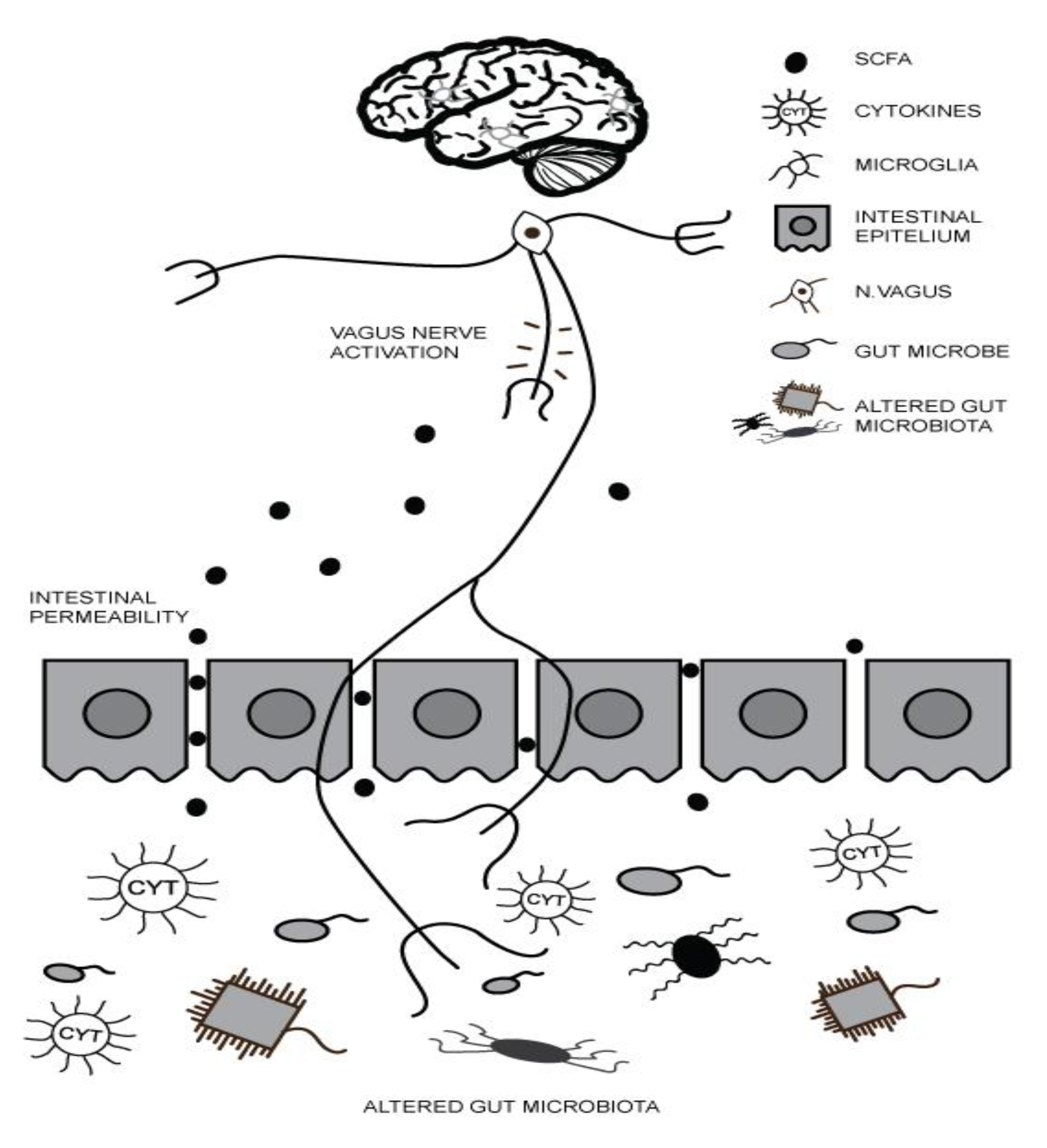
2. Gut–Brain Axis (GBA) and ASD
3. Maternal Inflammation during Pregnancy and ASD
4. Essential Fatty Acids—Omega-3 and Omega-6 PUFA and Inflammatory Processes in ASD
4.1. Omega-3 and Omega-6 PUFA and Gut Microbiota in ASD
4.2. Maternal Status of PUFA during Pregnancy and ASD
5. The Role of Omega-3 PUFA Supplementation in ASD Symptoms
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; New School Library: London, UK, 2013. [Google Scholar]
- Kohane, I.S.; McMurry, A.; Weber, G.; MacFadden, D.; Rappaport, L.; Kunkel, L.; Bickel, J.; Wattanasin, N.; Spence, S.; Murphy, S. The co-morbidity burden of children and young adults with autism spectrum disorders. PLoS ONE 2012, 7, e33224. [Google Scholar] [CrossRef] [PubMed]
- Kraneveld, A.; Szklany, K.; de Theije, C.; Garssen, J. Gut-to-brain axis in autism spectrum disorders: Central role for the microbiome. Int. Rev. Neurobiol. 2016, 131, 263–287. [Google Scholar] [PubMed]
- Gaugler, T.; Klei, L.; Sanders, S.J.; Bodea, C.A.; Goldberg, A.P.; Lee, A.B.; Mahajan, M.; Manaa, D.; Pawitan, Y.; Reichert, J. Most genetic risk for autism resides with common variation. Nat. Genet. 2014, 46, 881–885. [Google Scholar] [CrossRef] [Green Version]
- Carter, M.T.; Scherer, S.W. Autism spectrum disorder in the genetics clinic: A review. Clin. Genet. 2013, 83, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Castellani, M.; Conti, C.; Kempuraj, D.; Salini, V.; Vecchiet, J.; Tete, S.; Ciampoli, C.; Conti, F.; Cerulli, G.; Caraffa, A. Autism and immunity: Revisited study. Int. J. Immunopathol. Pharmacol. 2009, 22, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Rose, S.; Slattery, J.; MacFabe, D.F. Gastrointestinal dysfunction in autism spectrum disorder: The role of the mitochondria and the enteric microbiome. Microb. Ecol. health Dis. 2015, 26, 27458. [Google Scholar] [CrossRef] [PubMed]
- Vuong, H.E.; Hsiao, E.Y. Emerging roles for the gut microbiome in autism spectrum disorder. Biol. Psychiatry 2017, 81, 411–423. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Han, Y.; Dy, A.B.C.; Hagerman, R.J. The gut microbiota and autism spectrum disorders. Front. Cell. Neurosci. 2017, 11, 120. [Google Scholar] [CrossRef]
- Noriega, D.B.; Savelkoul, H.F. Immune dysregulation in autism spectrum disorder. Eur. J. Pediatrics 2014, 173, 33–43. [Google Scholar] [CrossRef]
- Ciéslińska, A.; Kostyra, E.; Savelkoul, H.F. Treating autism spectrum disorder with gluten-free and casein-free diet: The underlying microbiota-gut-brain axis mechanisms. HSOA J. Clin. Immunol. Immunother. 2017, 3, 11. [Google Scholar]
- Milošević, M.; Arsić, A.; Cvetković, Z.; Vučić, V. Memorable Food: Fighting Age-Related Neurodegeneration by Precision Nutrition. Front. Nutr. 2021, 8. [Google Scholar] [CrossRef]
