
Sex-Specific Autonomic Responses to Acute Resistance Exercise




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
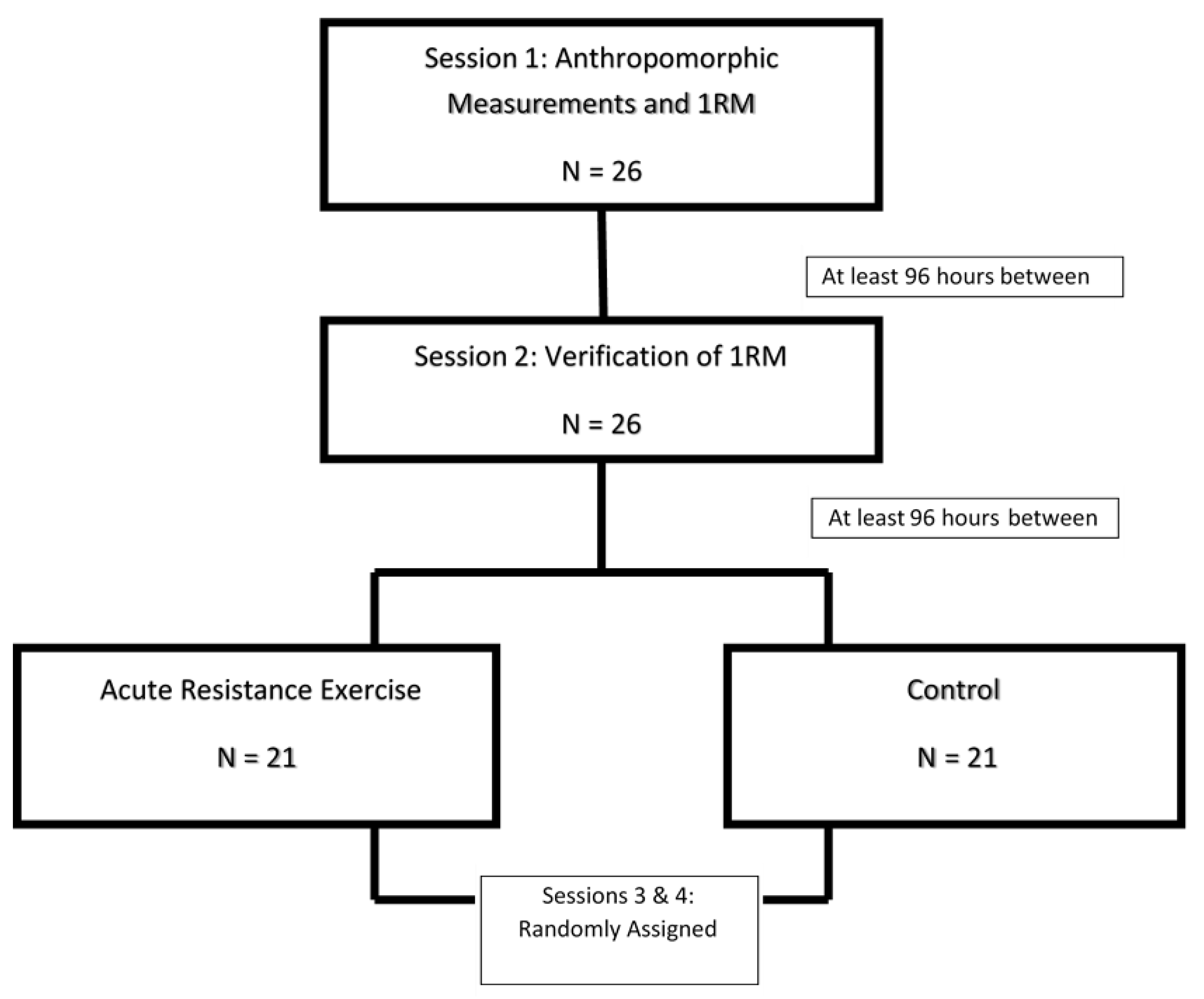
2.2. Study Design
2.3. Anthropometrics
2.4. Maximal Strength
2.5. Autonomic Modulation
2.6. Acute Resistance Exercise
2.7. Statistics
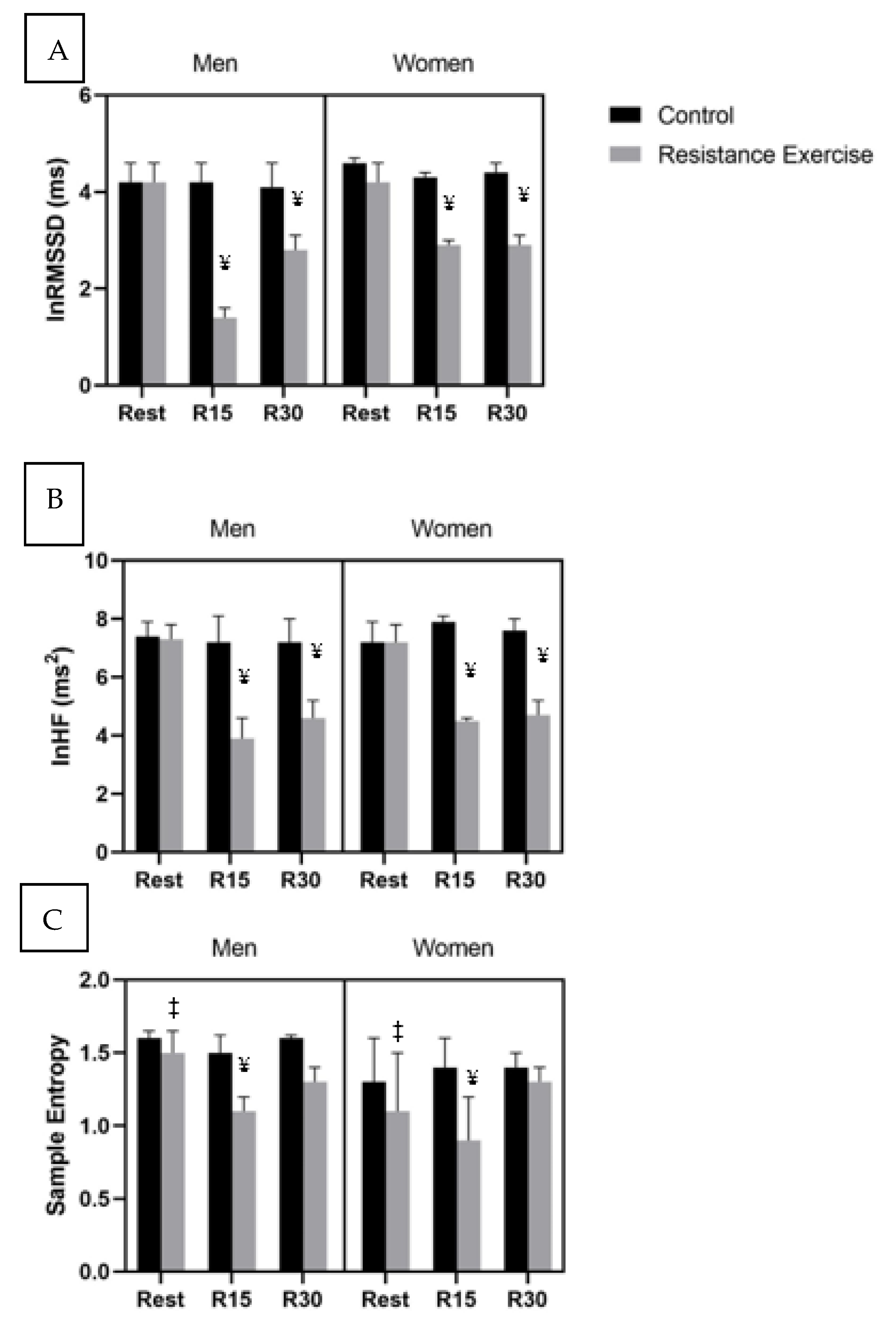
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pollock, M.L.; Franklin, B.A.; Balady, G.J.; Chaitman, B.L.; Fleg, J.L.; Fletcher, B.; Limacher, M.; Piña, I.L.; Stein, R.A.; Williams, M. Resistance exercise in individuals with and without cardiovascular disease: Benefits, rationale, safety, and prescription an advisory from the committee on exercise, rehabilitation, and prevention, council on clinical cardiology, American Heart Association. Circulation 2000, 101, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, K.S.; Sosnoff, J.; Jae, S.; Gates, G.; Fernhall, B. Acute resistance exercise reduces heart rate complexity and increases QTc interval. Int. J. Sports Med. 2008, 29, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, J.D.; Hochgesang, S.; Brewer, A.; Buxton, E.; Martinson, M.; Heidner, G. Autonomic modulation in resistance-trained individuals after acute resistance exercise. Int. J. Sports Med. 2014, 35, 851–856. [Google Scholar]
- Kingsley, J.D.; Figueroa, A. Acute and training effects of resistance exercise on heart rate variability. Clin. Physiol. Funct. Imaging 2016, 36, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, J.D.; Tai, Y.-L.; Marshall, E.M.; Glasgow, A.; Oliveira, R.; Parks, J.C.; Mayo, X. Autonomic modulation and baroreflex sensitivity after acute resistance exercise: Responses between sexes. J. Sports Med. Phys. Fitness 2019, 59, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, K.S.; Kelly, E.E.; Collier, S.R.; Fernhall, B. Cardiac autonomic modulation during recovery from acute endurance versus resistance exercise. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 80–86. [Google Scholar] [CrossRef]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Kuusela, T.A.; Jartti, T.T.; Tahvanainen, K.U.; Kaila, T.J. Nonlinear methods of biosignal analysis in assessing terbutaline-induced heart rate and blood pressure changes. Am. J. Phys. Heart Circ. Phys. 2002, 282, H773–H781. [Google Scholar] [CrossRef] [Green Version]
- Tuzcu, V.; Nas, S.; Börklü, T.; Ugur, A. Decrease in the heart rate complexity prior to the onset of atrial fibrillation. Europace 2006, 8, 398–402. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Fahs, C.A.; Shinsako, K.K.; Jae, S.Y.; Fernhall, B. Heart rate recovery and heart rate complexity following resistance exercise training and detraining in young men. Am. J. Phys. Heart Circ. Phys. 2007, 293, H3180–H3186. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, L.; Ritti-Dias, R.M.; Tinucci, T.; Júnior, D.M.; de Moraes Forjaz, C.L. Post-concurrent exercise hemodynamics and cardiac autonomic modulation. Eur. J. Appl. Phys. 2011, 111, 2069–2078. [Google Scholar] [CrossRef]
- Voss, A.; Schroeder, R.; Heitmann, A.; Peters, A.; Perz, S. Short-term heart rate variability—influence of gender and age in healthy subjects. PLoS ONE 2015, 10, e0118308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregoire, J.; Tuck, S.; Hughson, R.L.; Yamamoto, Y. Heart rate variability at rest and exercise: Influence of age, gender, and physical training. Can. J. Appl. Phys. 1996, 21, 455–470. [Google Scholar] [CrossRef]
