
Cardiac Rehabilitation and Complementary Physical Training in Elderly Patients after Acute Coronary Syndrome: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
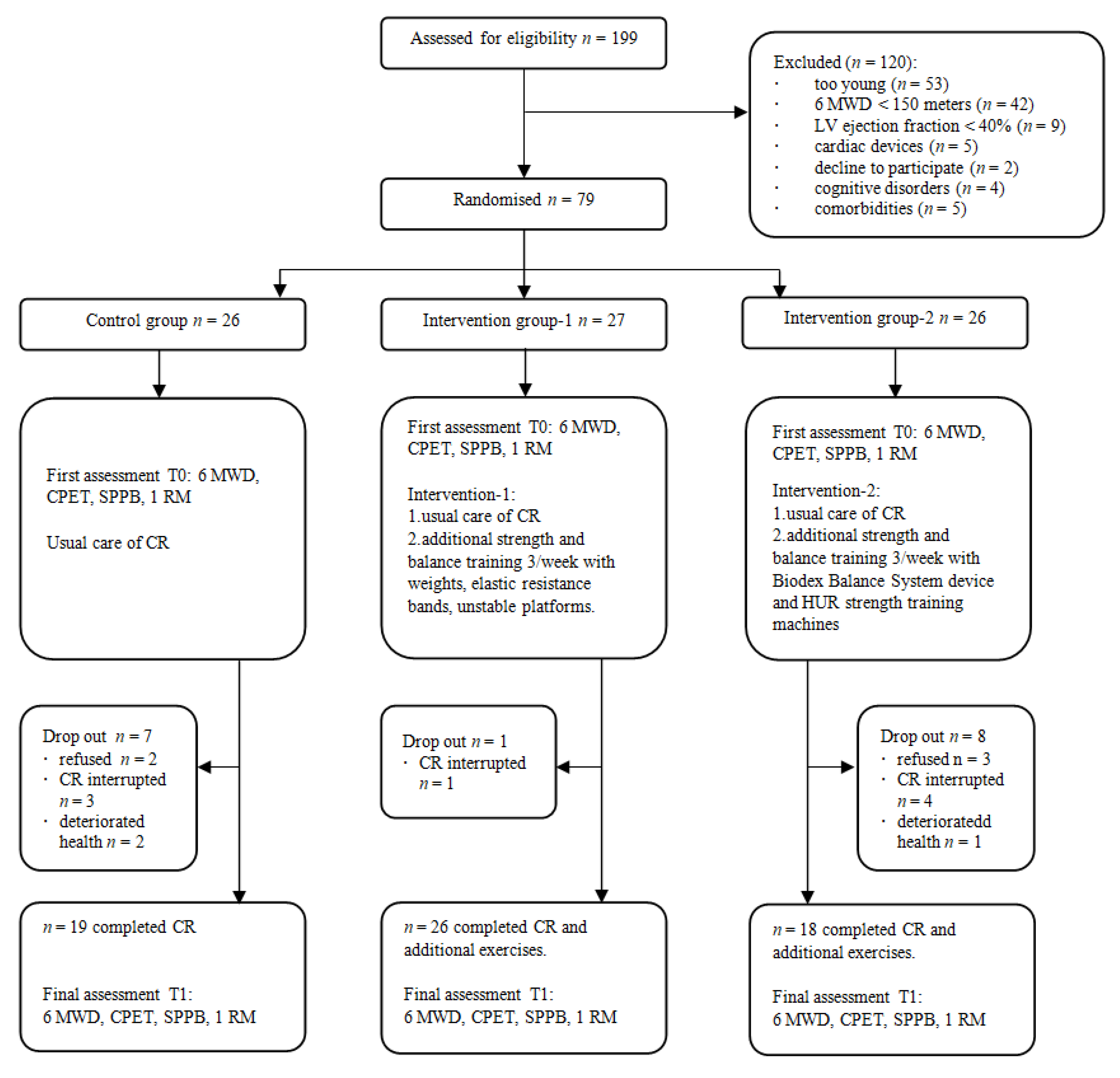
2.1. Study Design and Participants
2.2. Study Assessment
2.3. Study Interventions
2.4. Statistical Analysis
3. Results
Effectiveness of Cardiac Rehabilitation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Price, K.J.; Gordon, B.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Taylor, R.S. Cardiac rehabilitation for people with heart disease: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2014, 2014, CD011273. [Google Scholar] [CrossRef]
- Anderson, L.; Thompson, D.R.; Oldridge, N.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2016, 1, CD001800. [Google Scholar] [CrossRef] [Green Version]
- Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 1, CD003331. [Google Scholar] [CrossRef] [Green Version]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation 2019, 140, e69–e89. [Google Scholar] [CrossRef]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance Exercise in Individuals with and Without Cardiovascular Disease: 2007 Update: A Scientific Statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molino-Lova, R.; Pasquini, G.; Vannetti, F.; Paperini, A.; Forconi, T.; Polcaro, P.; Zipoli, R.; Cecchi, F.; Macchi, C. Effects of a structured physical activity intervention on measures of physical performance in frail elderly patients after cardiac rehabilitation: A pilot study with 1-year follow-up. Intern. Emerg. Med. 2013, 8, 581–589. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Dere, W.; Evans, W.; Kanis, J.A.; Rizzoli, R.; Sayer, A.A.; Sieber, C.C.; Kaufman, J.-M.; Van Kan, G.A.; Boonen, S.; et al. Frailty and sarcopenia: Definitions and outcome parameters. Osteoporos. Int. 2012, 23, 1839–1848. [Google Scholar] [CrossRef]
