
Features of Patients Receiving Extracorporeal Membrane Oxygenation Relative to Cardiogenic Shock Onset: A Single-Centre Experience

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
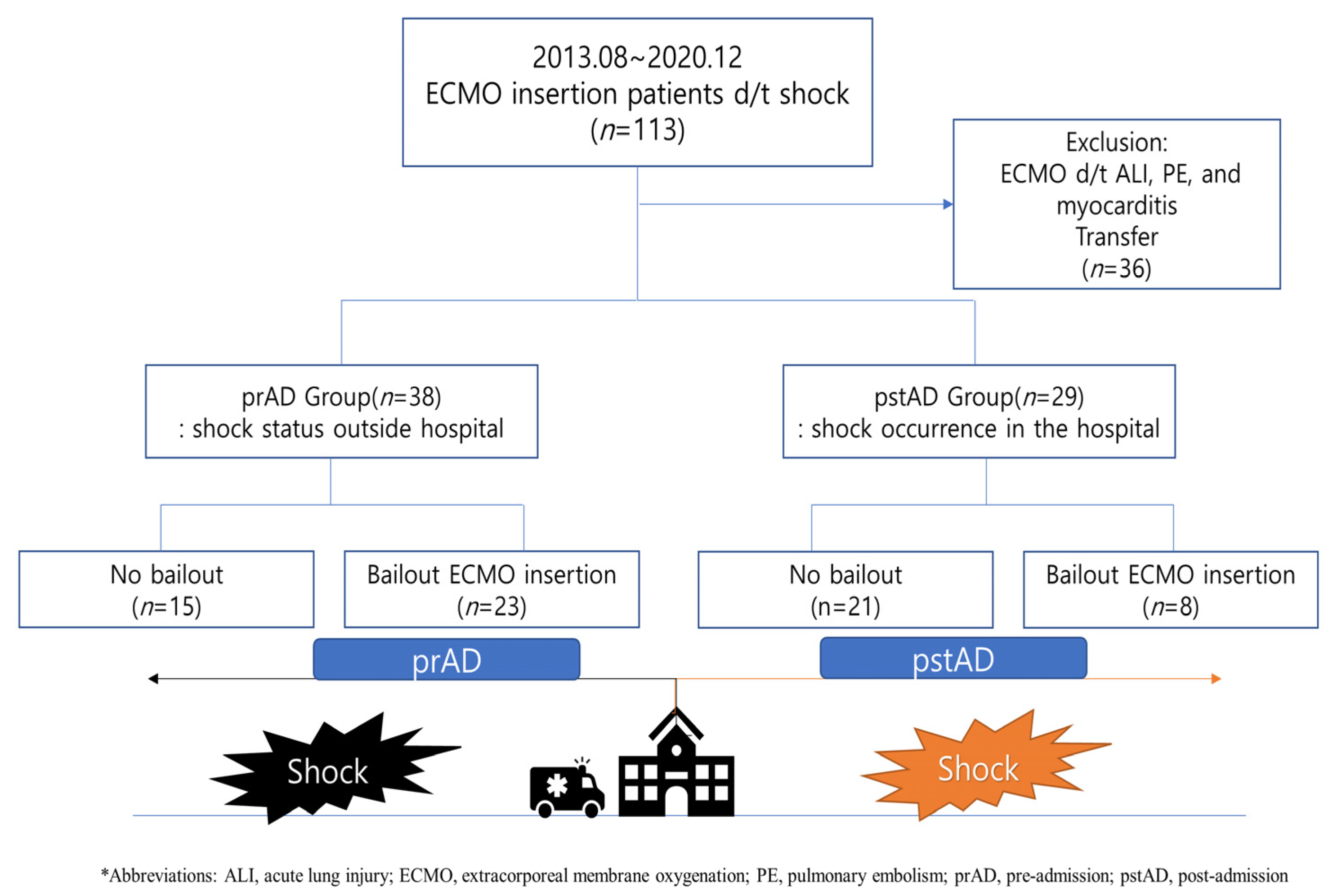
2.1. Study Population
2.2. Coronary Intervention, ECMO Insertion, and Control
2.3. Primary Endpoint and Subgroup Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
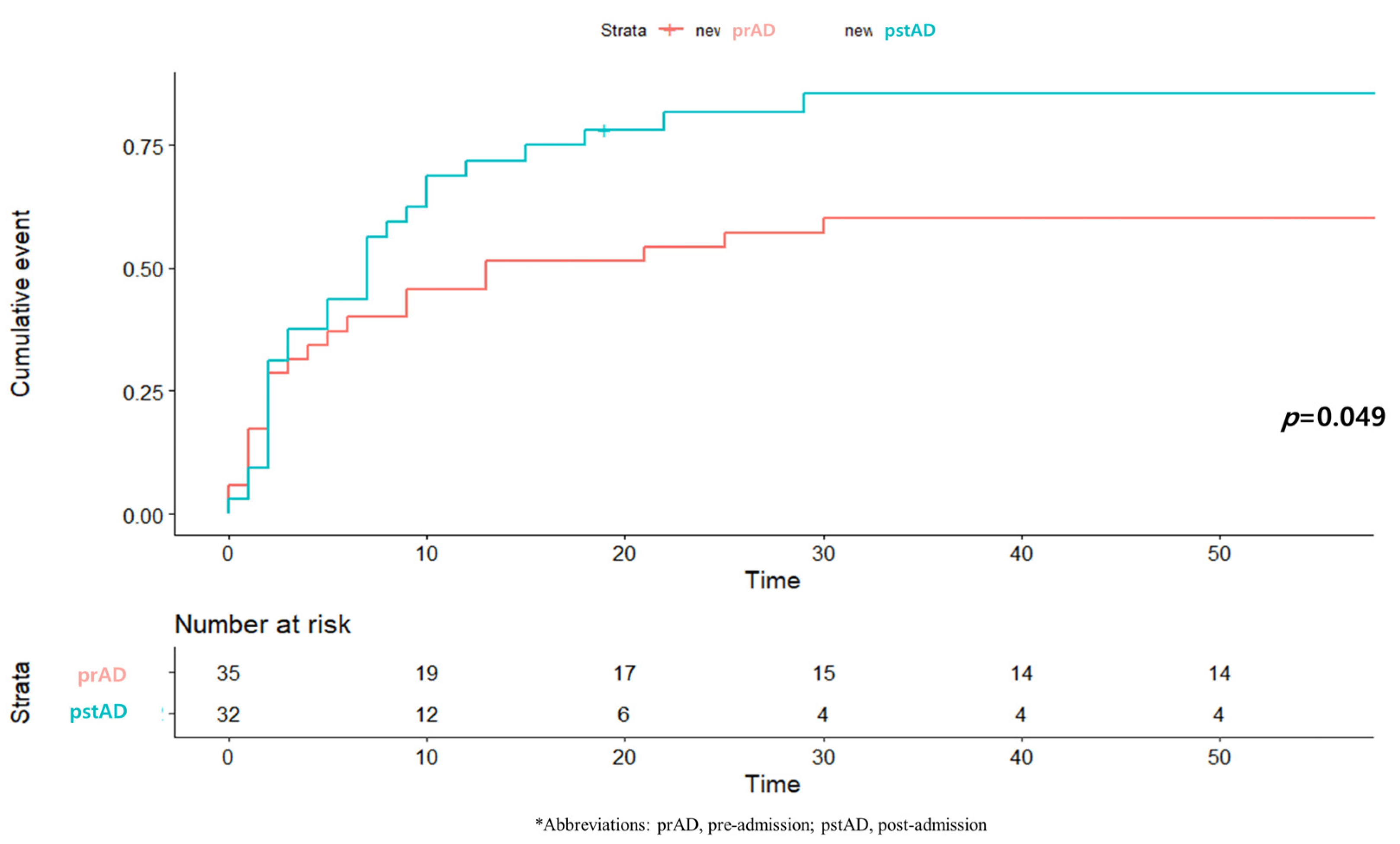
3.2. One-Month Mortality and Related Factors
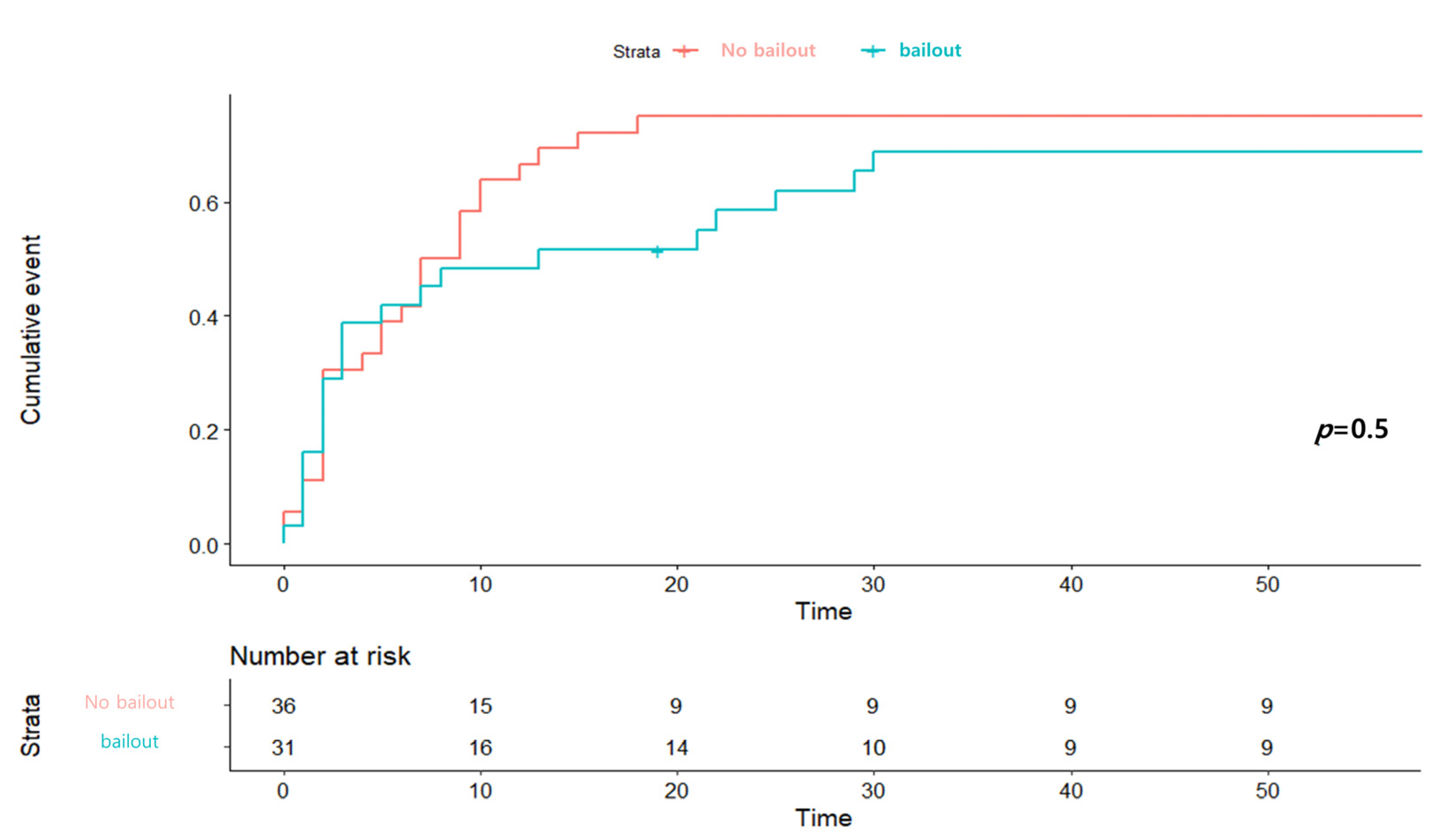
3.3. Subgroup Analysis of Bailout ECMO
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CPR | cardiopulmonary resuscitation |
| CS | cardiogenic shock |
| ECMO | Extracorporeal membrane oxygenation |
| ECPR | extracorporeal CPR |
| ED | emergency department |
| IHCAs | in-hospital cardiac arrests |
| LAD | left anterior descending artery |
| MCS | mechanical circulatory support |
| MI | myocardial infarction |
| OHCAs | Out-of-hospital cardiac arrests |
| sBP | systolic blood pressure |
| STEMI | ST-segment elevation myocardial infarction |
References
- Choudhury, T.; West, N.E.; El-Omar, M. ST elevation myocardial infarction. Clin. Med. 2016, 16, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Miyachi, H.; Takagi, A.; Miyauchi, K.; Yamasaki, M.; Tanaka, H.; Yoshikawa, M.; Saji, M.; Suzuki, M.; Yamamoto, T.; Shimizu, W.; et al. Current characteristics and management of ST elevation and non-ST elevation myocardial infarction in the Tokyo metropolitan area: From the Tokyo CCU network registered cohort. Heart Vessels 2016, 31, 1740–1751. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, R.J.; Gore, J.M.; Alpert, J.S.; Osganian, V.; de Groot, J.; Bade, J.; Chen, Z.; Frid, D.; Dalen, J.E. Cardiogenic shock after acute myocardial infarction. Incidence and mortality from a community-wide perspective, 1975 to 1988. N. Engl. J. Med. 1991, 325, 1117–1122. [Google Scholar] [CrossRef]