- Li, Q.; Zhou, J.-M. The microbiota–gut–brain axis and its potential therapeutic role in autism spectrum disorder. Neuroscience 2016, 324, 131–139. [Google Scholar] [CrossRef]
- Iannone, L.F.; Preda, A.; Blottière, H.M.; Clarke, G.; Albani, D.; Belcastro, V.; Carotenuto, M.; Cattaneo, A.; Citraro, R.; Ferraris, C. Microbiota-gut brain axis involvement in neuropsychiatric disorders. Expert Rev. Neurother. 2019, 19, 1037–1050. [Google Scholar] [CrossRef]
- MacFabe, D.F. Enteric short-chain fatty acids: Microbial messengers of metabolism, mitochondria, and mind: Implications in autism spectrum disorders. Microb. Ecol. health Dis. 2015, 26, 28177. [Google Scholar] [CrossRef] [Green Version]
- Maslowski, K.M.; Vieira, A.T.; Ng, A.; Kranich, J.; Sierro, F.; Yu, D.; Schilter, H.C.; Rolph, M.S.; Mackay, F.; Artis, D. Regulation of inflammatory responses by gut microbiota and chemoattractant receptor GPR43. Nature 2009, 461, 1282–1286. [Google Scholar] [CrossRef] [PubMed]
- Goines, P.E.; Ashwood, P. Cytokine dysregulation in autism spectrum disorders (ASD): Possible role of the environment. Neurotoxicol. Teratol. 2013, 36, 67–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooks, M.G.; Garrett, W.S. Gut microbiota, metabolites and host immunity. Nat. Rev. Immunol. 2016, 16, 341–352. [Google Scholar] [CrossRef]
- Madore, C.; Leyrolle, Q.; Lacabanne, C.; Benmamar-Badel, A.; Joffre, C.; Nadjar, A.; Layé, S. Neuroinflammation in autism: Plausible role of maternal inflammation, dietary omega 3, and microbiota. Neural Plast. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, P.H. Maternal infection and immune involvement in autism. Trends Mol. Med. 2011, 17, 389–394. [Google Scholar] [CrossRef] [Green Version]
- van der Burg, J.W.; Sen, S.; Chomitz, V.R.; Seidell, J.C.; Leviton, A.; Dammann, O. The role of systemic inflammation linking maternal BMI to neurodevelopment in children. Pediatric Res. 2016, 79, 3–12. [Google Scholar] [CrossRef]
- Vargas, D.L.; Nascimbene, C.; Krishnan, C.; Zimmerman, A.W.; Pardo, C.A. Neuroglial activation and neuroinflammation in the brain of patients with autism. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 2005, 57, 67–81. [Google Scholar] [CrossRef]
- El-Ansary, A.; Al-Ayadhi, L. GABAergic/glutamatergic imbalance relative to excessive neuroinflammation in autism spectrum disorders. J. Neuroinflammation 2014, 11, 1–9. [Google Scholar] [CrossRef]
- Masi, A.; Quintana, D.; Glozier, N.; Lloyd, A.; Hickie, I.; Guastella, A. Cytokine aberrations in autism spectrum disorder: A systematic review and meta-analysis. Mol. Psychiatry 2015, 20, 440–446. [Google Scholar] [CrossRef]
