
Chronic Rhinosinusitis with Nasal Polyps: Age and Disease Severity Differences in the Levels of Inflammatory Markers

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics
2.2. Determination of Inflammatory Markers Concentration
2.3. Statistical Analysis
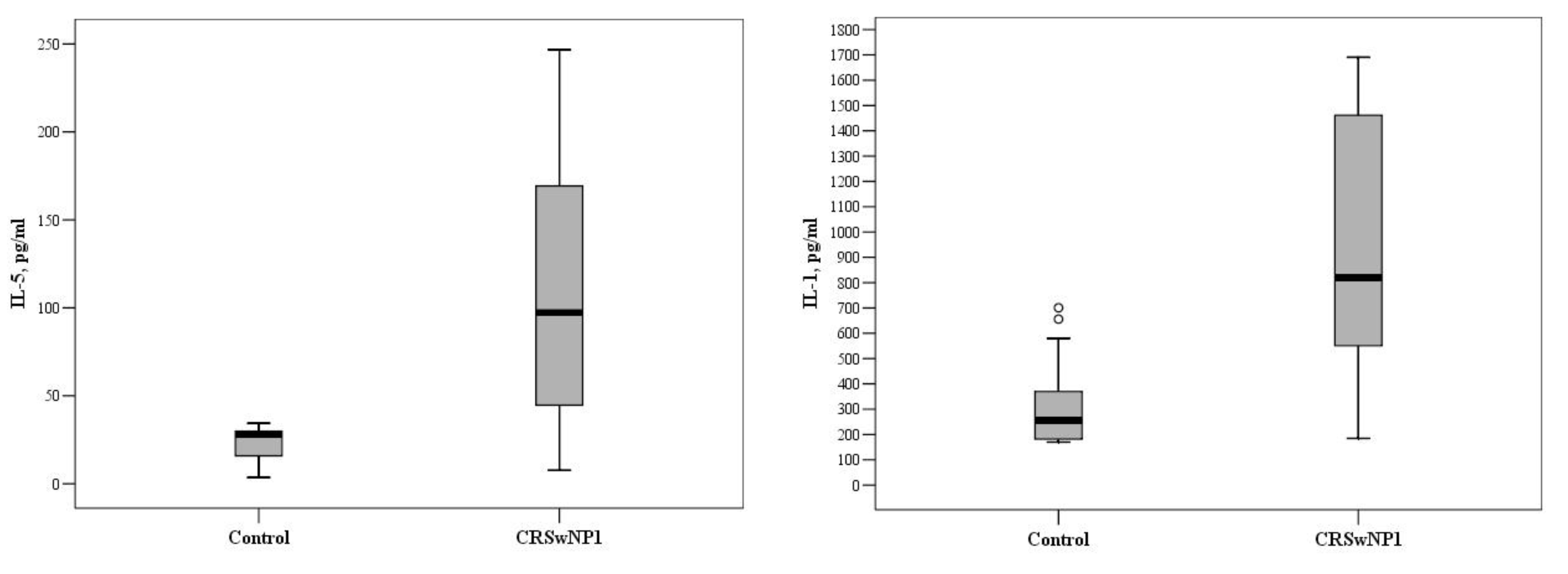
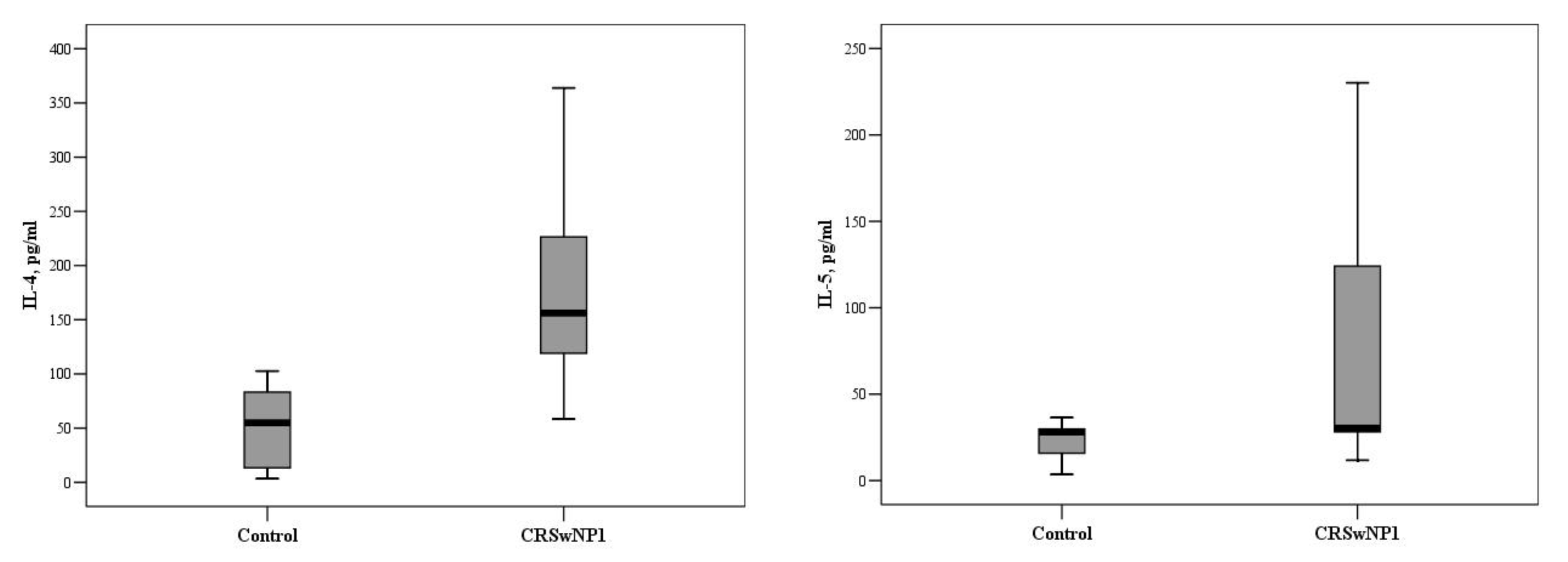
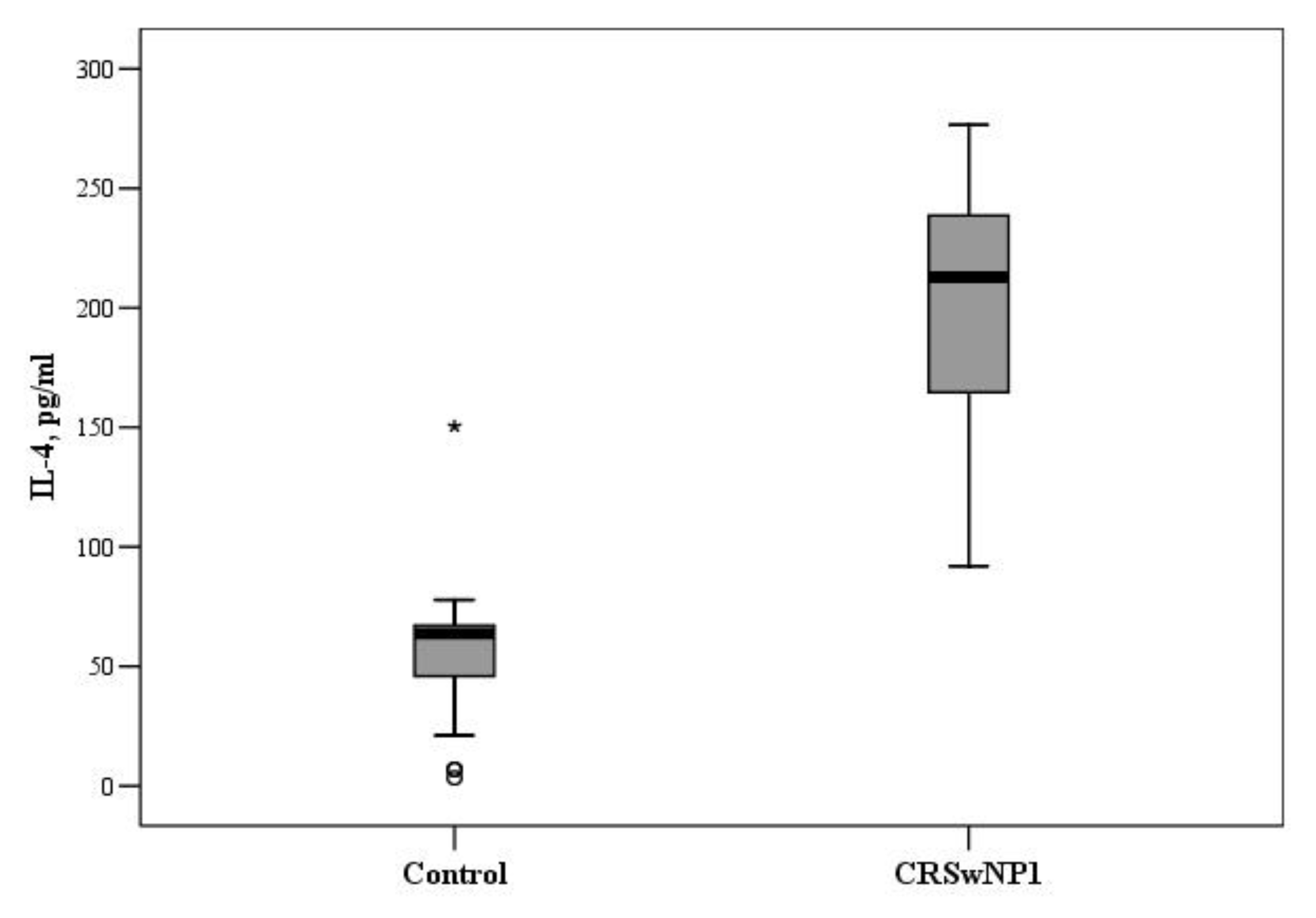
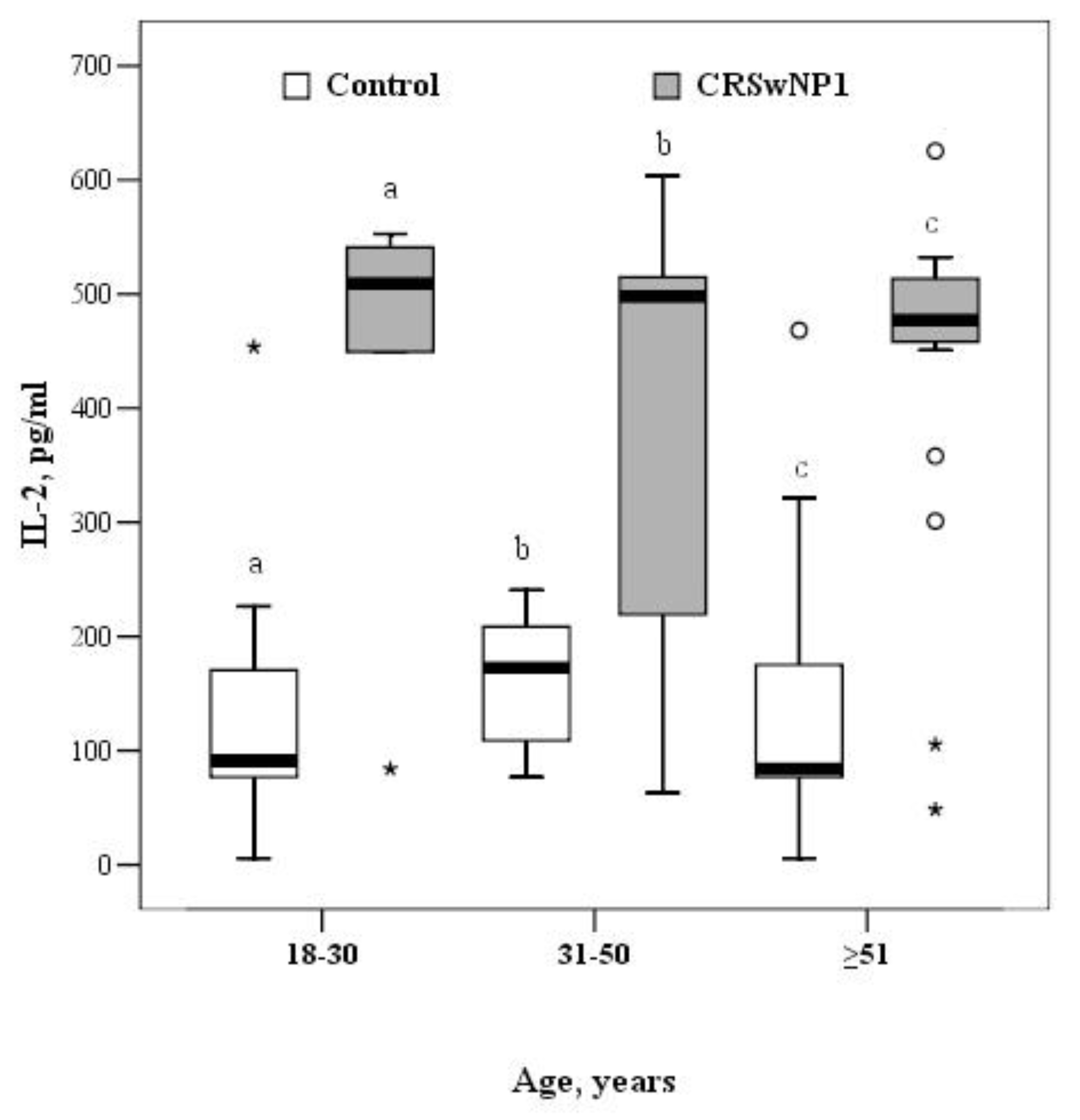
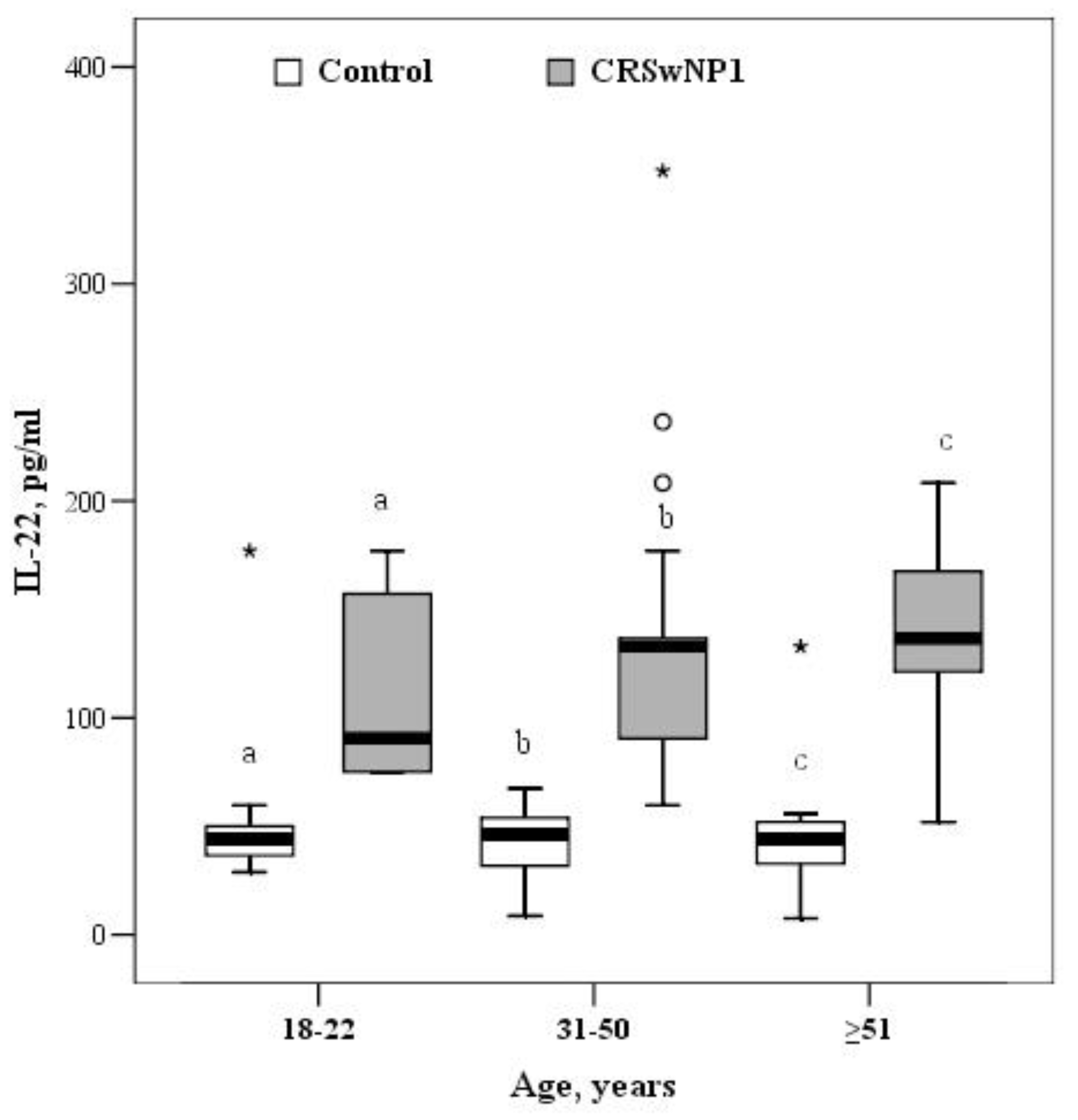
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meltzer, E.O.; Hamilos, D.L.; Hadley, J.A.; Lanza, D.C.; Marple, B.F.; Nicklas, R.A.; Bachert, C.; Baraniuk, J.; Baroody, F.M.; Benninger, M.S.; et al. Rhi-nosinusitis: Establishing definitions for clinical re-search and patient care. Suppl. J. Allergy Clin. Immunol. 2004, 114 (Suppl. 6), S1–S62. [Google Scholar]
- Chalermwatanachai, T.; Vilchez-Vargas, R.; Holtappels, G.; Lacoere, T.; Jáuregui, R.; Kerckhof, F.-M.; Pieper, D.H.; Van De Wiele, T.; Vaneechoutte, M.; Van Zele, T.; et al. Chronic rhinosinusitis with nasal polyps is characterized by dysbacteriosis of the nasal microbiota. Sci. Rep. 