
Tension Hemothorax in Aortic Rupture: A Case Report

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
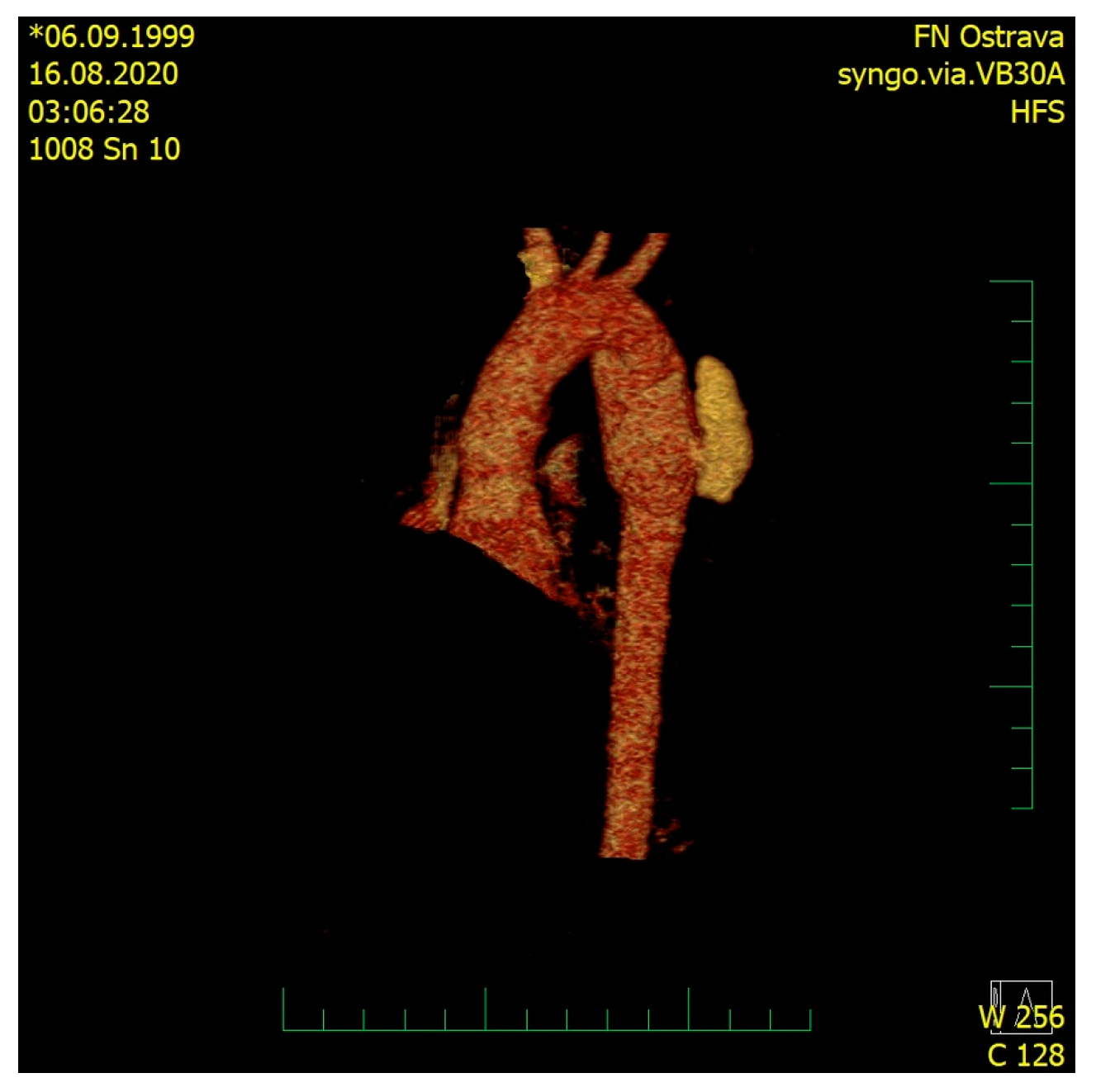
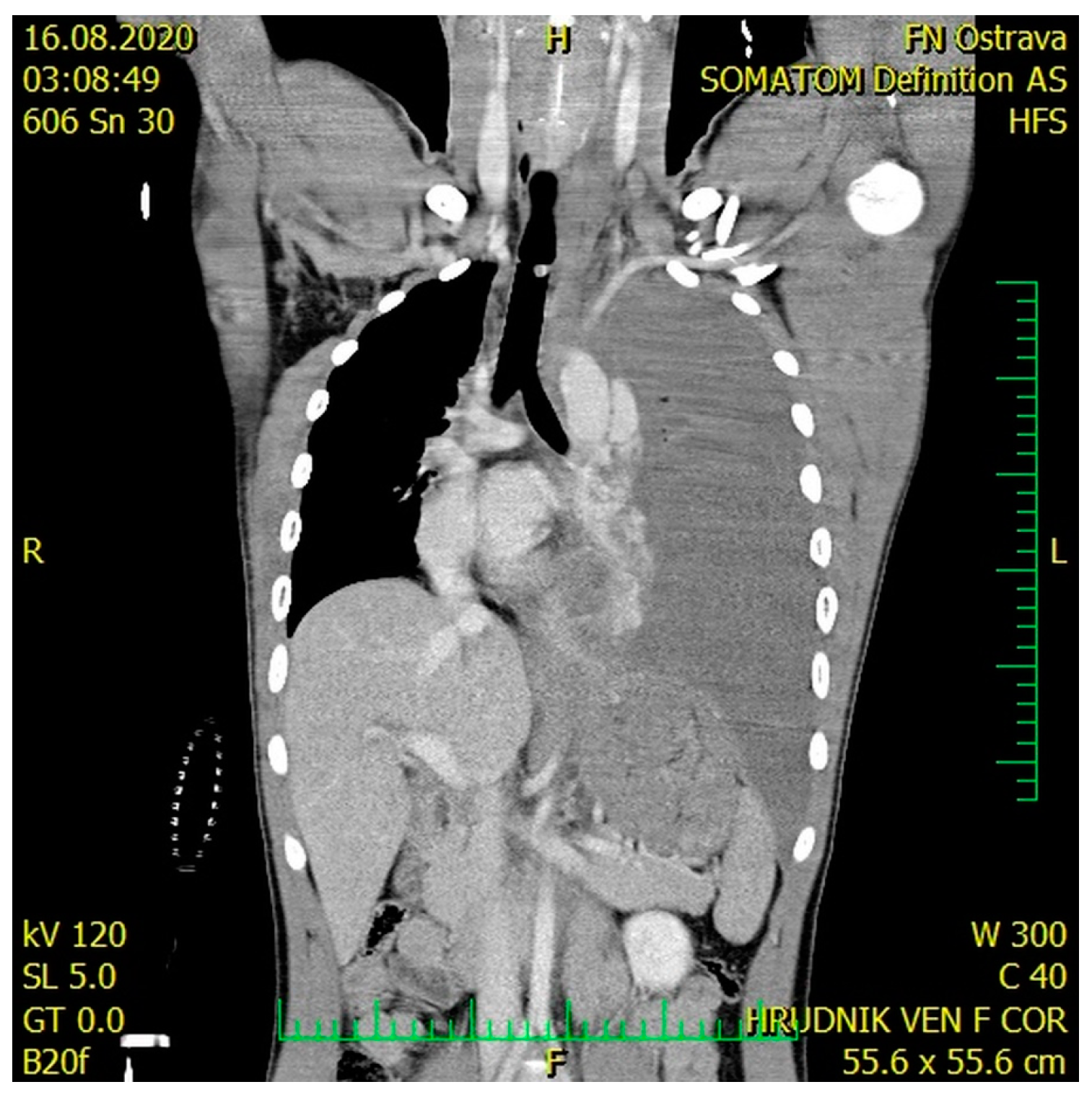
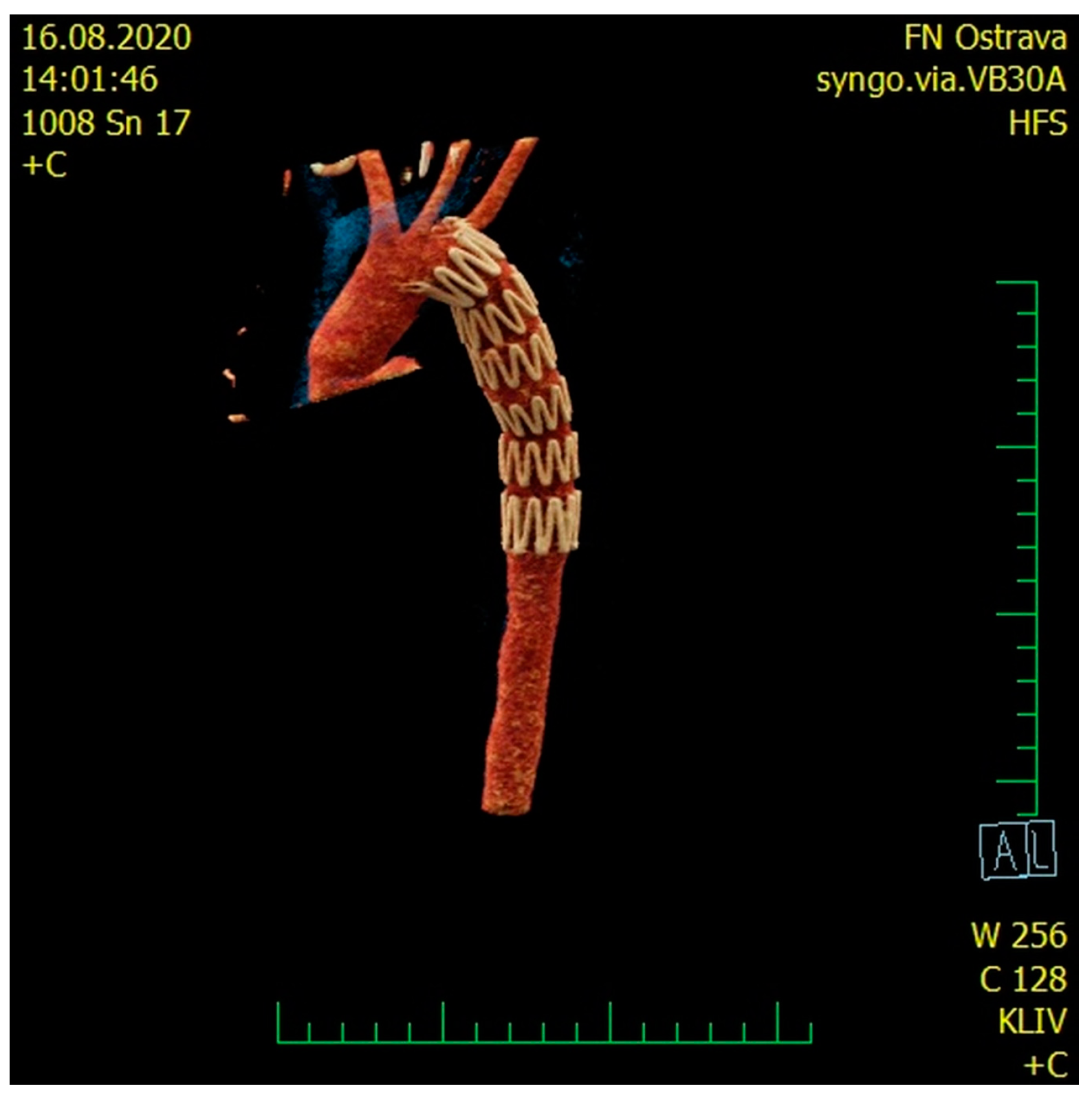
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Buczkowski, P.; Puślecki, M.; Stefaniak, S.; Juszkat, R.; Kulesza, J.; Perek, B.; Misterski, M.; Urbanowicz, T.; Ligowski, M.; Zabicki, B.; et al. Post-traumatic acute thoracic aortic injury (TAI)—a single center experience. J. Thorac. Dis. 2017, 9, 4477–4485. [Google Scholar] [CrossRef] [Green Version]
- Ungar, T.C.; Wolf, S.J.; Haukoos, J.S.; Dyer, D.S.; Moore, E.E. Derivation of a Clinical Decision Rule to Exclude Thoracic Aortic Imaging in Patients With Blunt Chest Trauma After Motor Vehicle Collisions. J. Trauma Inj. Infect. Crit. Care 2006, 61, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, H.; Dambrin, C.; Marcheix, B.; Richeux, L.; Mazerolles, M.; Cron, C.; Watkinson, A.; Mugniot, A.; Soula, P.; Chabbert, V.; et al. Acute traumatic aortic rupture: A comparison of surgical and stent-graft repair. J. Thorac. Cardiovasc. Surg. 2005, 129, 1050–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parmley, L.F.; Mattingly, T.W.; Manion, W.C.; Jahnke, E.J., Jr. Nonpenetrating Traumatic Injury of the Aorta. Circulation 1958, 17, 1086–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, J.S.; Graff, J.A.; Uku, J.M.; Steinig, J.P. Aortic injury in vehicular trauma. Ann. Thorac. Surg. 1994, 57, 726–730. [Google Scholar] [CrossRef]
