
WNT-5a and SOST Levels in Gingival Crevicular Fluid Depend on the Inflammatory and Osteoclastogenic Activities of Periodontal Tissues


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Study Groups
2.4. Clinical Examination
2.5. Sample Collection
2.6. Laboratory Analysis
2.7. Sample Size Calculation
2.8. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinical Findings
3.2. Clinical Characteristics of Sampled Sites
3.3. Total Protein Amounts of Periodontitis, Gingivitis and Healthy Sites
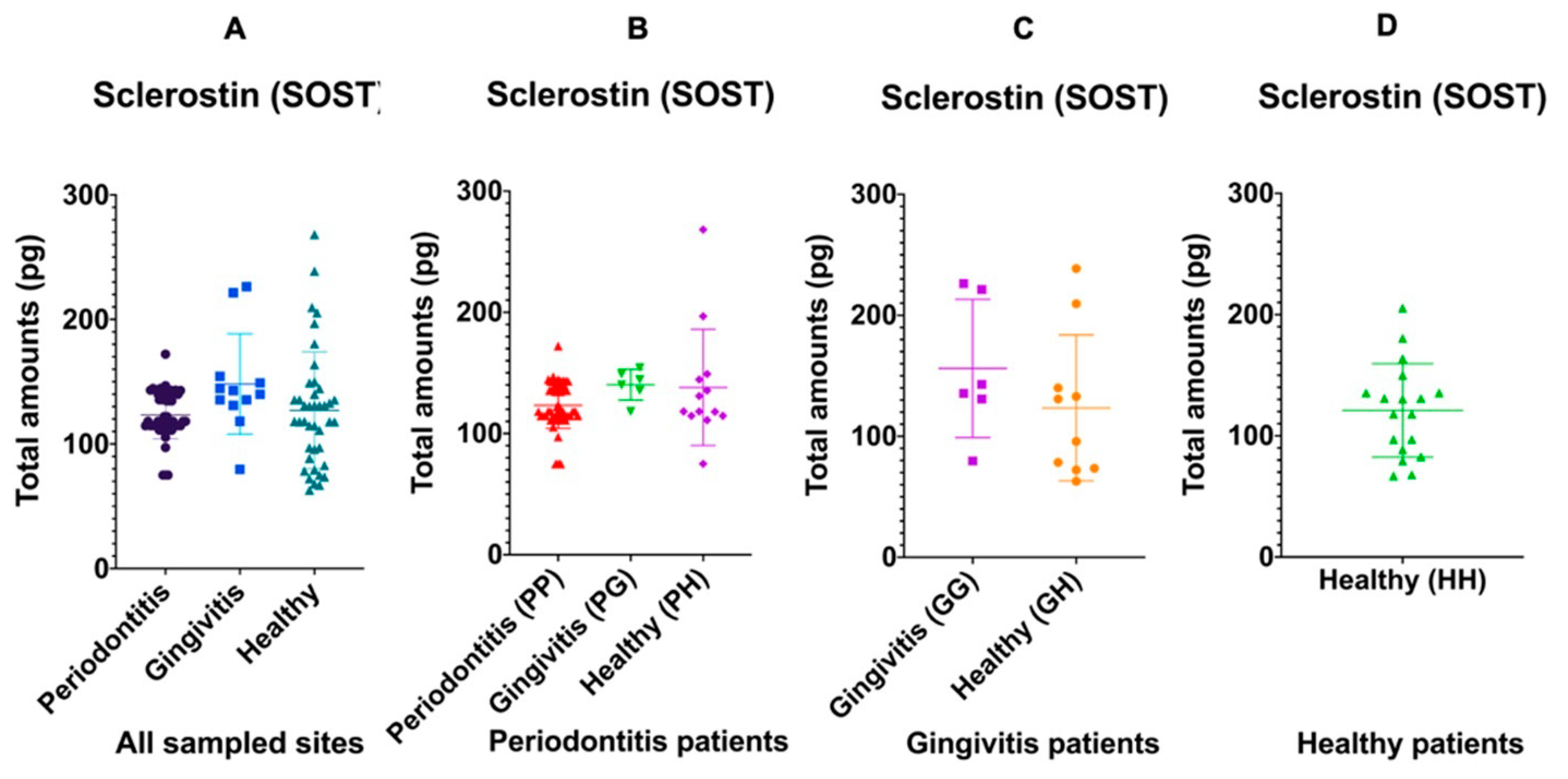
3.3.1. Sclerostin Is Osteoclastogenic but Dampens Osteoblasts
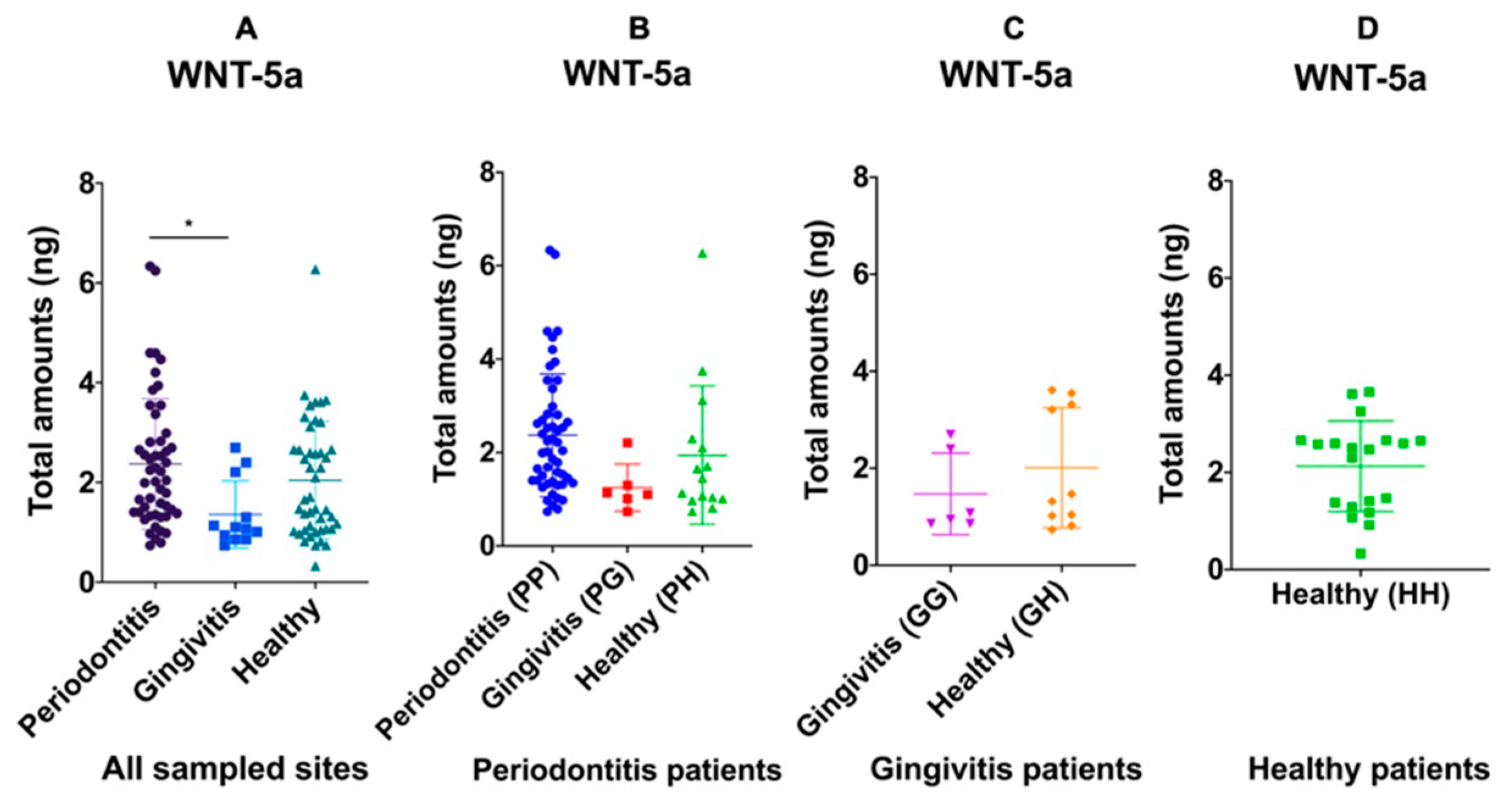
3.3.2. WNT-5a Could Be Both: Osteoclastogenic and Pro-Osteoblastic
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef]
- Costalonga, M.; Herzberg, M.C. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol. Lett. 2014, 162, 22–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims, N.A.; Martin, T.J. Coupling the activities of bone formation and resorption: A multitude of signals within the basic multicellular unit. Bonekey Rep. 2014, 3, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enzo, M.V.; Rastrelli, M.; Rossi, C.R.; Hladnik, U.; Segat, D. The Wnt/β-catenin pathway in human fibrotic-like diseases and its eligibility as a therapeutic target. Mol. Cell. Ther. 2015, 3, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, V.; Bryant, H.U.; Macdougald, O.A. Regulation of bone mass by Wnt signaling. J. Clin. Invest. 2006, 116, 1202–1209. [Google Scholar] [CrossRef]
- Komiya, Y.; Habas, R. Wnt signal transduction pathways. Organogenesis 2008, 4, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Rossini, M.; Gatti, D.; Adami, S. Involvement of WNT/β-catenin signaling in the treatment of osteoporosis. Calcif. Tissue Int. 2013, 93, 121–132. [Google Scholar] [CrossRef]
- Poole, K.E.; van Bezooijen, R.L.; Loveridge, N.; Hamersma, H.; Papapoulos, S.E.; Lowik, C.W.; Reeve, J. Sclerostin is a delayed secreted product of osteocytes that inhibits bone formation. FASEB J. 2005, 19, 1842–1844. [Google Scholar] [CrossRef] [Green Version]