- World Health Organization. WHO Clinical Consortium on Healthy Ageing: Topic Focus: Frailty and Intrinsic Capacity: Report of Consortium Meeting; 1–2 December 2016 in Geneva, Switzerland. World Health Organization. 2017. Available online: https://apps.who.int/iris/handle/10665/272437 (accessed on 30 March 2021).
- Hertz, K.; Santy-Tomlinson, J. (Eds.) Fragility Fracture Nursing: Holistic Care and Management of the Orthogeriatric Patient; Springer International Publishing: Cham, Switzerland, 2018. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [Green Version]
- ATS. Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS Statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Lazinica, B.; Schoenfeld, B.J.; Pedisic, Z. Test–Retest Reliability of the One-Repetition Maximum (1RM) Strength Assessment: A Systematic Review. Sports Med.-Open 2020, 6, 31. [Google Scholar] [CrossRef]
- Decato, T.W.; Haverkamp, H.; Hegewald, M.J. Cardiopulmonary Exercise Testing (CPET). Am. J. Respir. Crit. Care Med. 2020, 201, P1–P2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JCS Joint Working Group. Guidelines for Rehabilitation in Patients with Cardiovascular Disease (JCS 2012): Digest Version. Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef] [Green Version]
- Biodex. Available online: https://www.biodex.com/sites/default/files/950300man_08060.pdf (accessed on 30 March 2021).
- Siddiqi, F.A.; Masood, T. Training on Biodex balance system improves balance and mobility in the elderly. J. Pak. Med. Assoc. 2018, 68, 1655–1659. [Google Scholar]
- LR Sveikatos Apsaugos Ministro Įsakymas V-50 Dėl Medicininės Reabilitacijos ir Sanatorinio (Antirecidyvinio) Gydymo Organi-Zavimo. Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/TAIS.313664/qcprTtREST (accessed on 2 April 2021).