- Ristic-Medic, D.; Vucic, V. Dietary fats and metabolic syndrome. J. Nutr. Health Food Sci. 2013, 1, 8. [Google Scholar]
- Parletta, N.; Niyonsenga, T.; Duff, J. Omega-3 and omega-6 polyunsaturated fatty acid levels and correlations with symptoms in children with attention deficit hyperactivity disorder, autistic spectrum disorder and typically developing controls. PLoS ONE 2016, 11, e0156432. [Google Scholar] [CrossRef]
- De Crescenzo, F.; D’Alò, G.L.; Morgano, G.P.; Minozzi, S.; Mitrova, Z.; Saulle, R.; Cruciani, F.; Fulceri, F.; Davoli, M.; Scattoni, M.L. Impact of polyunsaturated fatty acids on patient-important outcomes in children and adolescents with autism spectrum disorder: A systematic review. Health Qual. life Outcomes 2020, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Gesundheit, B.; Rosenzweig, J.P.; Naor, D.; Lerer, B.; Zachor, D.A.; Procházka, V.; Melamed, M.; Kristt, D.A.; Steinberg, A.; Shulman, C. Immunological and autoimmune considerations of Autism Spectrum Disorders. J. Autoimmun. 2013, 44, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pardo, C.A.; Eberhart, C.G. The neurobiology of autism. Brain Pathol. 2007, 17, 434–447. [Google Scholar] [CrossRef] [PubMed]
- Mazahery, H.; Stonehouse, W.; Delshad, M.; Kruger, M.C.; Conlon, C.A.; Beck, K.L.; Von Hurst, P.R. Relationship between long chain n-3 polyunsaturated fatty acids and autism spectrum disorder: Systematic review and meta-analysis of case-control and randomised controlled trials. Nutrients 2017, 9, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheppard, K.W.; Boone, K.M.; Gracious, B.; Klebanoff, M.A.; Rogers, L.K.; Rausch, J.; Bartlett, C.; Coury, D.L.; Keim, S.A. Effect of omega-3 and-6 supplementation on language in preterm toddlers exhibiting autism spectrum disorder symptoms. J. Autism Dev. Disord. 2017, 47, 3358–3369. [Google Scholar] [CrossRef] [PubMed]
- Won, H.; Mah, W.; Kim, E. Autism spectrum disorder causes, mechanisms, and treatments: Focus on neuronal synapses. Front. Mol. Neurosci. 2013, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Tas, A.A. Dietary strategies in autism spectrum disorder (ASD). Prog. Nutr. 2018, 20, 554–562. [Google Scholar]
- Mazahery, H.; Conlon, C.A.; Beck, K.L.; Mugridge, O.; Kruger, M.C.; Stonehouse, W.; Camargo, C.A., Jr.; Meyer, B.J.; Jones, B.; von Hurst, P.R. A randomised controlled trial of vitamin D and omega-3 long chain polyunsaturated fatty acids in the treatment of irritability and hyperactivity among children with autism spectrum disorder. J. steroid Biochem. Mol. Biol. 2019, 187, 9–16. [Google Scholar] [CrossRef]
- El-Ansary, A.; Bhat, R.S. Targeting gut microbiota as a possible therapeutic intervention in autism. In Autism 360°; Elsevier: Amsterdam, The Netherlands, 2020; pp. 301–327. [Google Scholar]