- Wijenayaka, A.R.; Kogawa, M.; Lim, H.P.; Bonewald, L.F.; Findlay, D.M.; Atkins, G.J. Sclerostin stimulates osteocyte support of osteoclast activity by a RANKL-dependent pathway. PLoS ONE 2011, 6, e25900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewiecki, E.M.; Dinavahi, R.V.; Lazaretti-Castro, M.; Ebeling, P.R.; Adachi, J.D.; Miyauchi, A.; Gielen, E.; Milmont, C.E.; Libanati, C.; Ggrauer, A. One year of romosozumab followed by two years of denosumab maintains fracture risk reductions: Results of the FRAME extension study. J. Bone Miner. Res. 2019, 34, 419–428. [Google Scholar] [CrossRef]
- Taut, A.D.; Jin, Q.; Chung, J.H.; Galindo-Moreno, P.; Yi, E.S.; Sugai, J.V.; Ke, H.Z.; Liu, M.; Giannobile, W.V. Sclerostin antibody stimulates bone regeneration after experimental periodontitis. J. Bone Miner. Res. 2013, 28, 2347–2356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Zhang, C.; Huang, Y.; Yu, Y.; Li, R.; Li, M.; Liu, N.; Liu, P.; Qiao, J. Up-regulated expression of WNT5a increases inflammation and oxidative stress via PI3K/AKT/NF-κB signaling in the granulosa cells of PCOS patients. J. Clin. Endocrinol. Metab. 2015, 100, 201–211. [Google Scholar] [CrossRef]
- Pashirzad, M.; Shafiee, M.; Rahmani, F.; Behnam-Rassouli, R.; Hoseinkhani, F.; Ryzhikov, M.; Binabaj, M.M.; Parizadeh, M.R.; Avan, A.; Hassanian, S.M. Role of Wnt5a in the pathogenesis of inflammatory diseases. J. Cell. Physiol. 2017, 232, 1611–1616. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Kobayashi, Y.; Udagawa, N.; Uehara, S.; Ishihara, A.; Mizoguchi, T.; Kikuchi, Y.; Takada, I.; Kato, S.; Kani, S.; et al. Wnt5a-Ror2 signaling between osteoblast-lineage cells and osteoclast precursors enhances osteoclastogenesis. Nat. Med. 2012, 18, 405–412. [Google Scholar] [CrossRef]
- Okamoto, M.; Udagawa, N.; Uehara, S.; Maeda, K.; Yamashita, T.; Nakamichi, Y.; Kato, H.; Saito, N.; Minami, Y.; Takahashi, N.; et al. Noncanonical Wnt5a enhances Wnt/β-catenin signaling during osteoblastogenesis. Sci. Rep. 2014, 4, 4493. [Google Scholar] [CrossRef] [Green Version]
- Leris, A.; Roberts, T.; Jiang, W.; Newbold, R.; Mokbel, K. WNT5A expression in human breast cancer. Anticancer. Res. 2005, 25, 731–734. [Google Scholar]
- Slots, J. Periodontology: Past, present, perspectives. Periodontology 2000 2013, 62, 7–19. [Google Scholar] [CrossRef]
