
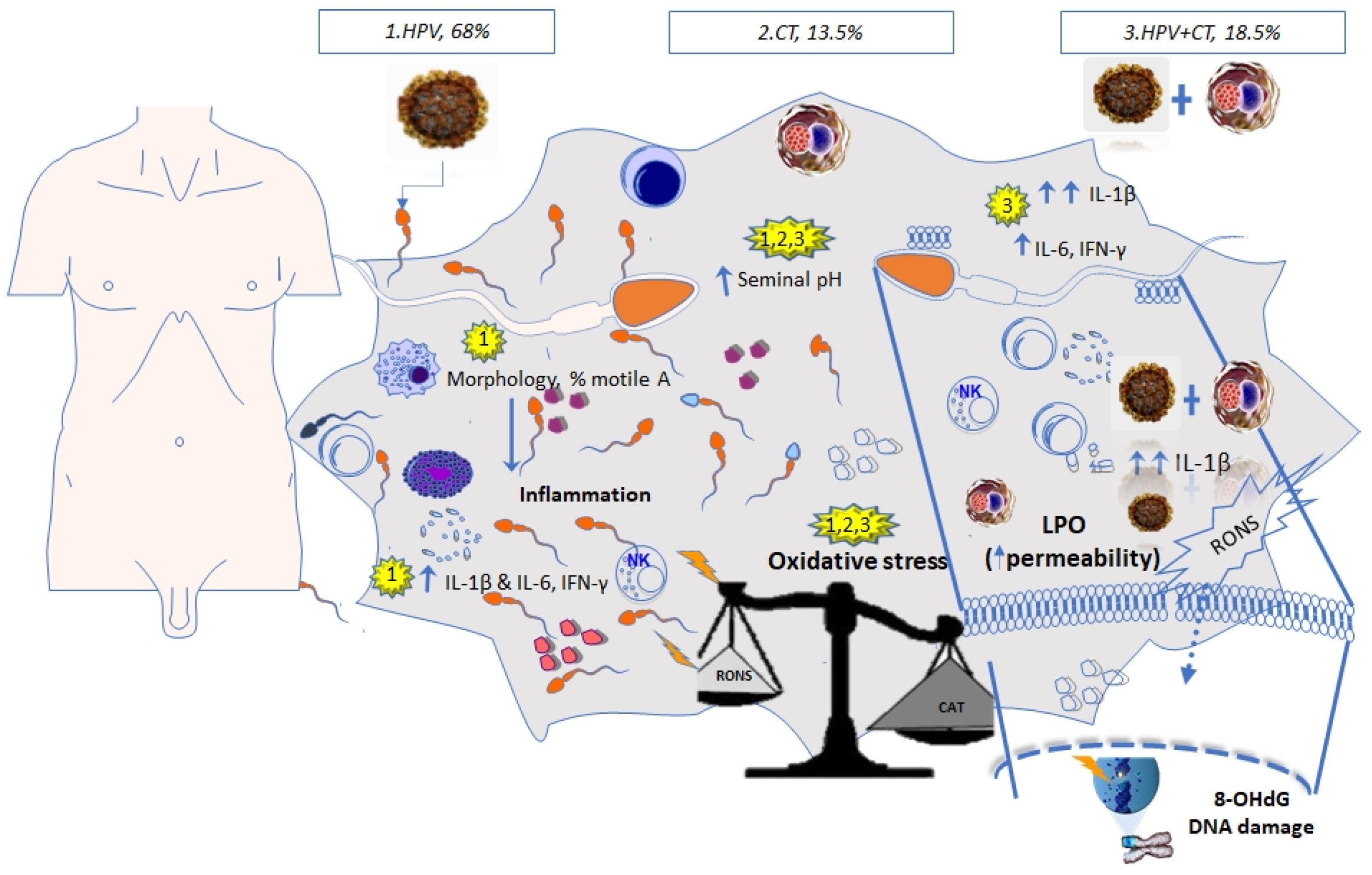
Proinflammatory and Oxidative Stress States Induced by Human Papillomavirus and Chlamydia trachomatis Coinfection Affect Sperm Quality in Asymptomatic Infertile Men

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Population
2.2. Semen Analysis
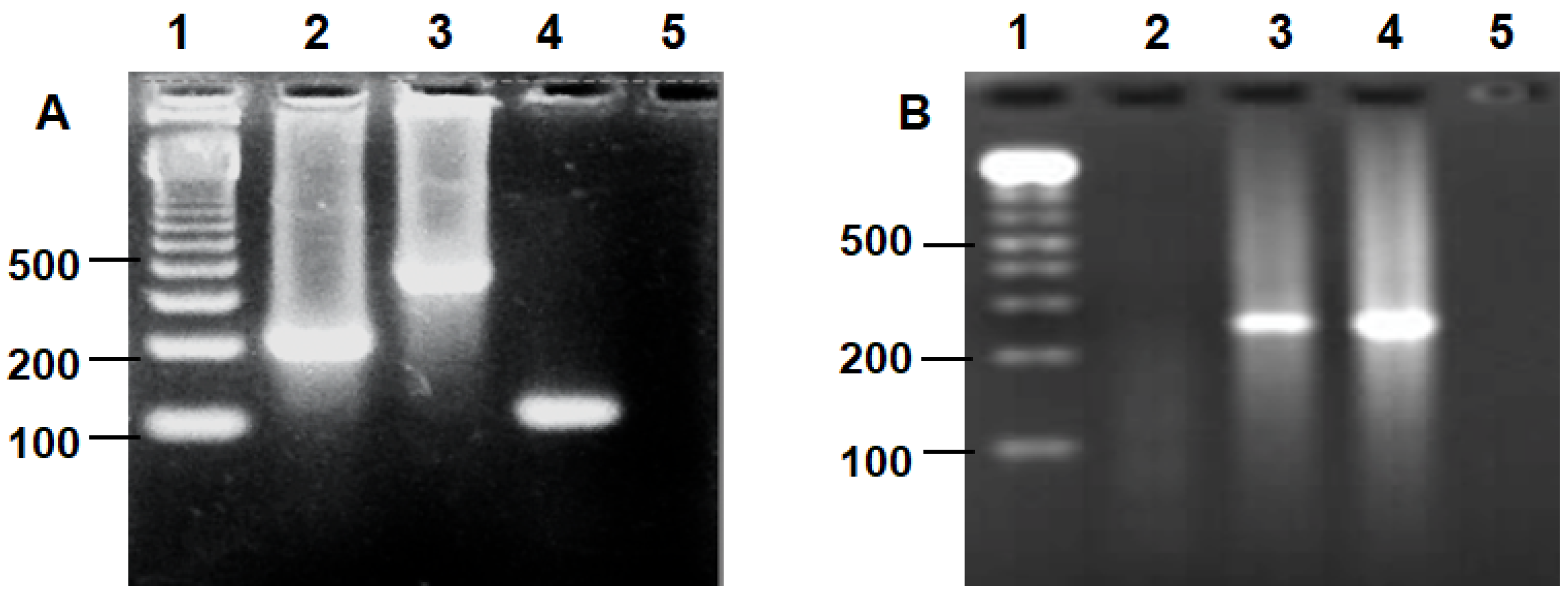
2.3. Detection of HPV and Chlamydia trachomatis by PCR
2.4. Cytokines in the Seminal Plasma
2.5. Assessment of Lipid Peroxidation in the Seminal Plasma
2.6. 8-Hydroxydeoxyguanosine Assay in the Seminal Plasma
2.7. Quantification of Total Antioxidant Capacity
2.8. Statistical Analysis
2.9. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Goulart, A.C.X.; Farnezi, H.C.M.; Medeiros, F.J.P.B.; Dos Santos, A.; Ramos, M.G.; Penna, M.L.F. HIV, HPV and Chlamydia trachomatis: Impacts on male fertility. JBRA Assist. Reprod. 2020, 24, 492–497. [Google Scholar] [CrossRef]
- Damke, E.; Kurscheidt, F.A.; Balani, V.A.; Takeda, K.I.; Irie, M.M.T.; Gimenes, F.; Consolaro, M.E.L. Male Partners of Infertile Couples with Seminal Infections of Human Papillomavirus Have Impaired Fertility Parameters. Biomed. Res. Int. 2017, 4684629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moazenchi, M.; Totonchi, M.; Salman, Y.R.; Hratian, K.; Mohseni, M.M.A.; Ahmadi, P.M.; Chehrazi, M.; Monseni, M.A. The impact of Chlamydia trachomatis infection on sperm parameters and male fertility: A comprehensive study. Int. J. STD AIDS 2017, 29, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Wagenlehner, F.M.E.; Mondaini, N.; Elia, C.D.; Meacci, F.; Migno, S.; Malossini, G.; Bartoletti, R. Effect of human papillomavirus and Chlamydia trachomatis co-infection on sperm quality in young heterosexual men with chronic prostatitis-related symptoms. BJU Int. 2014, 113, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foresta, C.; Patassini, C.; Bertoldo, A.; Menegazzo, M.; Francavilla, F.; Barzon, L.; Ferlin, A. Mechanism of Human Papillomavirus Binding to Human Spermatozoa and Fertilizing Ability of Infected Spermatozoa. PLoS ONE 2011, 6, e15036. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Jia, C.W.; Ma, Y.M.; Zhou, L.Y.; Wang, S.Y. Correlation between HPV sperm infection and male infertility. Asian J. Androl. 2013, 15, 529–532. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Soto, E.; Oros-Pantoja, R.; Fernández-Martínez, E.; Carbonell-Campos, J.M.; Sánchez-Monroy, V. Seminal pro-inflammatory cytokines and pH are affected by Chlamydia infection in asymptomatic patients with teratozoospermia. Cent. Eur. J. Immunol. 2021, 46, 76–81. [Google Scholar] [CrossRef]