2018, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Tyagi, S.; Tyagi, B.S. Impact of active and second hand tobacco smoke on CRS patients: Comparative analysis by CT scanning and nasal endoscopy. Res. J. Allergy Immunol. 2017, 1, 14–16. [Google Scholar]
- Reh, D.D.; Higgins, T.S.; Smith, T.L. Impact of tobacco smoke on chronic rhinosinusitis: A review of the literature. Int. Forum Allergy Rhinol. 2012, 2, 362–369. [Google Scholar] [CrossRef]
- Thomson, N.C.; Chaudhuri, R.; Livingston, E. Asthma and cigarete smoking. Eur. Respir. J. 2004, 24, 822–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berania, I.; Endam, L.M.; Boisvert, P.; Boulet, L.-P.; Bossé, Y.; Desrosiers, M.; Filali-Mouhim, A. Active smoking status in chronic rhinosinusitis is associated with higher serum markers of inflammation and lower serum eosinophilia. Int. Forum Allergy Rhinol. 2014, 4, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Vaitkus, J.; Vitkauskiene, A.; Matuseviciute, V.; Naudziunas, A.; Siupsinskiene, N.; Vaitkus, S. Local inflammatory marker production in Lithuanian patients with chronic rhinosinusitis with nasal polyps. J. Immunotoxicol. 2020, 17, 202–206. [Google Scholar] [CrossRef]