- Barros, S.P.; Williams, R.; Offenbacher, S.; Morelli, T. Gingival crevicular fluid as a source of biomarkers for periodontitis. Periodontology 2000 2016, 70, 53–64. [Google Scholar] [CrossRef]
- Buduneli, N.; Kinane, D.F. Host-derived diagnostic markers related to soft tissue destruction and bone degradation in periodontitis. J. Clin. Periodontol. 2011, 38 (Suppl. 11), 85–105. [Google Scholar] [CrossRef]
- Uitto, V.J.; Overall, C.M.; McCulloch, C. Proteolytic host cell enzymes in gingival crevice fluid. Periodontology 2000 2003, 31, 77–104. [Google Scholar] [CrossRef]
- Ueda, M.; Kuroishi, K.N.; Gunjigake, K.K.; Ikeda, E.; Kawamoto, T. Expression of SOST/sclerostin in compressed periodontal ligament cells. J. Dent. Sci. 2016, 11, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, D.; Wada, N.; Maeda, H.; Yoshida, S.; Mitarai, H.; Tomokiyo, A.; Monnouchi, S.; Hamano, S.; Yuda, A.; Akamine, A. Wnt5a Induces Collagen Production by Human Periodontal Ligament Cells Through TGFβ1-Mediated Upregulation of Periostin Expression. J. Cell. Physiol. 2015, 230, 2647–2660. [Google Scholar] [CrossRef]
- Chatzopoulos, G.S.; Mansky, K.C.; Lunos, S.; Costalonga, M.; Wolff, L.F. Sclerostin and WNT-5a gingival protein levels in chronic periodontitis and health. J. Periodont. Res. 2019, 54, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Development of classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. 1), S46–S73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Best, A.M.; Burmeister, J.A.; Gunsolley, J.C.; Brooks, C.N.; Schenkein, H.A. Reliability of attachment loss measurements in a longitudinal clinical trial. J. Clin. Periodontol. 1990, 17, 564–569. [Google Scholar] [CrossRef]
- Polson, A.M. The research team, calibration, and quality assurance in clinical trials in periodontics. Ann. Periodontol. 1997, 2, 75–82. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Graziani, F.; Herrera, D.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S162–S170. [Google Scholar] [CrossRef]
- Loos, B.G.; Tjoa, S. Host-derived diagnostic markers for periodontitis: Do they exist in gingival crevice fluid? Periodontology 2005, 39, 53–72. [Google Scholar] [CrossRef]
- Lamster, I.B. Evaluation of components of gingival crevicular fluid as diagnostic tests. Ann. Periodontol. 1997, 2, 123–137. [Google Scholar] [CrossRef]