- Vahdatpour, C.; Collins, D.; Goldberg, S. Cardiogenic Shock. J. Am. Heart Assoc. 2019, 8, e011991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeger, R.V.; Radovanovic, D.; Hunziker, P.R.; Pfisterer, M.E.; Stauffer, J.C.; Erne, P.; Urban, P.; Investigators, A.P.R. Ten-year trends in the incidence and treatment of cardiogenic shock. Ann. Intern. Med. 2008, 149, 618–626. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Dzavik, V.; Buller, C.E.; Aylward, P.; Col, J.; White, H.D.; Investigators, S. Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA 2006, 295, 2511–2515. [Google Scholar] [CrossRef] [Green Version]
- Spence, N.; Abbott, J.D. Coronary Revascularization in Cardiogenic Shock. Curr. Treat. Options Cardiovasc. Med. 2016, 18, 1. [Google Scholar] [CrossRef]
- Rihal, C.S.; Naidu, S.S.; Givertz, M.M.; Szeto, W.Y.; Burke, J.A.; Kapur, N.K.; Kern, M.; Garratt, K.N.; Goldstein, J.A.; Dimas, V.; et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care: Endorsed by the American Heart Assocation, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’intervention. J. Am. Coll. Cardiol. 2015, 65, e7–e26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.S.; Yu, H.Y.; Huang, S.C.; Lin, J.W.; Chi, N.H.; Wang, C.H.; Wang, S.S.; Lin, F.Y.; Ko, W.J. Extracorporeal membrane oxygenation support can extend the duration of cardiopulmonary resuscitation. Crit. Care Med. 2008, 36, 2529–2535. [Google Scholar] [CrossRef]
- Chen, Y.S.; Lin, J.W.; Yu, H.Y.; Ko, W.J.; Jerng, J.S.; Chang, W.T.; Chen, W.J.; Huang, S.C.; Chi, N.H.; Wang, C.H.; et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: An observational study and propensity analysis. Lancet 2008, 372, 554–561. [Google Scholar] [CrossRef]
- Wang, C.H.; Chou, N.K.; Becker, L.B.; Lin, J.W.; Yu, H.Y.; Chi, N.H.; Hunag, S.C.; Ko, W.J.; Wang, S.S.; Tseng, L.J.; et al. Improved outcome of extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest—A comparison with that for extracorporeal rescue for in-hospital cardiac arrest. Resuscitation 2014, 85, 1219–1224. [Google Scholar] [CrossRef]