- Segnini, A.; Camejo, M.I.; Proverbio, F. Chlamydia trachomatis and sperm lipid peroxidation in infertile men. Asian J. Androl. 2003, 5, 47–49. [Google Scholar]
- Weidner, W.; Pilatz, A.; Schuppe, H.C.; Rusz, A.; Wagenlehner, F. Male urogenital infections: Impact of infection and inflammation on ejaculate parameters. World J. Urol. 2013, 31, 717–723. [Google Scholar] [CrossRef]
- Agarwal, A.; Rana, M.; Qiu, E.; AlBunni, H.; Bui, A.D.; Henkel, R. Role of oxidative stress, infection and inflammation in male infertility. Andrologia 2018, 50, e13126. [Google Scholar] [CrossRef]
- Wagner, H.; Cheng, J.W.; Ko, E.Y. Role of reactive oxygen species in male infertility: An updated review of literature. Arab. J. Urol. 2017, 16, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Parekh, N.; Selvam, M.K.P.; Henkel, R.; Shah, R.; Homa, S.T.; Ramasamy, R.; Edmund, K.; Tremellen, K.; Esteves, S.; et al. Male oxidative stress infertility (MOSI): Proposed terminology and clinical practice guidelines for management of idiopathic male infertility. World J. Men’s Health 2019, 37, 296–312. [Google Scholar] [CrossRef]
- World Health Organization. Who Laboratory Manual for the Examination and Processing of Human Semen. V.; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Manos, M.M.; Ting, Y.; Wright, D.K.; Lewis, A.J.; Broker, T.R.; Wolinsky, S.M. Use of polymerase chain reaction amplification for the detection of genital human papillomaviruses. Cancer Cells 1989, 7, 209–214. [Google Scholar]
- Mahony, J.B.; Luinstra, K.E.; Sellors, J.W.; Jang, D.; Chernesky, M.A. Confirmatory polymerase chain reaction testing for Chlamydia trachomatis in first-void urine from asymptomatic and symptomatic men. J. Clin. Microbiol. 1992, 30, 2241–2245. [Google Scholar] [CrossRef] [Green Version]
- Layali, I.; Tahmasbpour, E.; Joulaei, M.; Jorsaraei, S.G.; Farzanegi, P. Total antioxidant capacity and lipid peroxidation in semen of patient with hyperviscosity. Cell J. 2015, 16, 554–559. [Google Scholar] [CrossRef]
