
Impact of Changing Surgical Strategies on Clinical Outcomes in Patients with Parotid Carcinoma: A 53-Year Single-Institution Experience

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Histopathologic Results
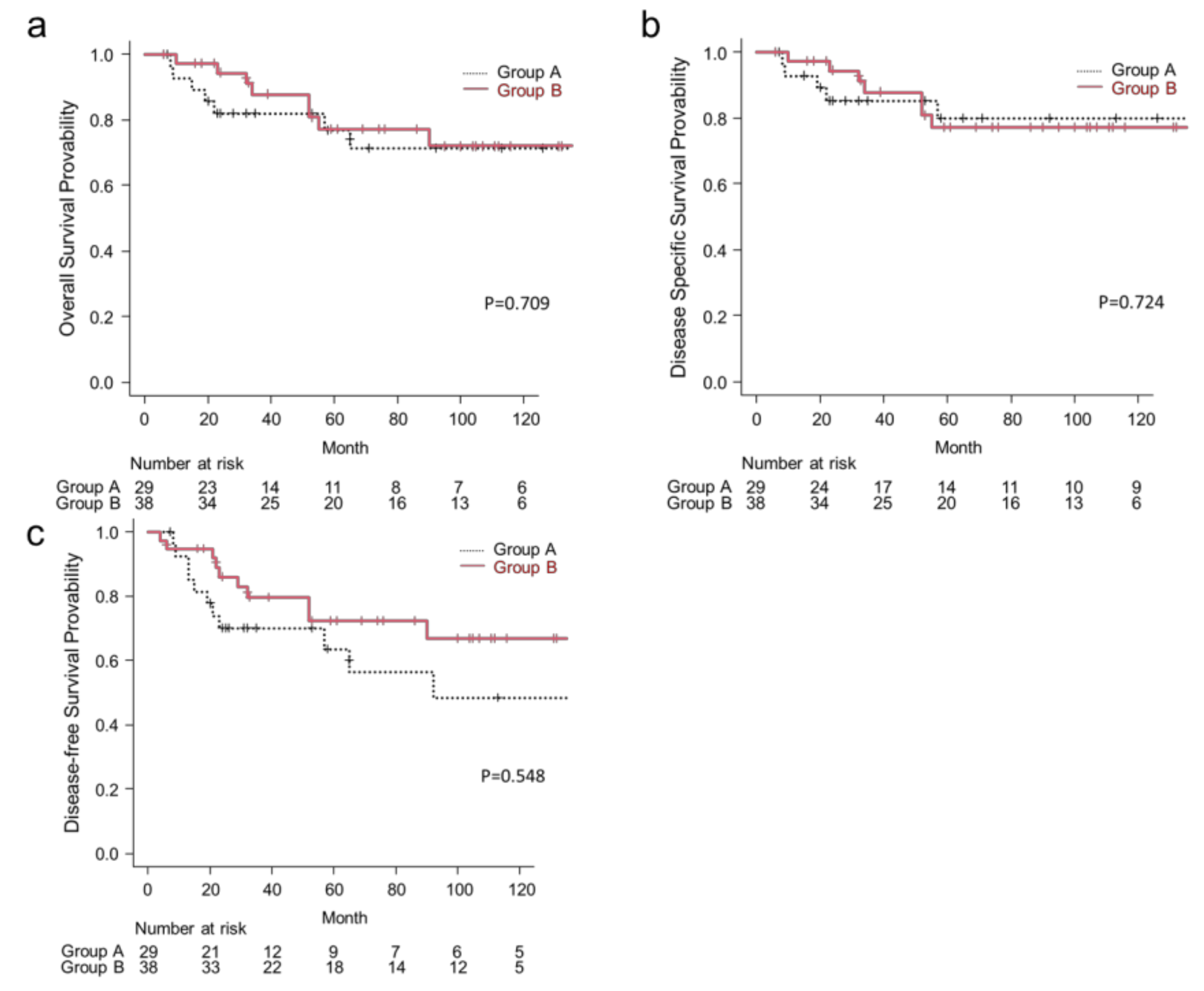
3.3. Treatment Outcomes
3.4. Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kokemueller, H.; Brueggemann, N.; Swennen, G.; Eckardt, A. Mucoepidermoid carcinoma of the salivary glands–clinical review of 42 cases. Oral. Oncol. 2005, 41, 3–10. [Google Scholar] [CrossRef]
- Hayashi, R.; Nibu, K.; Yoshimoto, S. Report of Head and Neck Cancer Registry of Japan Clinical Statics of Registered Patients, 2016; Japan Society of Head Neck Cancer: Tokyo, Japan, 2019. [Google Scholar]
- Seethala, R.R.; Stenman, G. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Tumors of the Salivary Gland. Head Neck Pathol. 2017, 11, 55–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Werning, J.W.; Villaret, D.B. Radiotherapy alone or combined with surgery for salivary gland carcinoma. Cancer 2005, 103, 2544–2550. [Google Scholar] [CrossRef]
- Catania, A.; Falvo, L.; D’Andrea, V.; Biancafarina, A.; De Stefano, M.; De Antoni, E. Parotid gland tumours. Our experience and a review of the literature. Chir Ital. 2003, 55, 857–864. [Google Scholar]
- Park, G.C.; Roh, J.L.; Cho, K.J.; Jin, M.H.; Jung, Y.G.; Lee, H.W.; Kim, T.G.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Clinically Node-Negative Parotid Gland Cancers: Prognostic Factors of Survival and Surgical Extent. Oncology 2020, 98, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.C.; Lee, S.Y.; Kim, K.; Lee, J.S.; Koo, B.S.; Shin, H.A.; Choi, E.C. Conservative parotidectomy for the treatment of parotid cancers. Oral Oncol. 2005, 41, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Magnano, M.; Gervasio, C.F.; Cravero, L.; Machetta, G.; Lerda, W.; Beltramo, G.; Orecchia, R.; Ragona, R.; Bussi, M. Treatment of malignant neoplasms of the parotid gland. Otolaryngol. Head Neck Surg. 1999, 121, 627–632. [Google Scholar] [CrossRef]
- Roh, J.L.; Kim, H.S.; Park, C.I. Randomized clinical trial comparing partial parotidectomy versus superficial or total parotidectomy. Br. J. Surg. 2007, 94, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.T.; Karnell, L.H.; Robinson, R.A.; Pinkston, J.A.; Menck, H.R. National Cancer Data Base report on cancer of the head and neck: Acinic cell carcinoma. Head Neck 1999, 21, 297–309. [Google Scholar] [CrossRef]