- Kim, H.; Cho, Y.H. Role of extracorporeal cardiopulmonary resuscitation in adults. Acute Crit. Care 2020, 35, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Rhee, T.M.; Hahn, J.Y.; Kim, H.K.; Park, J.; Hwang, D.; Choi, K.H.; Kim, J.; Park, T.K.; Yang, J.H.; et al. Multivessel Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction with Cardiogenic Shock. J. Am. Coll. Cardiol. 2018, 71, 844–856. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2016, 67, 1235–1250. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.C.; Sleeper, L.A.; Monrad, E.S.; Menegus, M.A.; Palazzo, A.; Dzavik, V.; Jacobs, A.; Jiang, X.; Hochman, J.S.; Investigators, S. Absence of gender differences in clinical outcomes in patients with cardiogenic shock complicating acute myocardial infarction. A report from the SHOCK Trial Registry. J. Am. Coll. Cardiol. 2001, 38, 1395–1401. [Google Scholar] [CrossRef] [Green Version]
- Sadowski, M.; Gutkowski, W.; Raczynski, G.; Gierlotka, M.; Polonski, L. Mortality in cardiogenic shock complicating acute myocardial infarction due to left main coronary artery disease: Does gender matter? Przegl. Lek. 2014, 71, 117–121. [Google Scholar] [PubMed]
- Vallabhajosyula, S.; Vallabhajosyula, S.; Dunlay, S.M.; Hayes, S.N.; Best, P.J.M.; Brenes-Salazar, J.A.; Lerman, A.; Gersh, B.J.; Jaffe, A.S.; Bell, M.R.; et al. Sex and Gender Disparities in the Management and Outcomes of Acute Myocardial Infarction-Cardiogenic Shock in Older Adults. Mayo Clin. Proc. 2020, 95, 1916–1927. [Google Scholar] [CrossRef] [PubMed]
- Hoybye, M.; Stankovic, N.; Holmberg, M.; Christensen, H.C.; Granfeldt, A.; Andersen, L.W. In-Hospital vs. Out-of-Hospital Cardiac Arrest: Patient Characteristics and Survival. Resuscitation 2021, 158, 157–165. [Google Scholar] [CrossRef]