- Mendonca, G.V.; Heffernan, K.S.; Rossow, L.; Guerra, M.; Pereira, F.D.; Fernhall, B. Sex differences in linear and nonlinear heart rate variability during early recovery from supramaximal exercise. Appl. Phys. Nutr. Metab. 2010, 35, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Collier, S.R. Sex differences in the effects of aerobic and anaerobic exercise on blood pressure and arterial stiffness. Gend. Med. 2008, 5, 115–123. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Ainsworth, B.E.; Jacobs, D.R., Jr.; Leon, A.S. Validity and reliability of self-reported physical activity status: The Lipid Research Clinics questionnaire. Med. Sci. Sports Exerc. 1993, 25, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Draper, C.F.; Duisters, K.; Weger, B.; Chakrabarti, A.; Harms, A.C.; Brennan, L.; Hankemeier, T.; Goulet, L.; Konz, T.; Martin, F.P.; et al. Menstrual cycle rhythmicity: Metabolic patterns in healthy women. Sci. Rep. 2018, 8, 14568. [Google Scholar] [CrossRef]
- Haff, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics: Champagne, IL, USA, 2015; ISBN 1-4925-0162-X. [Google Scholar]
- Teixeira, A.L.; Ritti-Dias, R.; Antonino, D.; Bottaro, M.; Millar, P.J.; Vianna, L.C. Sex differences in cardiac baroreflex sensitivity following isometric handgrip exercise. Med. Sci. Sports Exerc. 2018, 50, 770–777. [Google Scholar] [CrossRef]
- Pal, G.K.; Pal, P.; Lalitha, V.; Dutta, T.K.; Adithan, C.; Nanda, N. Sympathovagal imbalance in young prehypertensives: Importance of male-female difference. Am. J. Med. Sci. 2013, 345, 10–17. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, M.C.; Ricci-Vitor, A.L.; Quizzini, G.H.; de Oliveira, J.V.N.; Vanderlei, L.C.M.; Lira, F.S.; Rossi, F.E. Postexercise hypotension and autonomic modulation response after full versus split body resistance exercise in trained men. J. Exerc. Rehabil. 2018, 14, 399. [Google Scholar] [CrossRef]