- Vyhnánek, F.H.J. Thoracic trauma as cause of the death in bblunt injuries. Úrazová Chir. 2013, 21, 95–98. [Google Scholar]
- Greendyke, R.M. Traumatic rupture of aorta; special reference to automobile accidents. JAMA 1966, 195, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Brüls, S.; Goffin, P.; Sakalihasan, N.; Bonnet, P.; Defraigne, J.O. Traumatic rupture of the aortic isthmus: Modern perspectives. Rev. Medicale Liege 2015, 70, 415–422. [Google Scholar]
- Fabian, T.C.; Richardson, J.D.; Croce, M.A.; Smith, J.S., Jr.; Rodman, G., Jr.; Kearney, P.A.; Flynn, W.; Ney, A.L.; Cone, J.B.; Luchette, F.A.; et al. Prospective study of blunt aortic injury: Multicenter Trial of the American Association for the Surgery of Trauma. J. Trauma 1997, 42, 374–380. [Google Scholar] [CrossRef]
- Merrill, W.H.; Lee, R.B.; Hammon, J.W., Jr.; Frist, W.H.; Stewart, J.R.; Bender, H.W., Jr. Surgical Treatment of Acute Traumatic Tear of the Thoracic Aorta. Ann. Surg. 1988, 207, 699–706. [Google Scholar] [CrossRef]
- Treska, V.; Slauf, F.; Certik, B.; Sulc, R.; Cechura, M.; Molacek, J.; Hajek, T.; Houdek, K. Traumatic rupture of thoracic aorta. Rozhl. Chir. 2012, 91, 535–538. [Google Scholar] [PubMed]