- Jang, J.Y.; Choi, N.; Ko, Y.H.; Chung, M.K.; Son, Y.I.; Baek, C.H.; Baek, K.H.; Jeong, H.S. Treatment outcomes in metastatic and localized high-grade salivary gland cancer: High chance of cure with surgery and post-operative radiation in T1-2 N0 high-grade salivary gland cancer. BMC Cancer 2018, 18, 672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, L.; Zhang, D.; Zhang, M.; Zhou, L. Clinical behaviours and prognoses of high- and low-risk parotid malignancies based on histology. Eur. Arch. Otorhinolaryngol. 2019, 276, 497–503. [Google Scholar] [CrossRef]
- Ali, S.; Palmer, F.L.; DiLorenzo, M.; Shah, J.P.; Patel, S.G.; Ganly, I. Treatment of the neck in carcinoma of the parotid gland. Ann. Surg. Oncol. 2014, 21, 3042–3048. [Google Scholar] [CrossRef]
- Armstrong, J.G.; Harrison, L.B.; Thaler, H.T.; Friedlander-Klar, H.; Fass, D.E.; Zelefsky, M.J.; Shah, J.P.; Strong, E.W.; Spiro, R.H. The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer 1992, 69, 615–619. [Google Scholar] [CrossRef]
- Kawata, R.; Koutetsu, L.; Yoshimura, K.; Nishikawa, S.; Takenaka, H. Indication for elective neck dissection for N0 carcinoma of the parotid gland: A single institution’s 20-year experience. Acta Otolaryngol. 2010, 130, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Zbären, P.; Schüpbach, J.; Nuyens, M.; Stauffer, E. Elective neck dissection versus observation in primary parotid carcinoma. Otolaryngol. Head Neck Surg. 2005, 132, 387–391. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) International Union Against Cancer (UICC): TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Oxford, UK, 2017. [Google Scholar]
- Yanagihara, N. Grading of facial palsy. In Proceedings of the Third International Symposium on Facial Nerve Surgery, Zurich, Switzerland, 9–12 August 1976; Aesculapius Publishing Company: Zurich, Switzerland, 1976; pp. 533–535. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software EZR for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Spiro, J.D.; Spiro, R.H. Cancer of the parotid gland: Role of 7th nerve preservation. World J. Surg. 2003, 27, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Spencer, S.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; Colevas, A.D.; Dunphy, F.; Eisele, D.W.; et al. Head and neck cancers, Version 2.2014. Clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2014, 12, 1454–1487. [Google Scholar] [CrossRef] [Green Version]
- Kaura, A.; Kennedy, R.A.; Ali, S.; Odell, E.; Simo, R.; Jeannon, J.P.; Oakley, R. Utility of neck dissection for management of carcinoma of the parotid gland. Br. J. Oral Maxillofac. Surg. 2019, 57, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Israel, Y.; Rachmiel, A.; Gourevich, K.; Nagler, R. Mortality rates and prognostic factors in patients with malignant salivary tumors. Med. Oncol. 2019, 36, 65. [Google Scholar] [CrossRef]