- Das, U. Long-chain polyunsaturated fatty acids in the growth and development of the brain and memory. Nutrition 2003, 19, 62. [Google Scholar] [CrossRef]
- Robertson, R.C.; Oriach, C.S.; Murphy, K.; Moloney, G.M.; Cryan, J.F.; Dinan, T.G.; Ross, R.P.; Stanton, C. Omega-3 polyunsaturated fatty acids critically regulate behaviour and gut microbiota development in adolescence and adulthood. Brain Behav. Immun. 2017, 59, 21–37. [Google Scholar] [CrossRef]
- Maukonen, J.; Saarela, M. Human gut microbiota: Does diet matter? Proc. Natl. Acad. Sci. USA 2015, 74, 23–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simoes, C.D.; Maukonen, J.; Kaprio, J.; Rissanen, A.; Pietiläinen, K.H.; Saarela, M. Habitual dietary intake is associated with stool microbiota composition in monozygotic twins. J. Nutr. 2013, 143, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Wall, R.; Marques, T.M.; O’Sullivan, O.; Ross, R.P.; Shanahan, F.; Quigley, E.M.; Dinan, T.G.; Kiely, B.; Fitzgerald, G.F.; Cotter, P.D. Contrasting effects of Bifidobacterium breve NCIMB 702258 and Bifidobacterium breve DPC 6330 on the composition of murine brain fatty acids and gut microbiota. Am. J. Clin. Nutr. 2012, 95, 1278–1287. [Google Scholar] [CrossRef] [Green Version]
- Willemsen, L.E.; Koetsier, M.A.; Balvers, M.; Beermann, C.; Stahl, B.; van Tol, E.A. Polyunsaturated fatty acids support epithelial barrier integrity and reduce IL-4 mediated permeability in vitro. Eur. J. Nutr. 2008, 47, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Depino, A.M. Peripheral and central inflammation in autism spectrum disorders. Mol. Cell. Neurosci. 2013, 53, 69–76. [Google Scholar] [CrossRef]
- Costantini, L.; Molinari, R.; Farinon, B.; Merendino, N. Impact of omega-3 fatty acids on the gut microbiota. Int. J. Mol. Sci. 2017, 18, 2645. [Google Scholar] [CrossRef] [Green Version]
- Petrovic, S.; Arsic, A.; Ristic-Medic, D.; Cvetkovic, Z.; Vucic, V. Lipid Peroxidation and Antioxidant Supplementation in Neurodegenerative Diseases: A Review of Human Studies. Antioxidants 2020, 9, 1128. [Google Scholar] [CrossRef]
- Martins, B.P.; Bandarra, N.M.; Figueiredo-Braga, M. The role of marine omega-3 in human neurodevelopment, including Autism Spectrum Disorders and Attention-Deficit/Hyperactivity Disorder–a review. Crit. Rev. Food Sci. Nutr. 2020, 60, 1431–1446. [Google Scholar] [CrossRef]
- Arsić, A.; Vučić, V.; Prekajski, N.; Tepšić, J.; Ristić-Medić, D.; Veličković, V.; Glibetić, M. Different fatty acid composition of serum phospholipids of small and appropriate for gestational age preterm infants and of milk from their mothers. Hippokratia 2012, 16, 230. [Google Scholar]