- Avery, J.E.; Hall, D.P.; Adams, J.E.; Headrick, J.R.; Nipp, R.E. Traumatic Rupture of the Thoracic Aorta. South. Med. J. 1979, 72, 1238–1240. [Google Scholar] [CrossRef] [PubMed]
- Richens, D.; Field, M.; Neale, M.; Oakley, C. The mechanism of injury in blunt traumatic rupture of the aorta. Eur. J. Cardio Thorac. Surg. 2002, 21, 288–293. [Google Scholar] [CrossRef]
- Fattori, R.; Russo, V.; Lovato, L.; Di Bartolomeo, R. Optimal Management of Traumatic Aortic Injury. Eur. J. Vasc. Endovasc. Surg. 2009, 37, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.S.; Chang, F.C. Traumatic rupture of the aorta: Still a lethal injury. Am. J. Surg. 1986, 152, 660–663. [Google Scholar] [CrossRef]
- Nagpal, P.; Mullan, B.F.; Sen, I.; Saboo, S.S.; Khandelwal, A. Advances in Imaging and Management Trends of Traumatic Aortic Injuries. Cardiovasc. Interv. Radiol. 2017, 40, 643–654. [Google Scholar] [CrossRef]
- O’Conor, C. Diagnosing traumatic rupture of the thoracic aorta in the emergency department. Emerg. Med. J. 2004, 21, 414–419. [Google Scholar]
- Coermann, R.; Dotzauer, G.; Lange, W.; Voigt, G.E. The effects of the design of the steering assembly and the instrument panel on injuries (especially aortic rupture) sustained by car drivers in head-on collision. J. Trauma Inj. Infect. Crit. Care 1972, 12, 715–724. [Google Scholar] [CrossRef]