- Valstar, M.H.; van den Brekel, M.W.; Smeele, L.E. Interpretation of treatment outcome in the clinically node-negative neck in primary parotid carcinoma: A systematic review of the literature. Head Neck 2010, 32, 1402–1411. [Google Scholar] [CrossRef]
- Qian, K.; Guo, K.; Zheng, X.; Sun, W.; Sun, T.; Chen, L.; Ma, D.; Wu, Y.; Ji, Q.; Wang, Z. The limited role of elective neck dissection in patients with cN0 salivary gland carcinoma. J. Craniomaxillofac. Surg. 2019, 47, 47–52. [Google Scholar] [CrossRef]
- Terhaard, C.H.; Lubsen, H.; Rasch, C.R.; Levendag, P.C.; Kaanders, H.H.; Tjho-Heslinga, R.E.; van Den Ende, P.L.; Burlage, F. The role of radiotherapy in the treatment of malignant salivary gland tumors. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 103–111. [Google Scholar] [CrossRef]
- Sood, S.; McGurk, M.; Vaz, F. Management of Salivary Gland Tumours: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S142–S149. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Garcia, J.; Bucci, M.K.; Quivey, J.M.; Eisele, D.W. The role of postoperative radiation therapy in carcinoma ex pleomorphic adenoma of the parotid gland. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Stodulski, D.; Mikaszewski, B.; Stankiewicz, C. Are all prognostic factors in parotid gland carcinoma well recognized? Eur. Arch. Otorhinolaryngol. 2012, 269, 1019–1025. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.W.; Hong, H.J.; Ban, M.J.; Shin, Y.S.; Kim, W.S.; Koh, Y.W.; Choi, E.C. Prognostic Factors and Treatment Outcomes of Parotid Gland Cancer: A 10-Year Single-Center Experience. Otolaryngol. Head Neck Surg. 2015, 153, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Yasumatsu, R.; Kogo, R.; Hashimoto, K.; Asai, K.; Ohga, S.; Yamamoto, H.; Nakashima, T.; Nakagawa, T. Parotid gland carcinoma: 32 years’ experience from a single institute. J. Laryngol. Otol. 2019, 133, 604–609. [Google Scholar] [CrossRef]
- Kandaz, M.; Soydemir, G.; Bahat, Z.; Canyilmaz, E.; Yoney, A. Prognostic Factors and Clinical Outcome in Parotid Gland Tumors: A Single Institution Experience from the Eastern Black Sea Region of Turkey. Asian Pac. J. Cancer Prev. 2016, 17, 1169–1174. [Google Scholar] [CrossRef] [Green Version]
- Parikh, A.S.; Khawaja, A.; Puram, S.V.; Srikanth, P.; Tjoa, T.; Lee, H.; Sethi, R.K.V.; Bulbul, M.; Varvares, M.A.; Rocco, J.W.; et al. Outcomes and prognostic factors in parotid gland malignancies: A 10-year single center experience. Laryngoscope Investig. Otolaryngol. 