- Goodson, J.M. Gingival crevice fluid flow. Periodontology 2000 2003, 31, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, D.E.; Cha, J.H.; Bak, E.J.; Yoo, Y.J. Receptor activator of nuclear factor-κB ligand and sclerostin expression in osteocytes of alveolar bone in rats with ligature-induced periodontitis. J. Periodontol. 2014, 85, e370–e378. [Google Scholar] [CrossRef]
- Kuchler, U.; Schwarze, U.Y.; Dobsak, T.; Heimel, P.; Bosshardt, D.D.; Kneissel, M.; Gruber, R. Dental and periodontal phenotype in sclerostin knockout mice. Int. J. Oral Sci. 2014, 6, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Napimoga, M.H.; Nametala, C.; da Silva, F.L.; Miranda, T.S.; Bossonaro, J.P.; Demasi, A.P.D.; Duarte, P.M. Involvement of the Wnt-β-catenin signalling antagonists, sclerostin and dickkopf-related protein 1, in chronic periodontitis. J. Clin. Periodontol. 2014, 41, 550–557. [Google Scholar] [CrossRef]
- Balli, U.; Aydogdu, A.; Dede, F.O.; Turer, C.C.; Guven, B. Gingival Crevicular Fluid Levels of Sclerostin, Osteoprotegerin, and Receptor Activator of Nuclear Factor-κB Ligand in Periodontitis. J. Periodontol. 2015, 86, 1396–1404. [Google Scholar] [CrossRef] [PubMed]
- Esfahrood, Z.R.; Yadegari, Z.; Veysari, S.K.; Kadkhodazadeh, M. Gingival crevicular fluid levels of sclerostin in chronic periodontitis and healthy subjects. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 289–292. [Google Scholar] [CrossRef] [Green Version]
- Beiler, T.F.C.S.B.; de Mello Neto, J.M.; Alves, J.C.; Hamlet, S.; Ipe, D.; da Silva Figueredo, C.M. Impact of non-surgical periodontal treatment on salivary expression of cytokines related to bone metabolism. Odontology 2020, 108, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Yakar, N.; Guncu, G.N.; Akman, A.C.; Pınar, A.; Karabulut, E.; Nohutcu, R.M. Evaluation of gingival crevicular fluid and peri-implant crevicular fluid levels of sclerostin, TWEAK, RANKL and OPG. Cytokine 2019, 113, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Katoh, M.; Katoh, M. STAT3-induced WNT5A signaling loop in embryonic stem cells, adult normal tissues, chronic persistent inflammation, rheumatoid arthritis and cancer (Review). Int. J. Mol. Med. 2007, 19, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Malgor, R.; Bhatt, P.M.; Connolly, B.A.; Jacoby, D.L.; Feldmann, K.J.; Silver, M.J.; Nazawa, M.; McCall, K.D.; Goetz, D.J. Wnt5a, TLR2 and TLR4 are elevated in advanced human atherosclerotic lesions. Inflamm. Res. 2014, 63, 277–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanbara, H.; Wara-Aswapati, N.; Nagasawa, T.; Yoshida, Y.; Yashiro, R.; Bando, Y.; Kobayashi, H.; Khongcharoensuk, J.; Hormdee, D.; Pitiphat, W.; et al. Modulation of Wnt5a expression by periodontopathic bacteria. PLoS ONE 2012, 7, e34434. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Liu, J.; Ma, L.; Bai, N.; Xu, H. Wnt5a is involved in LOX-1 and TLR4 induced host inflammatory response in peri-implantitis. J. Periodontal. Res. 2020, 55, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Haftcheshmeh, S.M.; Mohammadi, A.; Soltani, A.; Momtazi-Borojeni, A.A.; Sattari, M. Evaluation of STAT1 and Wnt5a gene expression in gingival tissues of patients with periodontal disease. J. Cell. Biochem. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rauner, M.; Sipos, W.; Pietschmann, P. Age-dependent Wnt gene expression in bone and during the course of osteoblast differentiation. Age 2008, 30, 273–282. [Google Scholar] [CrossRef] [Green Version]
- BinShabaib, M.; ALHarthi, S.S.; Akram, Z.; Khan, J.; Rahman, I.; Romanos, G.E.; Javed, F. Clinical periodontal status and gingival crevicular fluid cytokine profile among cigarette-smokers, electronic-cigarette users and never-smokers. Arch. Oral Biol. 2019, 102, 212–217. [Google Scholar] [CrossRef]
- Ustün, K.; Alptekin, N.O. The effect of tobacco smoking on gingival crevicular fluid volume. Eur. J. Dent. 2007, 1, 236–239. [Google Scholar]



{kind=link}
{kind=link}
| Demographic, Smoking and Clinical Characteristics | Periodontitis Group (N = 20–45.5%) | Gingivitis Group (N = 10–22.7%) | Healthy Group (N = 14–31.8%) | Total Population (N = 44–100%) | p-Value * |
|---|---|---|---|---|---|
| Age | <0.001 † | ||||
| Mean (SD) | 58.7 (13.8) | 31.6 (12.7) | 27.1 (8.4) | 42.5 (19.1) | |
| Gender | 0.21 ‡ | ||||
| Males (%) | 10 (50) | 2 (20) | 4 (28.6) | 16 (36.4) | |
| Females (%) | 10 (50) | 8 (80) | 10 (71.4) | 28 (63.6) | |
| Race | 0.13 ‡ | ||||