- Goldberger, Z.D.; Chan, P.S.; Berg, R.A.; Kronick, S.L.; Cooke, C.R.; Lu, M.; Banerjee, M.; Hayward, R.A.; Krumholz, H.M.; Nallamothu, B.K.; et al. Duration of resuscitation efforts and survival after in-hospital cardiac arrest: An observational study. Lancet 2012, 380, 1473–1481. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, J.C.; Frisch, A.; Rittenberger, J.C.; Callaway, C.W. Duration of resuscitation efforts and functional outcome after out-of-hospital cardiac arrest: When should we change to novel therapies? Circulation 2013, 128, 2488–2494. [Google Scholar] [CrossRef] [PubMed]
- McNally, B.; Robb, R.; Mehta, M.; Vellano, K.; Valderrama, A.L.; Yoon, P.W.; Sasson, C.; Crouch, A.; Perez, A.B.; Merritt, R.; et al. Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill. Summ. 2011, 60, 1–19. [Google Scholar]
- Peberdy, M.A.; Kaye, W.; Ornato, J.P.; Larkin, G.L.; Nadkarni, V.; Mancini, M.E.; Berg, R.A.; Nichol, G.; Lane-Trultt, T. Cardiopulmonary resuscitation of adults in the hospital: A report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation 2003, 58, 297–308. [Google Scholar] [CrossRef]
- Goldberg, R.J.; Spencer, F.A.; Gore, J.M.; Lessard, D.; Yarzebski, J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: A population-based perspective. Circulation 2009, 119, 1211–1219. [Google Scholar] [CrossRef] [Green Version]
- Keebler, M.E.; Haddad, E.V.; Choi, C.W.; McGrane, S.; Zalawadiya, S.; Schlendorf, K.H.; Brinkley, D.M.; Danter, M.R.; Wigger, M.; Menachem, J.N.; et al. Venoarterial Extracorporeal Membrane Oxygenation in Cardiogenic Shock. JACC Heart Fail. 2018, 6, 503–516. [Google Scholar] [CrossRef]
- Rao, P.; Khalpey, Z.; Smith, R.; Burkhoff, D.; Kociol, R.D. Venoarterial Extracorporeal Membrane Oxygenation for Cardiogenic Shock and Cardiac Arrest. Circ. Heart Fail. 2018, 11, e004905. [Google Scholar] [CrossRef]
- De Charriere, A.; Assouline, B.; Scheen, M.; Mentha, N.; Banfi, C.; Bendjelid, K.; Giraud, R. ECMO in Cardiac Arrest: A Narrative Review of the Literature. J. Clin. Med. 2021, 10, 534. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, T.; Morimura, N.; Nagao, K.; Asai, Y.; Yokota, H.; Nara, S.; Hase, M.; Tahara, Y.; Atsumi, T.; Group, S.-J.S. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: A prospective observational study. Resuscitation 2014, 85, 762–768. [Google Scholar] [CrossRef]