- Yamamoto, S.; Hotta, K.; Ota, E.; Mori, R.; Matsunaga, A. Effects of resistance training on muscle strength, exercise capacity, and mobility in middle-aged and elderly patients with coronary artery disease: A meta-analysis. J. Cardiol. 2016, 68, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, P.A.; Shaw, A.O.; Miller, M.S.; Vanburen, P.; Lewinter, M.M.; Ades, P.A.; Toth, M.J. Effect of Resistance Training on Physical Disability in Chronic Heart Failure. Med. Sci. Sports Exerc. 2011, 43, 1379–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ximenes, N.N.P.S.; Borges, D.L.; Lima, R.O.; Silva, M.G.B.; Da Silva, L.N.; Costa, M.D.A.G.; Baldez, T.E.P.; Nina, V.J.D.S. Effects of resistance exercise applied early after coronary artery bypass grafting: A randomized controlled trial. Braz. J. Cardiovasc. Surg. 2015, 30, 620–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.-H.; Jang, Y.-C.; Song, M.-K.; Park, H.-K.; Choi, I.-S.; Han, J.-Y. Changes in Aerobic Capacity Over Time in Elderly Patients with Acute Myocardial Infarction During Cardiac Rehabilitation. Ann. Rehabil. Med. 2020, 44, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Deley, G.; Culas, C.; Blonde, M.-C.; Mourey, F.; Vergès, B. Physical and Psychological Effectiveness of Cardiac Rehabilitation: Age Is Not a Limiting Factor! Can. J. Cardiol. 2019, 35, 1353–1358. [Google Scholar] [CrossRef]
- Busch, J.C.; Lillou, D.; Wittig, G.; Bartsch, P.; Willemsen, D.; Oldridge, N.; Bjarnason-Wehrens, B. Resistance and Balance Training Improves Functional Capacity in Very Old Participants Attending Cardiac Rehabilitation After Coronary Bypass Surgery. J. Am. Geriatr. Soc. 2012, 60, 2270–2276. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Queirós, C. Frailty, Sarcopenia and Falls. In Fragility Fracture Nursing; Hertz, K., Santy-Tomlinson, J., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 15–26. [Google Scholar] [CrossRef] [Green Version]
- Baldasseroni, S.; Pratesi, A.; Francini, S.; Pallante, R.; Barucci, R.; Orso, F.; Burgisser, C.; Marchionni, N.; Fattirolli, F. Cardiac Rehabilitation in Very Old Adults: Effect of Baseline Functional Capacity on Treatment Effectiveness. J. Am. Geriatr. Soc. 2016, 64, 1640–1645. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | All (n = 63) | IG-1 (n = 26) | IG-2 (n = 18) | CG (n = 19) | p Value * |
|---|---|---|---|---|---|
| Age, years | 72.9 ± 5.5 | 72.9 ± 4.4 | 70.1 ± 4 | 75.5 ± 6.9 | 0.010 |
| Sex, n (%) | |||||
| Female | 17 (27) | 7 (26.9) | 6 (33.3) | 4 (21.1) | 0.673 |
| Male | 46 (73) | 19 (73.1) | 12 (66.7) | 15 (78.9) | |
| Height, m | 1.7 ± 0.8 | 1.7 ± 0.7 | 1.7 ± 0.9 | 1.7 ± 0.8 | 0.268 |
| Weight, kg | 81.9 ± 14.2 | 82 ± 13.1 | 86.2 ± 17.5 | 77.6 ± 11.4 | 0.185 |
| Body mass index, kg/m2 | 28.1 ± 3.7 | 28.7 ± 3.5 | 28.6 ± 3.8 | 26.9 ± 3.7 | 0.228 |
| Current smokers, n (%) | 5 (7.9) | 2 (7.7) | 2 (11.1) | 1 (5.3) | 0.858 |
| LV ejection fraction, % | 48.2 ± 5.1 | 49.6 ± 4.9 | 46.8 ± 4.2 | 47.6 ± 5.8 | 0.166 |
| Initiation of CR after index event, days | 9.7 ± 4 | 10.7 ± 4 | 9.2 ± 4.5 | 8.9 ± 3.2 | 0.256 |
| CR duration, days | 18.7 ± 1.7 | 19.5 ± 0.9 | 18.1 ± 1.8 | 18.2 ± 2.1 | 0.009 |