| Caucasians (%) | 14 (70) | 10 (100) | 11 (78.6) | 35 (79.5) | |
| African Americans (%) | 5 (25) | 0 (0) | 1 (7.1) | 6 (13.6) | |
| Asians (%) | 0 (0) | 0 (0) | 2 (14.3) | 2 (4.5) | |
| Hispanics (%) | 1 (5) | 0 (0) | 0 (0) | 1 (2.3) | |
| Smoking status | <0.001 ‡ | ||||
| Never smokers (%) | 6 (30) | 10 (100) | 14 (100) | 30 (68.2) | |
| Ex-smokers (%) | 6 (30) | 0 (0) | 0 (0) | 6 (13.6) | |
| Current smokers (%) | 8 (40) | 0 (0) | 0 (0) | 8 (18.2) | |
| Amount of smoking | 1.00 ‡ | ||||
| <10 cig/day (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| 10–20 cig/day (%) | 2 (25) | 0 (0) | 0 (0) | 2 (25) | |
| >20 cig/day (%) | 6 (75) | 0 (0) | 0 (0) | 6 (75) | |
| Missing teeth (mean ± SD) | 4.90 ± 3.71 | 0.80 ± 1.14 | 0.79 ± 1.58 | 2.66 ± 3.38 | <0.001 † |
| Full mouth (mean ± SD) | |||||
| PPD (mm) | 3.82 ± 1.20 | 2.15 ± 0.31 | 1.70 ± 0.22 | 2.77 ± 1.28 | <0.001 † |
| CAL (mm) | 3.95 ± 1.69 | 0.00 ± 0.00 | 0.00 ± 0.00 | 1.80 ± 2.28 | <0.001 † |
| BOP (%) | 45.65 ± 31.02 | 25.50 ± 18.78 | 4.21 ± 2.12 | 27.89 ± 28.82 | <0.001 † |
| PI (%) | 30.39 ± 34.33 | 4.90 ± 6.03 | 1.21 ± 2.72 | 15.31 ± 26.95 | 0.002 † |
| Sites with PPD = 1–3 mm (%) | 55.56 ± 21.45 | 95.20 ± 6.67 | 99.31 ± 0.73 | 78.49 ± 25.75 | <0.001 † |
| Sites with PPD = 4–6 mm (%) | 33.08 ± 14.55 | 4.80 ± 6.67 | 0.00 ± 0.00 | 16.13 ± 18.74 | <0.001 † |
| Sites with PPD ≥ 7 mm (%) | 10.98 ± 15.26 | 0.00 ± 0.00 | 0.00 ± 0.00 | 4.99 ± 11.55 | 0.005 † |
| Sites with CAL = 0–2 mm (%) | 33.46 ± 21.40 | 100.00 ± 0.00 | 100.00 ± 0.00 | 69.76 ± 36.41 | <0.001 † |
| Sites with CAL = 3–4 mm (%) | 32.46 ± 10.94 | 0.00 ± 0.00 | 0.00 ± 0.00 | 14.76 ± 17.89 | <0.001 † |
| Sites with CAL ≥ 5 mm (%) | 34.08 ± 24.98 | 0.00 ± 0.00 | 0.00 ± 0.00 | 15.49 ± 23.88 | <0.001 † |
| Clinical Characteristics | Periodontitis Sites (N = 51) | Gingivitis Sites (N = 12) | Healthy Sites (N = 45) | p-Value * |
|---|---|---|---|---|
| PPD (mean ± SD) | 6.41 ± 2.05 | 2.67 ± 0.49a | 2.31 ± 0.73a | <0.001 |
| CAL (mean ± SD) | 6.75 ± 2.51 | 0.92 ± 1.08a | 0.62 ± 1.50a | <0.001 |
| BOP (%) | 43 (84.3) | 12 (100.0) | 0 (0.0) | <0.001 |
| Sites with PPD = 1–3 mm (%) | 0 (0.0) † | 12 (100.0) | 45 (100.0) | <0.001 |
| Sites with PPD = 4–6 mm (%) | 31 (60.8) | 0 (0.0) | 0 (0.0) | |
| Sites with PPD ≥ 7 mm (%) | 20 (39.2) | 0 (0.0) | 0 (0.0) | |