- Kim, D.-K.; Eun, K.M.; Kim, M.-K.; Cho, D.; A Han, S.; Han, S.-Y.; Seo, Y.; Lee, D.-H.; Cho, S.H.; Kim, D.W. Comparison Between Signature Cytokines of Nasal Tissues in Subtypes of Chronic Rhinosinusitis. Allergy, Asthma Immunol. Res. 2019, 11, 201–211. [Google Scholar] [CrossRef]
- Bachert, C.; Marple, B.; Hosemann, W.; Cavaliere, C.; Wen, W.; Zhang, N. Endotypes of Chronic Rhinosinusitis with Nasal Polyps: Pathology and Possible Therapeutic Implications. J. Allergy Clin. Immunol. Pr. 2020, 8, 1514–1519. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.; Chandra, R.K.; Pollak, J.; Kato, A.; Conley, D.B.; Peters, A.T.; Grammer, L.C.; Avila, P.C.; Kern, R.C.; Stewart, W.F.; et al. Incidence and associated premorbid diagnoses of patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 2013, 131, 1350–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.H.; Hong, S.J.; Han, B.; Lee, S.H.; Suh, L.; Norton, J.; Lin, D.; Conley, D.B.; Chandra, R.; Kern, R.C.; et al. Age-related differences in the pathogenesis of chronic rhinosinusitis. J. Allergy Clin. Immunol. 