2019, 4, 632–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.B.; Delord, J.P.; Doi, T.; Piha-Paul, S.A.; Liu, S.V.; Gilbert, J.; Algazi, A.P.; Damian, S.; Hong, R.L.; Le Tourneau, C.; et al. Pembrolizumab for the Treatment of Advanced Salivary Gland Carcinoma: Findings of the Phase 1b KEYNOTE-028 Study. Am. J. Clin. Oncol. 2018, 41, 1083. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, K.; Miyahara, N.; Chikuie, N.; Hamamoto, T.; Ishino, T.; Ueda, T.; Takeno, S. Efficacy of anti-PD-1 therapy in a patient with brain metastasis of parotid carcinoma: A case report. Auris Nasus Larynx 2019, 46, 813–817. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Group A (n = 29) | Group B (n = 38) | p Value |
|---|---|---|---|
| Median age (range), years | 54 (15–74) | 62 (20–89) | 0.040 * |
| Sex | 0.93 | ||
| Male | 18 | 22 | |
| Female | 11 | 16 | |
| Preoperative facial nerve palsy | 0.42 | ||
| No | 26 | 37 | |
| Yes | 3 | 1 | |
| Clinical T classification | 0.075 | ||
| T1 | 2 | 9 | |
| T2 | 15 | 9 | |
| T3 | 4 | 6 | |
| T4 | 8 | 14 | |
| Clinical N classification | |||
| N0 | 22 | 36 | 0.090 |
| N1 | 3 | 0 | |
| N2b | 3 | 2 | |
| N2c | 1 | 0 | |
| Disease stage | 0.16 | ||
| I | 2 | 9 | |
| II | 12 | 8 | |
| III | 4 | 6 | |
| IV | 11 | 15 | |
| Surgery | |||
| Parotid resection | <0.001 * | ||
| Partial | 4 | 31 | |
| Total | 25 | 7 | |
| Facial nerve resection | 0.0291 * | ||
| Preserved | 17 | 26 | |
| Partial | 1 | 8 | |
| Total | 11 | 4 | |
| Neck dissection | <0.001 * | ||
| Yes | 12 | 2 | |
| No | 17 | 36 | |
| Postoperative facial nerve palsy | 0.15 | ||
| No | 10 | 21 | |
| Yes | 19 | 17 | |
| Postoperative radiotherapy | 0.75 | ||
| Yes | 14 | 21 | |
| No | 15 | 17 |
| Histological Grade | Histology | Group A (n = 29) | Group B (n = 38) | Total |
|---|---|---|---|---|
| Low | 16 | 17 | 33 | |
| Mucoepidermoid carcinoma, low grade | 8 | 6 | 14 | |
| Acinic cell carcinoma | 8 | 7 | 15 | |
| Epithelial-myoepithelial carcinoma | 0 | 2 | 2 | |
| Carcinoma ex-plemorphic adenoma, non- invasive | 0 | 1 | 1 | |
| Basal cell adenocarcinoma | 0 | 1 | 1 | |
| Intermediate | 3 | 1 | 4 | |
| Adenocystic carcinoma, tubular type | 1 | 1 | 2 | |
| Adenocystic carcinoma, cribriform type | 2 | 0 | 2 | |
| High | 10 | 20 | 30 | |
| Mucoepidermoid carcinoma, high grade | 4 | 5 | 9 | |
| Carcinoma ex-plemorphic adenoma, invasive | 3 | 8 | 11 | |
| Squamous cell carcinoma | 1 | 3 | 4 | |
| Adenocystic carcinoma, solid type | 1 | 1 | 2 | |
| Adenocarcinoma, NOS | 0 | 1 | 1 | |
| Salivary duct carcinoma | 1 | 1 | 2 | |
| Undifferentiated carcinoma | 0 | 1 | 1 |
| (a) Group A | ||||||
|---|---|---|---|---|---|---|
| Variable (Number) | OS (5 Years) | p | DSS (5 Years) | p | DFS (5 Years) | p |
| Age (years) | 0.604 | 0.608 | 0.508 | |||
| <60 (22) | 73.9% | 78.1% | 56.2% | |||