- Wengenmayer, T.; Rombach, S.; Ramshorn, F.; Biever, P.; Bode, C.; Duerschmied, D.; Staudacher, D.L. Influence of low-flow time on survival after extracorporeal cardiopulmonary resuscitation (eCPR). Crit. Care 2017, 21, 157. [Google Scholar] [CrossRef] [PubMed]
- Link, M.S.; Berkow, L.C.; Kudenchuk, P.J.; Halperin, H.R.; Hess, E.P.; Moitra, V.K.; Neumar, R.W.; O’Neil, B.J.; Paxton, J.H.; Silvers, S.M.; et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S444–S464. [Google Scholar] [CrossRef] [PubMed]
- Mandawat, A.; Rao, S.V. Percutaneous Mechanical Circulatory Support Devices in Cardiogenic Shock. Circ. Cardiovasc. Interv. 2017, 10, e004337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagani, F.D.; Lynch, W.; Swaniker, F.; Dyke, D.B.; Bartlett, R.; Koelling, T.; Moscucci, M.; Deeb, G.M.; Bolling, S.; Monaghan, H.; et al. Extracorporeal life support to left ventricular assist device bridge to heart transplant: A strategy to optimize survival and resource utilization. Circulation 1999, 100, II206–II210. [Google Scholar] [CrossRef] [PubMed]
- Hoefer, D.; Ruttmann, E.; Poelzl, G.; Kilo, J.; Hoermann, C.; Margreiter, R.; Laufer, G.; Antretter, H. Outcome evaluation of the bridge-to-bridge concept in patients with cardiogenic shock. Ann. Thorac. Surg. 2006, 82, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Society of Thoracic Surgeons Blood Conservation Guideline Task Force; Ferraris, V.A.; Brown, J.R.; Despotis, G.J.; Hammon, J.W.; Reece, T.B.; Saha, S.P.; Song, H.K.; Clough, E.R.; Society of Cardiovascular Anesthesiologists Special Task Force on Blood Transfusion; et al. 2011 update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines. Ann. Thorac. Surg. 2011, 91, 944–982. [Google Scholar] [CrossRef]