2012, 129, 858–860.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, K.; Tos, M. The Estimated Incidence of Symptomatic Nasal Polyps. Acta Oto-Laryngologica 2002, 122, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Mahdavinia, M.; Grammer, L.C. Chronic rhinosinusitis and age: Is the pathogenesis different? Expert Rev. Anti-infective Ther. 2013, 11, 1029–1040. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinol. J. 2012, 50, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lund, V.J.; Mackay, I.S. Staging in rhinosinusitis. Rhinology 1993, 31, 183–184. [Google Scholar] [CrossRef]
- Vaitkus, S.; Padervinskis, E.; Balsevicius, T.; Siupsinskiene, N.; Staikuniene, J.; Ryskiene, S.; Lisauskaite, L.; Vaitkus, J. Translation, cross-cultural adaptation, and validation of the sino-nasal outcome test (SNOT)-22 for Lithuanian patients. Eur. Arch. Oto-Rhino-Laryngol. 2012, 270, 1843–1848. [Google Scholar] [CrossRef] [PubMed]
- Pettiford, J.N.; Jason, J.; Nwanyanwu, O.C.; Archibald, L.K.; Kazembe, P.N.; Dobbie, H.; Jarvis, W.R. Age-related differences in cell-specific cytokine production by acutely ill Malawian patients. Clin. Exp. Immunol. 2002, 128, 110–117. [Google Scholar] [CrossRef]