| 60 or higher (7) | 85.7% | 85.7% | 85.7% | |||
| Sex | 0.007 * | 0.013 * | 0.006 * | |||
| Male (18) | 61.3% | 65.7% | 41.4% | |||
| Female (11) | 100% | 100% | 100% | |||
| Clinical T classification | <0.001 * | <0.001 * | <0.001 * | |||
| T1–3 (24) | 91.3% | 95.5% | 81.8% | |||
| T4 (5) | 0.0% | 0.0% | 0.0% | |||
| Clinical N classification | 0.208 | 0.043 * | 0.009 * | |||
| N0 (22) | 84.0% | 88.2% | 76.5% | |||
| N+ (7) | 53.6% | 53.6% | 19.0% | |||
| Disease stage | <0.001 * | <0.001 * | <0.001 * | |||
| I–III (23) | 95.5% | 100.0% | 85.7% | |||
| IV (6) | 0.0% | 0.0% | 0.0% | |||
| Facial nerve invasion | 0.348 | 0.075 | 0.17 | |||
| No (17) | 87.5% | 93.3% | 80.0% | |||
| Yes (12) | 55.6% | 55.6% | 37.5% | |||
| Histology grade | 0.147 | 0.026 * | 0.274 | |||
| Low/intermediate (19) | 88.9% | 94.4% | 76.5% | |||
| High (10) | 34.3% | 34.3% | 28.6% | |||
| Postoperative radiotherapy | 0.788 | 0.218 | 0.96 | |||
| Yes (14) | 62.3% | 62.3% | 53.0% | |||
| No (15) | 85.7% | 92.9% | 69.2% | |||
| (b) Group B | ||||||
| Variable (Number) | OS (5 Years) | p | DSS (5 Years) | p | DFS (5 Years) | p |
| Age (years) | 0.770 | 0.580 | 0.997 | |||
| <60 (13) | 73.3% | 73.3% | 75.5% | |||
| 60 or higher (25) | 80.6% | 86.3% | 70.2% | |||
| Sex | 0.481 | 0.599 | 0.771 | |||
| Male (22) | 72.5% | 78.5% | 74.1% | |||
| Female (16) | 83.9% | 83.9% | 69.9% | |||
| Clinical T classification | 0.014 * | 0.002 * | 0.006 * | |||
| T1–3 (24) | 93.8% | 100.0% | 87.5% | |||
| T4 (14) | 55.0% | 55.0% | 50.0% | |||
| Clinical N classification | <0.001 * | <0.001 * | <0.001 * | |||
| N0 (36) | 82.3% | 85.8% | 76.9% | |||
| N+ (2) | 0.0% | 0.0% | 0.0% | |||
| Disease stage | 0.025 * | 0.004 * | 0.013 * | |||
| I–III (23) | 93.3% | 100.0% | 86.7% | |||
| IV (15) | 58.2% | 58.2% | 53.3% | |||
| Facial nerve invasion | 0.009 * | 0.001 * | 0.003 * | |||
| No (28) | 89.2% | 94.1% | 85.7% | |||
| Yes (10) | 50.0% | 50.0% | 40.0% | |||
| Histology grade | 0.483 | 0.102 | 0.214 | |||
| Low/intermediate (18) | 84.6% | 91.7% | 86.6% | |||
| High (20) | 70.9% | 70.9% | 60.7% | |||
| Postoperative radiotherapy | 0.633 | 0.720 | 0.927 | |||
| Yes (21) | 81.9% | 81.9% | 72.6% | |||
| No (17) | 70.8% | 77.9% | 72.8% | |||
| No | Histology | cT | cN | cStage | Grade | PORT † | Recurrence Site and Management | Status at Last Follow-Up |
|---|---|---|---|---|---|---|---|---|
| Group A | ||||||||
| 1 | Acinic cell carcinoma | 2 | 0 | 2 | Low grade | − | LR: salvage surgery → controlled | 58 months, alive |
| 2 | Acinic cell carcinoma | 2 | 0 | 2 | Low grade | − | LR, CLNR: salvage surgery → controlled DM: chemoradiation therapy | 152 months, died |