- Seals, D.; Taylor, J.; NG, A.; Esler, M. Exercise and aging: Autonomic control of the circulation. Med. Sci. Sports Exerc. 1994, 26, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Mayo, X.; Iglesias-Soler, E.; Fariñas-Rodríguez, J.; Fernández-del-Olmo, M.; Kingsley, J.D. Exercise type affects cardiac vagal autonomic recovery after a resistance training session. J. Strength Cond. Res. 2016, 30, 2565–2573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leicht, A.S.; Allen, G.D.; Hoey, A.J. Influence of age and moderate-intensity exercise training on heart rate variability in young and mature adults. Can. J. Appl. Phys. 2003, 28, 446–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sookan, T.; McKune, A.J. Heart rate variability in physically active individuals: Reliability and gender characteristics. Cardiovasc. J. Afr. 2012, 23, 67. [Google Scholar]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Phys. 2013, 4, 26. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Men (n = 11) | Women (n = 10) | |
|---|---|---|
| Height (m) | 1.8 ± 0.1 * | 1.6 ± 0.1 |
| Weight (kg) | 79 ± 14 * | 60 ± 7 |
| Age (years) | 23 ± 3 | 22 ± 3 |
| BMI (kg·m2) | 25.3 ± 2.5 | 23.1 ± 1.4 |
| Years Training (years) | 3 ± 2 | 2 ± 2 |
| Men (n = 11) | Women (n = 10) | |
|---|---|---|
| Leg Press (kg) | 169 ± 34 * | 106 ± 17 |
| Lat Pulldown (kg) | 140 ± 23 * | 79 ± 13 |
| Chest Press (kg) | 145 ± 26 * | 64 ± 20 |
| Leg Curl (kg) | 88 ± 21 * | 47 ± 10 |
| Leg Extension (kg) | 110 ± 73 * | 72 ± 22 |
| Control | Acute Resistance Exercise | |||||
|---|---|---|---|---|---|---|
| Rest | R15 | R30 | Rest | R15 | R30 | |
| Heart rate (beats·min−1) | ||||||
| Men | 60 ± 12 | 59 ± 13 | 58 ± 12 | 62 ± 11 | 92 ± 11 ¥ | 86 ± 12 ¥ |
| Women | 66 ± 8 | 62 ± 8 | 62 ± 7 | 70 ± 7 | 90 ± 10 ¥ | 85 ± 8 ¥ |
| 95% CI | (59, 68) | (57, 66) | (57, 66) | (61, 71) | (85, 96) | (80, 90) |