- Won, H.-K.; Kim, Y.-C.; Kang, M.-G.; Park, H.-K.; Lee, S.-E.; Kim, M.-H.; Yang, M.-S.; Chang, Y.-S.; Cho, S.-H.; Song, W.-J. Age-related prevalence of chronic rhinosinusitis and nasal polyps and their relationships with asthma onset. Ann. Allergy, Asthma Immunol. 2018, 120, 389–394. [Google Scholar] [CrossRef]
- Ms, C.A.L.; Soler, Z.M.; Bs, S.K.; Do, V.M.D.; Yoo, F.; Nguyen, S.A.; Schlosser, R.J. Revision surgery rates in chronic rhinosinusitis with nasal polyps: Meta-analysis of risk factors. Int. Forum Allergy Rhinol. 2020, 10, 199–207. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef]
- Ahern, S.; Cervin, A. Inflammation and Endotyping in Chronic Rhinosinusitis—A Paradigm Shift. Med. Kaunas Lith. 2019, 55, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morse, J.C.; Li, P.; Ely, K.A.; Shilts, M.H.; Wannemuehler, T.J.; Huang, L.C.; Sheng, Q.; Chowdhury, N.I.; Chandra, R.K.; Das, S.R.; et al. Chronic rhinosinusitis in elderly patients is associat-ed with an exaggerated neutrophilic proinflammatory response to pathogenic bacteria. J. Allergy Clin. Immunol. 