- Lorusso, R.; Centofanti, P.; Gelsomino, S.; Barili, F.; Di Mauro, M.; Orlando, P.; Botta, L.; Milazzo, F.; Actis Dato, G.; Casabona, R.; et al. Venoarterial Extracorporeal Membrane Oxygenation for Acute Fulminant Myocarditis in Adult Patients: A 5-Year Multi-Institutional Experience. Ann. Thorac. Surg. 2016, 101, 919–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burrell, A.J.; Pellegrino, V.A.; Wolfe, R.; Wong, W.K.; Cooper, D.J.; Kaye, D.M.; Pilcher, D.V. Long-term survival of adults with cardiogenic shock after venoarterial extracorporeal membrane oxygenation. J. Crit. Care 2015, 30, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Zavalichi, M.A.; Nistor, I.; Nedelcu, A.E.; Zavalichi, S.D.; Georgescu, C.M.A.; Statescu, C.; Covic, A. Extracorporeal Membrane Oxygenation in Cardiogenic Shock due to Acute Myocardial Infarction: A Systematic Review. Biomed. Res. Int 2020, 2020, 6126534. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pre-Admission Group (n = 35) | Post-Admission Group (n = 32) | p-Value | |
|---|---|---|---|
| Age (years) | 65.0 (55.0–73.0) | 68.5 (60.5–77.0) | 0.46 |
| Males, n (%) | 29 (82.9) | 22 (68.8) | 0.29 |
| BMI, kg/m2 | 23.2 (20.7–24.7) | 25.2 (22.0–27.4) | 0.03 |
| Cardiovascular risk factors | |||
| Smoking | 9 (25.7) | 4 (12.5) | 0.32 |
| Hypertension | 13 (37.1) | 20 (62.5) | 0.07 |
| Diabetes mellitus | 14 (40.0) | 12 (37.5) | 1.00 |
| Chronic kidney disease | 1 (2.9) | 7 (21.9) | 0.04 |
| Stroke | 2 (5.7) | 1 (3.1) | 1.00 |
| Previous PCI | 6 (17.1) | 3 (9.4) | 0.57 |
| Past medical history | |||
| Aspirin | 11 (31.4) | 4 (12.5) | 0.12 |
| Clopidogrel | 4 (11.4) | 0 (0) | 0.15 |
| Statins | 4 (11.4) | 6 (18.8) | 0.62 |
| ACEi/ARB | 5 (14.3) | 6 (18.8) | 0.87 |
| Calcium channel blocker | 4 (11.4) | 4 (12.5) | 1.00 |
| Initial electrocardiogram | |||
| ST-segment elevation | 18 (51.4) | 17 (53.1) | 1.00 |
| Non-ST-segment elevation | 2 (5.7) | 14 (43.8) | 0.001 |
| Asystole | 9 (25.7) | 1 (3.1) | 0.03 |
| Ventricular fibrillation | 4 (11.4) | 0 (0.0) | 0.15 |
| EF after revascularization | 24.0 (16.0–30.0) | 19.5 (13.0–39.5) | 0.64 |