| Comorbidities, n (%) | |||||
| Diabetes | 11 (17.5) | 7 (26.9) | 1 (5.6) | 3 (15.8) | 0.184 |
| Atrial fibrillation | 12 (19) | 5 (19.2) | 3 (16.7) | 4 (21.1) | 0.944 |
| Degenerative joint disease | 5 (7.9) | 1 (3.8) | 3 (16.7) | 1 (5.3) | 0.265 |
| Cancer | 4 (6.3) | 1 (3.8) | 2 (11.1) | 1 (5.3) | 0.607 |
| Treatment, n (%) | |||||
| Coronary artery by-pass graft | 32 (50.8) | 19 (73.1) | 5 (27.8) | 8 (42.1) | 0.009 |
| PTCA | 31 (49.2) | 7 (26.9) | 13 (72.2) | 11 (57.9) | |
| Medication, n (%) | |||||
| ACE inhibitor | 49 (77.8) | 17 (65.4) | 15 (83.3) | 17 (89.5) | 0.126 |
| Diuretic | 42 (66.7) | 20 (76.9) | 11 (61.1) | 11 (57.9) | 0.343 |
| Statin | 62 (98.4) | 25 (96.2) | 18 (100) | 19 (100) | 0.485 |
| Parameters | Intervention Group 1 (n = 26) | p * | Intervention Group 2 (n = 28) | p * | Control Group (n = 19) | p * | |||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | T0 | T1 | ||||
| 6MWD, m | 285 (233; 316) | 388 (338; 419.5) | <0.001 | 348.5 (336.5; 403) | 434.5 (392.5; 475.2) | <0.001 | 319 (224; 406) | 420 (350; 466) | <0.001 |
| Peak workload, watt | 64 (51; 74.7) | 75 (59; 84.5) | <0.001 | 78.5 (58.2; 93) | 93.5 (58.2; 107.7) | <0.001 | 85 (58; 98) | 89 (57; 125) | 0.004 |
| Peak VO2, mL/kg/min | 9.3 (8.4; 11.1) | 11.2 (10.8; 12.3) | 0.009 | 11.8 (8.8; 12.9) | 12.3 (9.4; 15.3) | 0.093 | 11.6 (9.3; 15.2) | 12.1 (10; 14.3) | 0.365 |
| SPPB, score | 9 (7.7; 10) | 10.5 (9.2; 11.7) | <0.001 | 10.5 (9.7; 11.2) | 11.5 (10; 12) | 0.006 | 9 (8; 10) | 11 (9; 12) | <0.001 |
| Leg press 1RM, kg | 31.5 (28; 48) | 48 (41.2; 56) | <0.001 | 38 (31.7; 46.2) | 55.5 (42.7; 56) | 0.001 | 45 (33; 52) | 50 (45; 65) | 0.001 |
| Parameters | Intervention Group 1 (n = 26) | Intervention Group 2 (n = 18) | Control Group (n = 19) | p Value * |
|---|---|---|---|---|
| T1–T0 | T1–T0 | T1–T0 | ||
| 6MWD, m | 90.5 (46; 125.5) | 66.5 (39; 76.7) | 89 (29; 151) | 0.317 |
| Peak workload, watt | 7.5 (4; 20) | 13 (5; 21) | 10 (4; 15) | 0.596 |
| Peak VO2, mL/kg/min | 1.8 (0.4; 3.5) | 1.75 (–0.5; 2.5) | 0.55 (–0.47; 1.47) | 0.103 |
| SPPB, score | 1 (0; 2) | 1 (0; 1) | 1 (1; 2) | 0.295 |
| Leg press 1RM, kg | 14 (8.2; 16.7) | 12.5 (3.7; 21) | 8 (2; 15) | 0.206 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beigienė, A.; Petruševičienė, D.; Barasaitė, V.; Kubilius, R.; Macijauskienė, J. Cardiac Rehabilitation and Complementary Physical Training in Elderly Patients after Acute Coronary Syndrome: A Pilot Study. Medicina 2021, 57, 529. https://doi.org/10.3390/medicina57060529
Beigienė A, Petruševičienė D, Barasaitė V, Kubilius R, Macijauskienė J. Cardiac Rehabilitation and Complementary Physical Training in Elderly Patients after Acute Coronary Syndrome: A Pilot Study. Medicina. 2021; 57(6):529. https://doi.org/10.3390/medicina57060529
Chicago/Turabian StyleBeigienė, Aurelija, Daiva Petruševičienė, Vitalija Barasaitė, Raimondas Kubilius, and Jūratė Macijauskienė. 2021. "Cardiac Rehabilitation and Complementary Physical Training in Elderly Patients after Acute Coronary Syndrome: A Pilot Study" Medicina 57, no. 6: 529. https://doi.org/10.3390/medicina57060529