2018, 143, 990–1002. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.H.; Kim, D.W.; Lee, S.H.; Kolliputi, N.; Hong, S.J.; Suh, L.; Norton, J.; Hulse, K.E.; Seshadri, S.; Conley, D.B.; et al. Age-Related Increased Prevalence of Asthma and Nasal Polyps in Chronic Rhinosinusitis and Its Association with Altered IL-6 Trans-Signaling. Am. J. Respir. Cell Mol. Biol. 2015, 53, 601–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, C.S.; Lee, H.S.; Kim, S.N.; Kim, J.H.; Park, D.-J.; Kim, K.-S. Prevalence and Risk Factors of Chronic Rhinosinusitis in the Elderly Population of Korea. Am. J. Rhinol. Allergy 2019, 33, 240–246. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | CRSwNP N = 59 (53.2%) | Control N = 52 (46.8%) | p Value |
|---|---|---|---|
| Age, mean ± SD, years | 50.3 ± 14.7 | 45.8 ± 19.5 | 0.177 * |
| Age groups, years | |||
| 18–30 | 5 (8.5) | 15 (28.8) | 0.02 |
| 31–50 | 22 (37.3) | 16 (30.8) | 0.235 |
| >51 | 32 (54.2) | 21 (40.4) | 0.072 |
| Sex | |||
| Male | 31 (52.5) | 28 (53.8) | 0.891 |
| Female | 28 (47.5) | 24 (46.2) | |
| Smoking status | |||
| Yes | 11 (18.6) | 4 (7.7) | 0.092 |