- Benzie, I.F. An automated, specific, spectrophotometric method for measuring ascorbic acid in plasma (EFTSA). Clin. Biochem. 1996, 29, 111–116. [Google Scholar] [CrossRef]
- Nasseri, S.; Monavari, S.H.; Keyvani, H.; Nikkhoo, B.; Roudsari, R.V.; Khazeni, M. The prevalence of Human Papilloma Virus (HPV) infection in the oligospermic and azoospermic men. Med. J. Islamic Repub. Iran 2015, 29, 272. [Google Scholar]
- Lajous, M.; Mueller, N.; Cruz-Valdéz, A.; Aguilar, L.V.; Franceschi, S.; Hernández-Ávila, M.; Lazcano-Ponce, E. Determinants of prevalence, acquisition, and persistence of human papillomavirus in healthy Mexican military men. Cancer Epidemiol. Biomarker. Prev. 2005, 14, 1710–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed-Maldonado, A.B.; Madden, K.C. Infertility and the Military Male. In Seminars in Reproductive Medicine; Thieme Medical Publishers: New York, NY, USA, 2019; Volume 37, pp. 5–11. [Google Scholar] [CrossRef]
- Gimenes, F.; Medina, F.S.; De Abreu, A.L.P.; Irie, M.M.T.; Esquicati, I.B.; Malagutti, N.; Vasconcellos, V.R.B.; Discacciati, M.G.; Bonini, M.G.; Maria-Engler, S.S.; et al. Sensitive simultaneous detection of seven sexually transmitted agents in semen by multiplex-PCR and of HPV by single PCR. PLoS ONE 2014, 9, e98862. [Google Scholar] [CrossRef] [PubMed]
- Medel-Flores, O.; Valenzuela-Rodríguez, V.A.; Ocadiz-Delgado, R.; Castro-Muñoz, L.J.; Hernández-Leyva, S.; Lara-Hernández, G.; Silva-Escobedo, J.G.; Gariglio-Vidal, P.; Sánchez-Monroy, V. Association between HPV infection and prostate cancer in a Mexican population. Genet. Mol. Biol. 2018, 41, 781–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baud, D.; Pattaroni, C.; Vulliemoz, N.; Castella, V.; Marsland, B.J.; Stojanov, M. Sperm Microbiota and Its Impact on Semen Parameters. Front. Microbiol. 2019, 10, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraczek, M.; Kurpisz, M. Cytokines in the male reproductive tract and their role in infertility disorders. J. Reprod. Immunol. 2015, 108, 98–104. [Google Scholar] [CrossRef]