- Fujiwara, T.; Morisaki, N.; Honda, Y.; Sampei, M.; Tani, Y. Chemicals, nutrition, and autism spectrum disorder: A mini-review. Front. Neurosci. 2016, 10, 174. [Google Scholar] [CrossRef] [Green Version]
- Steenweg-de Graaff, J.; Tiemeier, H.; Ghassabian, A.; Rijlaarsdam, J.; Jaddoe, V.W.; Verhulst, F.C.; Roza, S.J. Maternal fatty acid status during pregnancy and child autistic traits: The generation R study. Am. J. Epidemiol. 2016, 183, 792–799. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Iosif, A.-M.; Hansen, R.L.; Schmidt, R.J. Maternal polyunsaturated fatty acids and risk for autism spectrum disorder in the MARBLES high-risk study. Autism 2020, 24, 1191–1200. [Google Scholar] [CrossRef] [PubMed]
- Amminger, G.P.; Berger, G.E.; Schäfer, M.R.; Klier, C.; Friedrich, M.H.; Feucht, M. Omega-3 fatty acids supplementation in children with autism: A double-blind randomized, placebo-controlled pilot study. Biol. Psychiatry 2007, 61, 551–553. [Google Scholar] [CrossRef] [PubMed]
- Bent, S.; Hendren, R.L.; Zandi, T.; Law, K.; Choi, J.-E.; Widjaja, F.; Kalb, L.; Nestle, J.; Law, P. Internet-based, randomized, controlled trial of omega-3 fatty acids for hyperactivity in autism. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 658–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yui, K.; Koshiba, M.; Nakamura, S.; Kobayashi, Y. Effects of large doses of arachidonic acid added to docosahexaenoic acid on social impairment in individuals with autism spectrum disorders: A double-blind, placebo-controlled, randomized trial. J. Clin. Psychopharmacol. 2012, 32, 200–206. [Google Scholar] [CrossRef]
- Ornoy, A.; Weinstein-Fudim, L.; Ergaz, Z. Prevention or amelioration of autism-like symptoms in animal models: Will it bring us closer to treating human ASD? Int. J. Mol. Sci. 2019, 20, 1074. [Google Scholar] [CrossRef] [Green Version]
- Mankad, D.; Dupuis, A.; Smile, S.; Roberts, W.; Brian, J.; Lui, T.; Genore, L.; Zaghloul, D.; Iaboni, A.; Marcon, P.M.A. A randomized, placebo controlled trial of omega-3 fatty acids in the treatment of young children with autism. Mol. Autism 2015, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Mazahery, H.; Conlon, C.A.; Beck, K.L.; Mugridge, O.; Kruger, M.C.; Stonehouse, W.; Camargo, C.A.; Meyer, B.J.; Tsang, B.; von Hurst, P.R. Inflammation (IL-1β) Modifies the Effect of Vitamin D and Omega-3 Long Chain Polyunsaturated Fatty Acids on Core Symptoms of Autism Spectrum Disorder—An Exploratory Pilot Study. Nutrients 2020, 12, 661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doaei, S.; Bourbour, F.; Teymoori, Z.; Jafari, F.; Kalantari, N.; Abbas Torki, N.; Gorgani, N.; Gholamalizadeh, M. The effect of omega-3 fatty acids supplementation on social and behavioral disorders of children with autism: A randomized clinical trial. Pediatric Endocrinol. Diabetes Metab. 2021, 27, 12–18. [Google Scholar] [CrossRef]