| Allergy | |||
| Yes | 15 (25.4) | 0 | <0.001 |
| Asthma | |||
| Yes | 18 (30.5) | 0 | <0.001 |
| Marker, pg/mL | Age Groups, Years | df = 2 χ2; p Value | ||
|---|---|---|---|---|
| 18–30 | 31–50 | >51 | ||
| IL-1 | 820.0 (367.7–1576.0) | 1181.6 (864–1489.2) | 1066.0 (719.3–1398.3) | 0.958; 0.619 |
| IL-2 | 509.1 (266.8–546.9) | 498.2 (213.1–518.2) | 477.1 (457.5–514.2) | 0.314; 0.855 |
| IL-4 | 169.7 (64.5–195.7) | 156.4 (110.5–231.2) | 212.7 (163.7–242.0) | 4.464; 0.107 |
| IL-5 | 97.2 (26.1–208.0) | 30.1 (28.2–136.4) | 29.9 (24.1–32.3) | 3.495; 0.174 |
| IL-6 | 208.3 (147.1–242.0) | 180.9 (150.3–233.5) | 209.0 (157.5–233.5) | 0.361; 0.835 |
| IL-7 | 22.8 (16.4–122.8) | 33.7 (29.4–123.4) | 29.9 (23.1–47.2) | 4.305; 0.116 |
| IL-10 | 190.1 (119.0–198.4) | 258.8 (171.4–396.7) | 233.9 (119.0–348.0) | 4.508; 0.105 |
| IL-13 | 165.2 (154.5–199.3) | 145.3 (121.4–168.2) | 160.2 (135.9–169.2) | 3.207; 0.201 |
| IL-21 | 109.6 (74.6–144.2) | 112.2 * (97.7–118.5) | 92.1* (71.0–105.6) | 6.29; 0.043; * p = 0.013 |
| IL-22 | 90.5 (75.1–167.1) | 132.8 (90.5–146.8) | 136.7 (115.5–167.5) | 1.73; 0.421 |
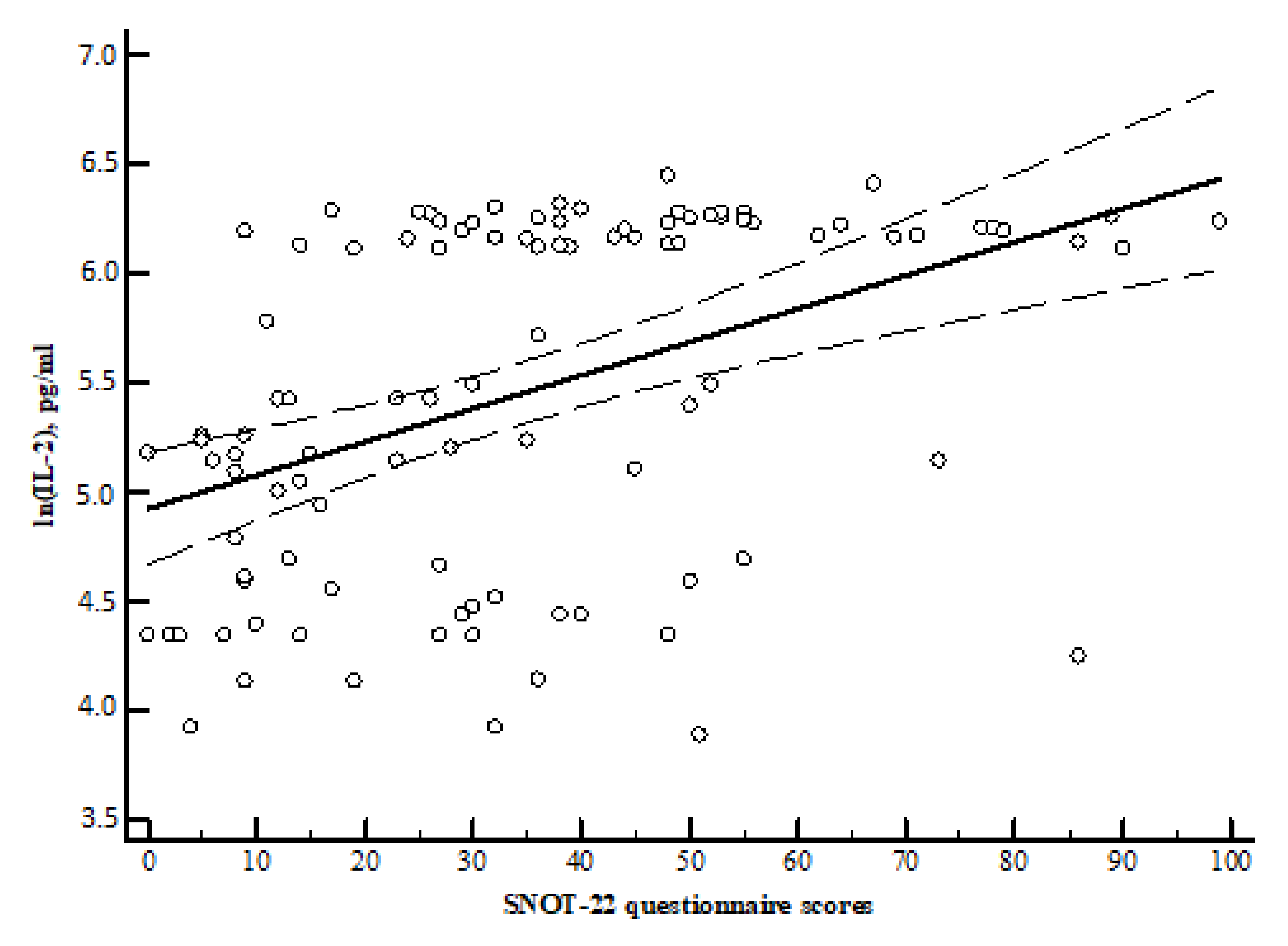