- Papadimas, J.; Goulis, D.G.; Sotiriades, A.; Daniilidis, M.; Fleva, A.; Bontis, J.N.; Tourkantonis, A. Interleukin-1 Beta and Tumor Necrosis Factor-alpha in normal/ infertile men. J. Reprod. Syst. 2009, 48, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Hosen, M.B.; Islam, M.R.; Begum, F.; Kabir, Y.; Howlader, M.Z.H. Oxidative stress induced sperm DNA damage, a possible reason for male infertility. Iran. J. Reprod. Med. 2015, 13, 525–532. [Google Scholar] [PubMed]
- Gholinezhad, M.; Aliarab, A.; Abbaszadeh-Goudarzi, G.; Yousefnia-Pasha, Y.; Samadaian, N.; Rasolpour-Roshan, K.; Aghagolzadeh-Haji, H.; Mohammadoo-Khorasani, M. Nitric oxide, 8-hydroxydeoxyguanosine, and total antioxidant capacity in human seminal plasma of infertile men and their relationship with sperm parameters. Clin. Exp. Reprod. Med. 2020, 47, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.H.; Mirsalehian, A.; Sadighi, G.M.A.; Bahador, A.; Afraz, K. Association of asymptomatic Chlamydia trachomatis infection with male infertility and the effect of antibiotic therapy in improvement of semen quality in infected infertile men. Andrologia 2018, 50, e12944. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.; Liu, B.J.; Wang, S.Q.; Xu, Y.; Han, P.; Li, P.C.; Wang, Z.J.; Song, N.H.; Zhang, W.; Yin, C.J. The role of mitochondrial aconitate (ACO2) in human sperm motility. Syst. Biol. Reprod. Med. 2014, 60, 251–256. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Parameter | HPV 1 | CT 2 | HPV + CT 3 | p | Normal Range |
|---|---|---|---|---|---|
| N (frequency) | 55/81 (68%) | 11/81 (13.5%) | 15/81 (18.5%) | ||
| Age (years) † | 31.40 ± 5.84 | 30.27 ± 4.07 | 33.38 ± 4.13 | >0.05 | |
| Volume (mL) † | 3.29 ± 1.34 a | 2.19 ± 1.35 | 3.22 ± 0.96 | <0.05 | (1.5–5 mL) |
| pH ‡ | 8 (7.00–8.00) | 8 (7.5–8.00) | 8.00 (8.00–8.00) | (7.2–7.8) | |
| Total sperm number (million/ejaculate) ‡ | 93.00 (46.00–156.00) | 56.00 (32.80–148.00) | 77.00 (49.00–134.00) | >0.05 | (>39) |
| Sperm count per mL (million/mL) ‡ | 24 (15.00–52.00) | 44.00 (15.30–97.00) | 25.00 (16.00–48.00) | >0.05 | (>15 million/mL) |
| Normal sperm morphology (%) † | 2.27 ± 1.42 a | 5.64 ± 2.87 | 2.67 ± 2.58 c | <0.05 | (≥4%) |
| Abnormal sperm morphology (%) † | 97.73 ± 1.42 a | 94.36 ± 2.87 | 97.33 ± 2.58 c | <0.05 | |
| Head defects (%) † | 41.95 ± 8.70 | 43.82 ± 12.40 | 47.33 ± 13.71 | >0.05 | |
| Midpiece defects (%) † | 25.82 ± 8.34 | 24.00 ± 13.19 | 23.27 ± 4.49 | >0.05 | |