- Raine, A.; Ang, R.P.; Choy, O.; Hibbeln, J.R.; Ho, R.M.; Lim, C.G.; Lim-Ashworth, N.S.; Ling, S.; Liu, J.C.; Ooi, Y.P. Omega-3 (ω-3) and social skills interventions for reactive aggression and childhood externalizing behavior problems: A randomized, stratified, double-blind, placebo-controlled, factorial trial. Psychol. Med. 2019, 49, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Keim, S.A.; Gracious, B.; Boone, K.M.; Klebanoff, M.A.; Rogers, L.K.; Rausch, J.; Coury, D.L.; Sheppard, K.W.; Husk, J.; Rhoda, D.A. ω-3 and ω-6 fatty acid supplementation may reduce autism symptoms based on parent report in preterm toddlers. J. Nutr. 2018, 148, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Parellada, M.; Llorente, C.; Calvo, R.; Gutierrez, S.; Lázaro, L.; Graell, M.; Guisasola, M.; Dorado, M.L.; Boada, L.; Romo, J. Randomized trial of omega-3 for autism spectrum disorders: Effect on cell membrane composition and behavior. Eur. Neuropsychopharmacol. 2017, 27, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Voigt, R.G.; Mellon, M.W.; Katusic, S.K.; Weaver, A.L.; Matern, D.; Mellon, B.; Jensen, C.L.; Barbaresi, W.J. Dietary docosahexaenoic acid supplementation in children with autism. J. Pediatric Gastroenterol. Nutr. 2014, 58, 715–722. [Google Scholar] [CrossRef]
- Meguid, N.A.; Atta, H.M.; Gouda, A.S.; Khalil, R.O. Role of polyunsaturated fatty acids in the management of Egyptian children with autism. Clin. Biochem. 2008, 41, 1044–1048. [Google Scholar] [CrossRef]


{kind=link}
| Study | Trial Design | Drugs and Dose | Participants | Treatment Duration | Results |
|---|---|---|---|---|---|
| Amminger et al., 2007 [50] | a randomized, double-blind, placebo-controlled pilot trial | 0.84 g/day EPA 0.7 g/day DHA | 13 children with autistic disorders, age 5–17 | 6 weeks |
|
| Bent et al., 2014 [51] | internet-based, randomized controlled trial | 1.3 g of omega-3 PUFA (350 mg of EPA and 230 mg of DHA) or placebo | 57 ASD children with hyperactivity (5–8 years) | 6 weeks |
|
| Yui et al., 2012 [52] | double-blind, randomized, placebo-controlled trial | 0.24 g/day DHA and 0.24 g/day AA per day | 13 ASD children (6–28 years) | 16 weeks |
|
| Voigt et al., 2014 [53] | randomized double-blind placebo-controlled trial | DHA supplementation of 200 mg/day or placebo | 48 children with ASD (3–10 years) | 26 weeks |
|
| Meguid et al., 2008 [56] | randomized, placebo-controlled trial | 60 mg of DHA, 12 mg of GLA, 13 mg of EPA and 5 mg of AA | 30 autistic children (3–11 years) and 30 healthy children as control | 3 months |