| 3 | Mucoepidermoid carcinoma | 4a | 2b | 4a | High grade | + | LR: palliative care | 22 months, died |
| 4 | Mucoepidermoid carcinoma | 2 | 1 | 3 | Low grade | + | LR: salvage surgery → controlled | 328 months, alive |
| 5 | Acinic cell carcinoma | 2 | 0 | 2 | Low grade | − | LR, CLNR: unknown | 228 months, alive |
| 6 | Adenoid cystic carcinoma | 4a | 2b | 4a | Intermediate grade | + | LR, CLNR, DM: unknown | 8 months, died |
| 7 | Carcinoma ex-plemorphic adenoma | 4a | 0 | 4a | High grade | + | LR: unknown | 57 months, died |
| 8 | Mucoepidermoid carcinoma | 4a | 2c | 4a | High grade | − | LR, CLNR, DM: unknown | 23 months, alive |
| 9 | Mucoepidermoid carcinoma | 4a | 2b | 4a | High grade | − | LR, CLNR, DM: unknown | 9 months, died |
| 10 | Mucoepidermoid carcinoma | 2 | 0 | 2 | Low grade | − | LR: unknown | 272 months, alive |
| 11 | Squamous cell carcinoma | 2 | 0 | 2 | High grade | + | DM: unknown | 19 months, died |
| Group B | ||||||||
| 1 | Mucoepidermoid carcinoma | 4b | 2b | 4b | High grade | + | DM: salvage surgery → uncontrolled | 52 months, died |
| 2 | Mucoepidermoid carcinoma | 3 | 0 | 3 | High grade | + | DM: salvage surgery → controlled | 95 months, alive |
| 3 | Carcinoma ex-plemorphic adenoma | 4a | 2b | 4a | High grade | − | CLNR: palliative care | 10 months, died |
| 4 | Carcinoma ex-plemorphic adenoma | 4a | 0 | 4a | High grade | + | CLNR: salvage surgery → controlled | 146 months, alive |
| 5 | Carcinoma ex-plemorphic adenoma | 4a | 0 | 4a | High grade | + | LR, CLNR: salvage surgery → controlledDM: palliative care | 34 months, died |
| 6 | Acinic cell carcinoma | 4b | 0 | 4b | Low grade | − | CLNR: salvage surgery → controlled DM: palliative care | 55 months, died |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, H.; Kojima, T.; Okanoue, Y.; Otsuki, S.; Hasebe, K.; Yuki, R.; Hori, R. Impact of Changing Surgical Strategies on Clinical Outcomes in Patients with Parotid Carcinoma: A 53-Year Single-Institution Experience. Medicina 2021, 57, 745. https://doi.org/10.3390/medicina57080745
Yamamoto H, Kojima T, Okanoue Y, Otsuki S, Hasebe K, Yuki R, Hori R. Impact of Changing Surgical Strategies on Clinical Outcomes in Patients with Parotid Carcinoma: A 53-Year Single-Institution Experience. Medicina. 2021; 57(8):745. https://doi.org/10.3390/medicina57080745
Chicago/Turabian StyleYamamoto, Hirotaka, Tsuyoshi Kojima, Yusuke Okanoue, Shuya Otsuki, Koki Hasebe, Ryohei Yuki, and Ryusuke Hori. 2021. "Impact of Changing Surgical Strategies on Clinical Outcomes in Patients with Parotid Carcinoma: A 53-Year Single-Institution Experience" Medicina 57, no. 8: 745. https://doi.org/10.3390/medicina57080745