| lnTotal Power (ms2) | ||||||
| Men | 8.2 ± 0.8 | 8.4 ± 1.0 | 8.2 ± 0.8 | 8.3 ± 0.9 | 5.9 ± 1.0 ¥µ | 6.5 ± 0.8 ¥µ |
| Women | 8.2 ± 1.1 | 8.5 ± 1.3 | 8.1 ± 1.6 | 8.3 ± 0.8 | 6.4 ± 0.7 ¥µ | 6.7 ± 0.6 ¥µ |
| 95% CI | (7.8, 8.7) | (7.8, 8.8) | (7.4, 8.6) | (7.8, 8.6) | (5.6, 6.6) | (6.2, 7.0) |
| lnLF (ms2) | ||||||
| Men | 6.9 ± 0.8 | 6.9 ± 0.7 | 6.5 ± 0.7 | 6.7 ± 0.8 | 4.9 ± 1.0 ¥µ | 5.5 ± 0.9 ¥µ£ |
| Women | 6.1 ± 2.1 | 7.0 ± 0.0 | 6.2 ± 1.2 | 6.2 ± 2.4 | 5.3 ± 0.8 ¥µ | 5.7 ± 0.5 ¥µ£ |
| 95% CI | (5.9, 7.1) | (5.8, 7.3) | (5.2, 7.3) | (6.1, 7.5) | (4.2, 5.7) | (5.2, 6.3) |
| lnLF/HF (ratio) | ||||||
| Men | 3.7 ± 2.0 | 3.9 ± 1.7 | 4.1 ± 0.8 | 3.5 ± 1.4 | 4.8 ± 1.9 ¥ƒ | 5.1 ± 2.0 ¥ƒ |
| Women | 3.4 ± 0.7 | 3.2 ± 1.8 | 3.2 ± 1.1 | 3.7 ± 0.6 | 5.0 ± 1.5 ¥ƒ | 5.6 ± 1.1 ¥ƒ |
| 95% CI | (3.3, 4.5) | (3.1, 4.7) | (2.9, 4.2) | (3.4, 4.7) | (4.4, 6.5) | (5.0, 6.3) |
| LZEntropy | ||||||
| Men | 0.8 ± 0.0 | 0.8 ± 0.1 | 0.7 ± 0.1 | 0.8 ± 0.0 | 0.5 ± 0.1 ¥ | 0.6 ± 0.1 £ |
| Women | 0.9 ± 0.3 | 0.9 ± 0.3 | 1.0 ± 0.3 | 1.0 ± 0.4 | 0.7 ± 0.2 ¥ | 0.9 ± 0.3 £ |
| 95% CI | (0.7, 0.8) | (0.7, 1.0) | (0.7, 1.1) | (0.7, 1.1) | (0.5, 0.8) | (0.5, 1.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Humm, S.M.; Erb, E.K.; Tagesen, E.C.; Kingsley, J.D. Sex-Specific Autonomic Responses to Acute Resistance Exercise. Medicina 2021, 57, 307. https://doi.org/10.3390/medicina57040307
Humm SM, Erb EK, Tagesen EC, Kingsley JD. Sex-Specific Autonomic Responses to Acute Resistance Exercise. Medicina. 2021; 57(4):307. https://doi.org/10.3390/medicina57040307
Chicago/Turabian StyleHumm, Stacie M., Emily K. Erb, Emily C. Tagesen, and J. Derek Kingsley. 2021. "Sex-Specific Autonomic Responses to Acute Resistance Exercise" Medicina 57, no. 4: 307. https://doi.org/10.3390/medicina57040307