| Sites with CAL = 0–2 mm (%) | 0 (0.0) † | 12 (100.0) | 45 (100) | <0.001 |
| Sites with CAL = 3–4 mm (%) | 8 (15.7) | 0 (0.0) | 0 (0.0) | |
| Sites with CAL ≥ 5 mm (%) | 43 (84.3) | 0 (0.0) | 0 (0.0) |
| Periodontitis Patient Group † | Gingivitis Patient Group † | Healthy Patient Group † | ||||
|---|---|---|---|---|---|---|
| Clinical Characteristics | Periodontitis Sites PP (N = 51) | Gingivitis Sites PG (N = 6) | Healthy Sites PH (N = 15) | Gingivitis Sites GG (N = 6) | Healthy Sites GH (N = 10) | Healthy Sites HH (N = 20) |
| PPD (mean ± SD) | 6.41 ± 2.05 | 2.5 ± 0.55 a | 2.47 ± 0.74 a | 2.83 ± 0.41 | 2.5 ± 0.85 | 2.10 ± 0.64 a |
| CAL (mean ± SD) | 6.75 ± 2.51 | 1.83 ± 0.75 a | 1.87 ± 2.13 a | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 a |
| BOP (%) | 43 (84.3) | 6 (100.0) | 0 (0.0) | 6 (100.0) | 0 (0.0) | 0 (0.0) |
| Sites with PPD = 1–3 mm (%) | 0 (0) | 6 (100.0) | 15 (100.0) | 6 (100.0) | 10 (100.0) | 20 (100.0) |
| Sites with PPD = 4–6 mm (%) | 31 (60.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Sites with PPD ≥ 7 mm (%) | 20 (39.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Sites with CAL = 0–2 mm (%) | 0 (0.0) | 6 (100.0) | 15 (100.0) | 6 (100.0) | 10 (100.0) | 20 (100.0) |
| Sites with CAL = 3–4 mm (%) | 8 (15.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Sites with CAL ≥ 5 mm (%) | 43 (84.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatzopoulos, G.S.; Costalonga, M.; Mansky, K.C.; Wolff, L.F. WNT-5a and SOST Levels in Gingival Crevicular Fluid Depend on the Inflammatory and Osteoclastogenic Activities of Periodontal Tissues. Medicina 2021, 57, 788. https://doi.org/10.3390/medicina57080788
Chatzopoulos GS, Costalonga M, Mansky KC, Wolff LF. WNT-5a and SOST Levels in Gingival Crevicular Fluid Depend on the Inflammatory and Osteoclastogenic Activities of Periodontal Tissues. Medicina. 2021; 57(8):788. https://doi.org/10.3390/medicina57080788
Chicago/Turabian StyleChatzopoulos, Georgios S., Massimo Costalonga, Kim C. Mansky, and Larry F. Wolff. 2021. "WNT-5a and SOST Levels in Gingival Crevicular Fluid Depend on the Inflammatory and Osteoclastogenic Activities of Periodontal Tissues" Medicina 57, no. 8: 788. https://doi.org/10.3390/medicina57080788