| Tail defects (%) † | 30.00 ± 12.19 | 26.27 ± 19.12 | 23.20 ± 14.30 | >0.05 | |
| Total progressive motility (% A + B) † | 43.87 ± 20.00 | 45.00 ± 22.50 | 47.33 ± 18.45 | >0.05 | (≥32%) |
| Fast progressive motility (% A) † | 5.96 ± 14.84 | 34.17 ± 28.29 | 2.00 ± 1.34 c | <0.05 | |
| Low progressive motility (% B) † | 38 ± 18.61 a | 10.83 ± 23.22 | 45.33 ± 17.44 c | <0.05 | |
| Leukocytes (million) ‡ | 0.8 (0.350–1.70) | 0.42 (0.110–1.48) | 0.700 (0.300–1.070) | >0.05 | (≤1 million) |
| Variable | HPV 1 | CT 2 | HPV + CT 3 | p |
|---|---|---|---|---|
| IFN-γ (pg/mL) ‡ | 524.25 (226.45–764.62) a | ND | 141.50 (39.00–911.90) c | <0.05 |
| IL-1β (pg/mL) ‡ | 141.33 (0–337.68) a | 0.000 (0–1.33) | 328.00 (141.33–1303.00) b, c | <0.05 |
| IL-6 (pg/mL) ‡ | 203.30 (0.400–203.33) a | ND | 190.80 (36.8–271.80) c | <0.05 |
| LPO (nmol MDA/mg protein) ‡ | 9.00 (7.04–12.23) a | 4.21 (2.42–4.34) | 7.45 (4.91–10.70) c | <0.05 |
| 8-OHdG (ng/mL) * | 8.29 (8.04–8.68) a | 1.9 (1.85–5.05) | 8.20 (7.85–8.92) | <0.05 |
| TAC (µmol/L) † | 590.05 ± 401.11 a | 1086.91 ± 273.57 | 713.44 ± 481.11 c | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Soto, E.; Fernández-Martínez, E.; Oros-Pantoja, R.; Medel-Flores, O.; Miranda-Covarrubias, J.C.; Sánchez-Monroy, V. Proinflammatory and Oxidative Stress States Induced by Human Papillomavirus and Chlamydia trachomatis Coinfection Affect Sperm Quality in Asymptomatic Infertile Men. Medicina 2021, 57, 862. https://doi.org/10.3390/medicina57090862
Pérez-Soto E, Fernández-Martínez E, Oros-Pantoja R, Medel-Flores O, Miranda-Covarrubias JC, Sánchez-Monroy V. Proinflammatory and Oxidative Stress States Induced by Human Papillomavirus and Chlamydia trachomatis Coinfection Affect Sperm Quality in Asymptomatic Infertile Men. Medicina. 2021; 57(9):862. https://doi.org/10.3390/medicina57090862
Chicago/Turabian StylePérez-Soto, Elvia, Eduardo Fernández-Martínez, Rigoberto Oros-Pantoja, Olivia Medel-Flores, José Cruz Miranda-Covarrubias, and Virginia Sánchez-Monroy. 2021. "Proinflammatory and Oxidative Stress States Induced by Human Papillomavirus and Chlamydia trachomatis Coinfection Affect Sperm Quality in Asymptomatic Infertile Men" Medicina 57, no. 9: 862. https://doi.org/10.3390/medicina57090862