- Lundevall, J. Traumatic Rupture of the Aorta, with Special Reference to Road Accidents. Acta. Pathol. Microbiol. Scand. 1964, 62, 29–33. [Google Scholar] [CrossRef]
- Ayella, R.J.; Hankins, J.R.; Turney, S.Z.; Cowley, R.A. Ruptured thoracic aorta due to blunt trauma. J. Trauma 1977, 17, 199–205. [Google Scholar] [CrossRef]
- Symbas, P.N.; Sherman, A.J.; Silver, J.M.; Symbas, J.D.; Lackey, J.J. Traumatic rupture of the aorta: Immediate or delayed repair? Ann. Surg. 2002, 235, 796–802. [Google Scholar] [CrossRef]
- von Oppell, U.O.; Dunne, T.T.; De Groot, M.K.; Zilla, P. Traumatic aortic rupture: Twenty-year metaanalysis of mortality and risk of paraplegia. Ann. Thorac. Surg. 1994, 58, 585–593. [Google Scholar] [CrossRef]
- Verdant, A. Contemporary results of standard open repair of acute traumatic rupture of the thoracic aorta. J. Vasc. Surg. 2010, 51, 294–298. [Google Scholar] [CrossRef] [Green Version]
- Pate, J.W.; Fabian, T.C.; Walker, W. Traumatic rupture of the aortic isthmus: An emergency? World J. Surg. 1995, 19, 119–125. [Google Scholar] [CrossRef]
- Schumacher, H.; Böckler, D.; Von Tengg-Kobligk, H.; Allenberg, J.-R. Acute Traumatic Aortic Tear: Open Versus Stent-graft Repair. Semin. Vasc. Surg. 2006, 19, 48–59. [Google Scholar] [CrossRef]
- Buz, S.; Zipfel, B.; Mulahasanovic, S.; Pasic, M.; Weng, Y.; Hetzer, R. Conventional surgical repair and endovascular treatment of acute traumatic aortic rupture. Eur. J. Cardio-Thoracic Surg. 2008, 33, 143–149. [Google Scholar] [CrossRef]