| Laboratory findings | |||
| WBC (×103/uL) | 12.9 (9.8–15.0) | 12.6 (8.4–16.6) | 0.76 |
| Haemoglobin (g/dL) | 13.6 (12.8–14.9) | 11.8 (10.0–13.7) | 0.01 |
| Platelets (×103/uL 5) | 248.0 (168.5–309.0) | 196.0 (165.5–260.0) | 0.10 |
| Creatinine (mg/dL) | 1.1 (1.0–1.4) | 1.5 (1.1–2.0) | 0.02 |
| Creatine kinase-MB (ng/mL) | 3.3 (1.8–21.7) | 22.4 (3.5–97.6) | 0.01 |
| Troponin I (pg/mL) | 8.2 (1.1–162.1) | 71.8 (2.0–5981.4) | 0.06 |
| BNP (pg/dL) | 161.2 (39.9–292.4) | 326.6 (55.1–855.5) | 0.58 |
| Inotropes | |||
| Dopamine | 30 (85.7) | 29 (90.6) | 0.81 |
| Dobutamine | 7 (20.0) | 9 (28.2) | 0.57 |
| Norepinephrine | 31 (88.6) | 25 (78.1) | 0.41 |
| Coronary reperfusion strategy | |||
| PCI | 31 (88.6) | 32 (100.0) | 0.15 |
| CABG | 1 (2.8) | 0 (0.0) | 1.00 |
| Fail or none | 3 (8.6) | 0 (0.0) | 0.27 |
| Total (n = 67) | Pre-Admission Group (n = 35) | Post-Admission Group (n = 32) | p-Value | |
|---|---|---|---|---|
| CPR | 44 (65.7) | 28 (80.0) | 17 (53.1) | 0.02 |
| CPR duration (min) | 32.5 (14.5–53.5) | 43.5 (18.0–55.5) | 30.0 (13.0–43.0) | 0.19 |
| Shock to CPR interval (min) | 8.5 (1.5–55.0) | 5.0 (0–14.5) | 50.0 (7.0–237.0) | <0.01 |
| Shock to ECMO interval (min) | 92.0 (54.0–148.0) | 92.0 (63.5–148.0) | 90.0 (51.0–190.0) | 0.79 |
| Shock to reperfusion interval (min) | 65.0 (1.5–113.0) | 69.0 (47.0–106.5) | 35.0 (−139.0–115.5) | 0.09 |
| ECMO duration | 5.0 (2.0–8.0) | 5.0 (2.0–7.0) | 6.0 (2.0–8.5) | 0.37 |
| Bailout ECMO | 31 (46.3) | 20 (57.1) | 11 (34.4) | 0.06 |
| Culprit site | ||||
| LM | 9 (13.4) | 6 (17.1) | 3 (9.4) | 0.57 |
| LAD | 34 (50.7) | 17 (48.6) | 17 (53.1) | 0.90 |
| LCx | 6 (9.0) | 3 (8.6) | 3 (9.4) | 1.00 |
| RCA | 18 (26.9) | 9 (25.7) | 9 (28.1) | 1.00 |
| Hospital duration | 10.0 (3.0–23.5) | 11.0 (2.0–25.5) | 9.0 (5.0–21.0) | 0.95 |
| 1-Month mortality | 48 (71.6) | 21 (60.0) | 27 (84.4) | 0.03 |
| Values | Hazard Ratio | |||
|---|---|---|---|---|
| Univariable Analysis | p-Value | Multivariable Analysis | p-Value | |