|
| Sheppard et al., 2017 [30] | pilot trial, single-site, double blinded, RCT | 2.5 ml omega-3 (338 mg EPA, 225 mg DHA); 280 mg omega-6 FA(83 mg GLA); 306 mg n-9 FA | 31 preterm children exhibiting ASD, 18–38 months of old born at ≤29 weeks of gestation | 3 months |
|
| Parellada et al., 2017 [57] | a randomized, crossover, placebo-controlled study | omega-3 (EPA+DHA, 33%+22%) and vitamin E as a stabilizer Subjects 5–11 years old – EPA 577.5 mg qd + DHA 385 mg qd + vitamin E 1.6 mg qd; 12–17 years – EPA 693 mg qd + DHA 462 mg qd + vitamin E 2.01 mg qd | 68 children and adolescents with ASD (5–17 years old) | 8 weeks |
|
| Raine et al., 2018 [58] | randomized, double-blind, stratified, placebo controlled, 2 × 2 factorial trial | 1.12 g of omega-3 daily (411.2 mg DHA, 106.4 mg DPA, and 604 mg of EPA) | 282 children with externalizing behavior disorder (7–16 years) | 6 months |
|
| Mazahery et al., 2019 [33] | randomized placebo controlled double-blind study design | vitamin D (2000 IU/day, vitamin D), omega-3 LCPUFA (722 mg/day DHA, OM) or both | 117 children (2.5 to 8 years) with ASD | 12 months |
|
| Keim et al., 2018 [60] | randomized, fully blinded, placebo-controlled trial | omega-3-6-9 (338 mg EPA, 225 mg DHA, and 83 mg GLA) VS. canola oil (124 mg palmitic acid, 39 mg stearic acid, 513 mg linoleic acid, 225 mg α-linolenic acid, and 1346 mg oleic acid) | 31 children born at ≤29 week of gestation (18–38 months of age) | 3 months |
|
| Doaei et al., 2021 [61] | double-blind, randomized clinical trial | group (1): 1 gram omega-3 Long Chain (180 mg EPA + 120 mg DHA) and Group (2) 1 gram medium chain triglyceride as placebo | 54 children with autism assigned to the case (n = 28) and control (n = 26) groups (5–15 years) | 8 weeks |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veselinović, A.; Petrović, S.; Žikić, V.; Subotić, M.; Jakovljević, V.; Jeremić, N.; Vučić, V. Neuroinflammation in Autism and Supplementation Based on Omega-3 Polyunsaturated Fatty Acids: A Narrative Review. Medicina 2021, 57, 893. https://doi.org/10.3390/medicina57090893
Veselinović A, Petrović S, Žikić V, Subotić M, Jakovljević V, Jeremić N, Vučić V. Neuroinflammation in Autism and Supplementation Based on Omega-3 Polyunsaturated Fatty Acids: A Narrative Review. Medicina. 2021; 57(9):893. https://doi.org/10.3390/medicina57090893
Chicago/Turabian StyleVeselinović, Aleksandra, Snježana Petrović, Vladica Žikić, Miško Subotić, Vladimir Jakovljević, Nevena Jeremić, and Vesna Vučić. 2021. "Neuroinflammation in Autism and Supplementation Based on Omega-3 Polyunsaturated Fatty Acids: A Narrative Review" Medicina 57, no. 9: 893. https://doi.org/10.3390/medicina57090893