- Watson, J.; Slaiby, J.; Toca, M.G.; Marcaccio, E.J., Jr.; Chong, T.T. A 14-year experience with blunt thoracic aortic injury. J. Vasc. Surg. 2013, 58, 380–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, G.L.; Tehrani, H.Y.; Usman, A.; Katariya, K.; Otero, C.; Perez, E.; Eskandari, M.K. Reduced mortality, paraplegia, and stroke with stent graft repair of blunt aortic transections: A modern meta-analysis. J. Vasc. Surg. 2008, 47, 671–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, H.M. Chest tube care in critically ill patient: A comprehensive review. Egypt. J. Chest Dis. Tuberc. 2015, 64, 849–855. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pometlová, J.; Madeja, R.; Demel, J.; Ječmínková, R.; Procházka, V.; Kitka, M.; Pleva, L. Tension Hemothorax in Aortic Rupture: A Case Report. Medicina 2021, 57, 790. https://doi.org/10.3390/medicina57080790
Pometlová J, Madeja R, Demel J, Ječmínková R, Procházka V, Kitka M, Pleva L. Tension Hemothorax in Aortic Rupture: A Case Report. Medicina. 2021; 57(8):790. https://doi.org/10.3390/medicina57080790
Chicago/Turabian StylePometlová, Jana, Roman Madeja, Jiří Demel, Renata Ječmínková, Václav Procházka, Miroslav Kitka, and Leopold Pleva. 2021. "Tension Hemothorax in Aortic Rupture: A Case Report" Medicina 57, no. 8: 790. https://doi.org/10.3390/medicina57080790