| Age (≥70 years) | 2.22 (1.25–3.94) | 0.01 | 2.07 (1.15–3.73) | 0.02 |
| Male sex | 0.34 (0.18–0.63) | <0.01 | 0.38 (0.19–0.70) | <0.01 |
| Hypertension | 0.99 (0.56–1.74) | 0.97 | ||
| Diabetes mellitus | 0.98 (0.55–1.76) | 0.95 | ||
| Chronic kidney disease | 1.00 (0.43–2.36) | 0.99 | ||
| Stroke | 0.37 (0.05–2.68) | 0.32 | ||
| Previous PCI | 0.94 (0.42–2.09) | 0.88 | ||
| Aspirin | 0.59 (0.29–1.23) | 0.16 | ||
| Clopidogrel | 1.02 (0.32–3.33) | 0.96 | ||
| Statins | 0.95 (0.43–2.12) | 0.90 | ||
| ACEi/ARB | 0.61 (0.26–1.44) | 0.26 | ||
| CCB | 0.37 (0.11–1.19) | 0.09 | ||
| Post-revascularization EF (≥30%) | 0.79 (0.40–1.60) | 0.52 | ||
| CPR start (≤9 min) | 0.89 (0.47–1.73) | 0.73 | ||
| CPR duration | 1.01 (0.99–1.02) | 0.14 | ||
| ECMO duration (≥6 days) | 0.43 (0.24–0.77) | 0.005 | 0.38 (0.21–0.72) | 0.01 |
| PCI to LM or LAD | 1.15 (0.63–2.09) | 0.66 | ||
| Bailout ECMO | 0.82 (0.46–1.45) | 0.50 | ||
| In-hospital shock | 1.77 (0.99–3.16) | 0.053 | 2.02 (1.07–3.81) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.-G.; Shin, S.-D.; Han, D.; Kang, M.-K.; Lee, S.-H.; Kim, J.; Cho, J.-R.; Kim, K.; Choi, S.; Lee, N. Features of Patients Receiving Extracorporeal Membrane Oxygenation Relative to Cardiogenic Shock Onset: A Single-Centre Experience. Medicina 2021, 57, 886. https://doi.org/10.3390/medicina57090886
Shin D-G, Shin S-D, Han D, Kang M-K, Lee S-H, Kim J, Cho J-R, Kim K, Choi S, Lee N. Features of Patients Receiving Extracorporeal Membrane Oxygenation Relative to Cardiogenic Shock Onset: A Single-Centre Experience. Medicina. 2021; 57(9):886. https://doi.org/10.3390/medicina57090886
Chicago/Turabian StyleShin, Dong-Geum, Sang-Deock Shin, Donghoon Han, Min-Kyung Kang, Seung-Hun Lee, Jihoon Kim, Jung-Rae Cho, Kunil Kim, Seonghoon Choi, and Namho Lee. 2021. "Features of Patients Receiving Extracorporeal Membrane Oxygenation Relative to Cardiogenic Shock Onset: A Single-Centre Experience" Medicina 57, no. 9: 886. https://doi.org/10.3390/medicina57090886