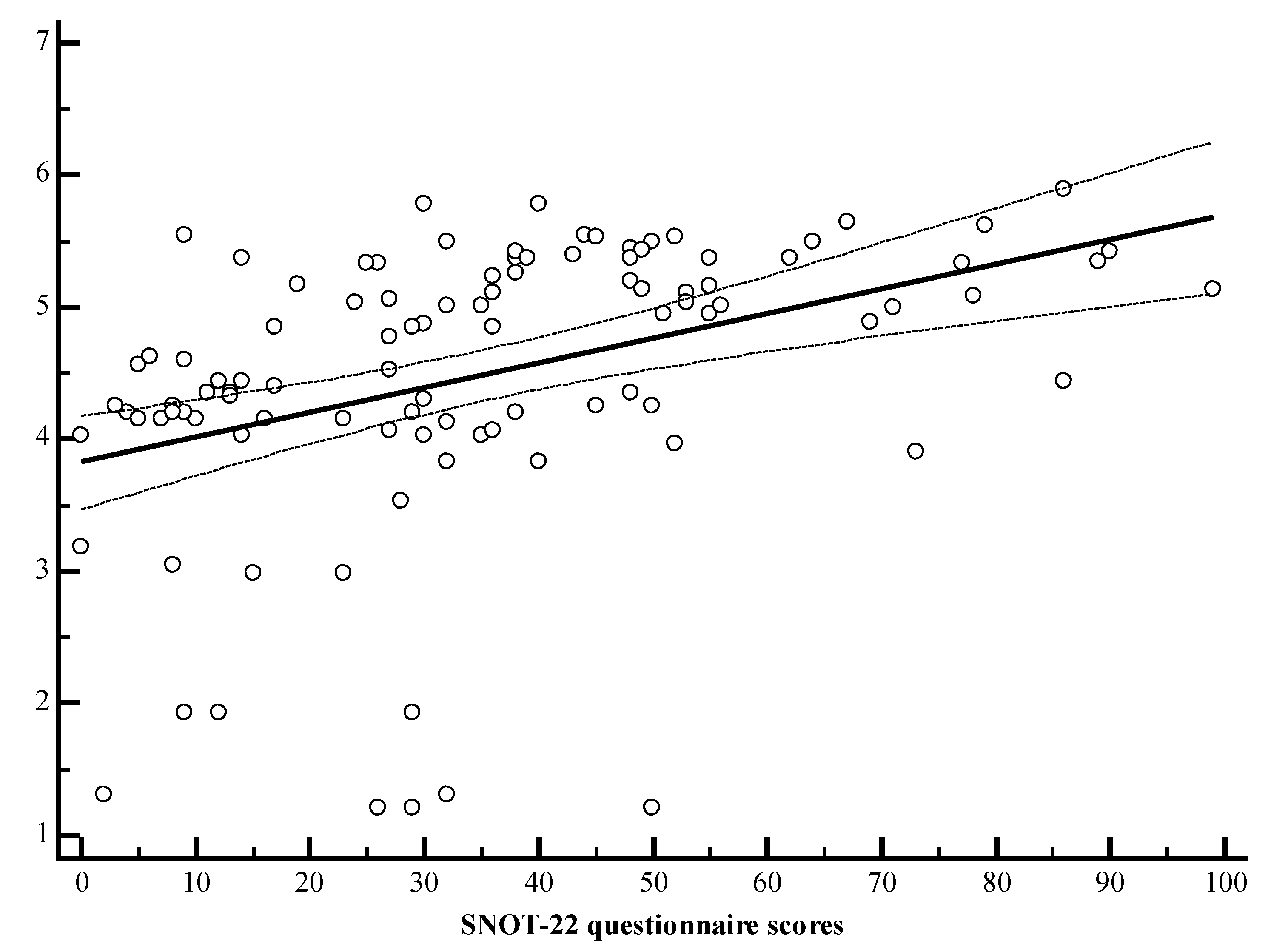
| The sum of the SNOT-22 Questionnaire Scores | Interleukins | ||
| IL-2 | IL-4 | IL-22 | |
| r = 0.464, p < 0.001 | r = 0.502, p < 0.001 | r = 0.521, p < 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaitkus, J.; Vitkauskienė, A.; Simuntis, R.; Vaitkus, Ž.; Šiupšinskienė, N.; Vaitkus, S. Chronic Rhinosinusitis with Nasal Polyps: Age and Disease Severity Differences in the Levels of Inflammatory Markers. Medicina 2021, 57, 282. https://doi.org/10.3390/medicina57030282
Vaitkus J, Vitkauskienė A, Simuntis R, Vaitkus Ž, Šiupšinskienė N, Vaitkus S. Chronic Rhinosinusitis with Nasal Polyps: Age and Disease Severity Differences in the Levels of Inflammatory Markers. Medicina. 2021; 57(3):282. https://doi.org/10.3390/medicina57030282
Chicago/Turabian StyleVaitkus, Justinas, Astra Vitkauskienė, Regimantas Simuntis, Žygimantas Vaitkus, Nora Šiupšinskienė, and Saulius Vaitkus. 2021. "Chronic Rhinosinusitis with Nasal Polyps: Age and Disease Severity Differences in the Levels of Inflammatory Markers" Medicina 57, no. 3: 282. https://doi.org/10.3390/medicina57030282