
Patient and Provider Perspective of Smart Wearable Technology in Diabetic Foot Ulcer Prevention: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
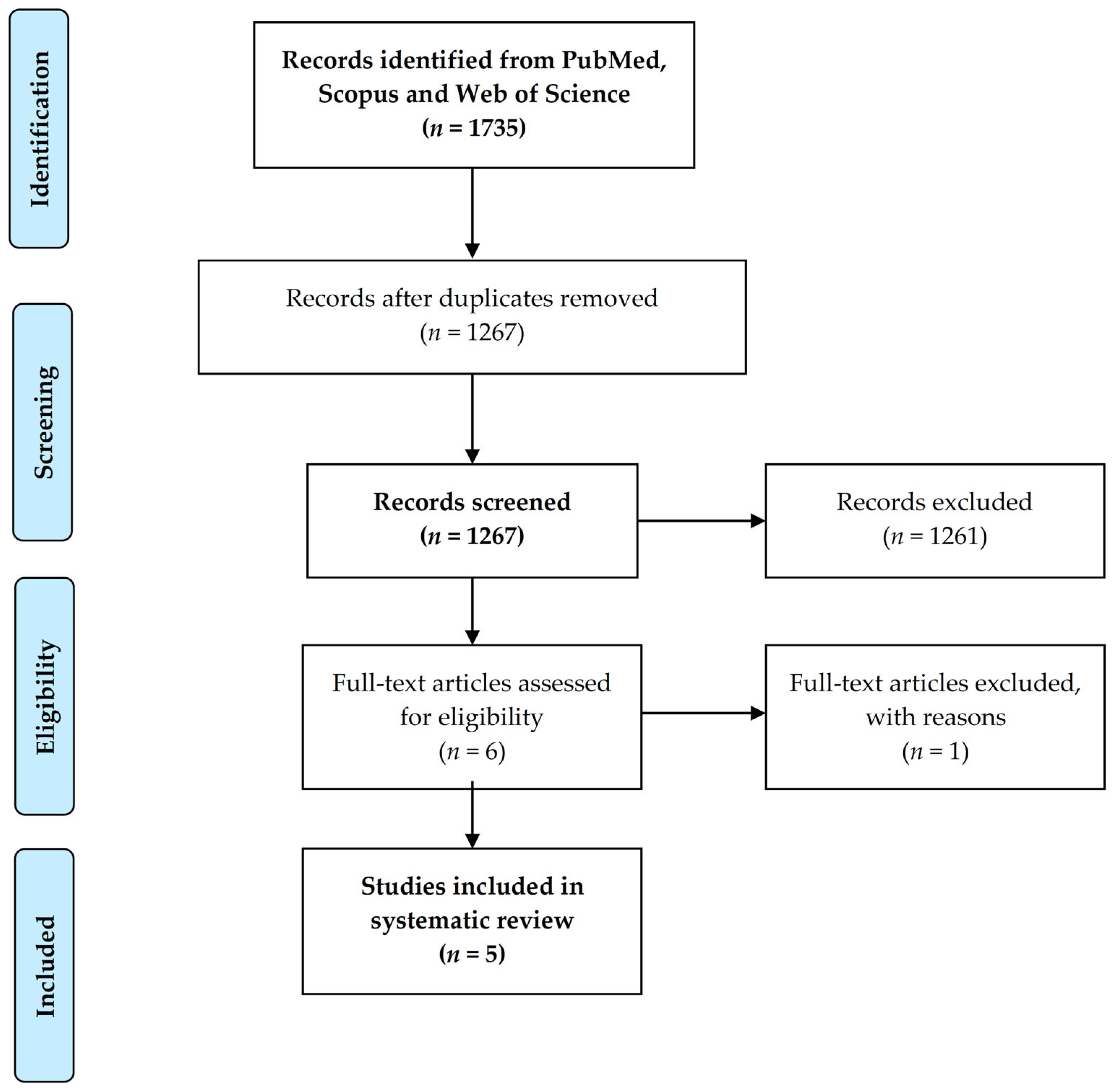
2.2. Study Selection
2.3. Data Extraction and Collection Process
2.4. Methodological Quality Evaluation
3. Results
3.1. Study Characteristics
3.2. Results of the Methodological Quality Assessment
3.3. Patient Perspective
3.4. Provider Perspectives
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Hex, N.; Bartlett, C.; Wright, D.; Taylor, M.; Varley, D. Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet. Med. 2012, 29, 855–862. [Google Scholar] [CrossRef]
- Kerr, M.; Barron, E.; Chadwick, P.; Evans, T.; Kong, W.M.; Rayman, G.; Sutton-Smith, M.; Todd, G.; Young, B.; Jeffcoate, W.J. The cost of diabetic foot ulcers and amputations to the National Health Service in England. Diabet. Med. 2019, 36, 995–1002. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, L.A.; Wrobel, J.S.; Vileikyte, L. Quality of Life in Healing Diabetic Wounds: Does the End Justify the Means? J. Foot Ankle Surg. 2008, 47, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Ismail, K.; Winkley, K.; Stahl, D.; Chalder, T.; Edmonds, M. A Cohort Study of People with Diabetes and Their First Foot Ulcer: The role of depression on mortality. Diabetes Care 2007, 30, 1473–1479. [Google Scholar] [CrossRef] [Green Version]
- Vileikyte, L.; Pouwer, F.; Gonzalez, J.S. Psychosocial research in the diabetic foot: Are we making progress? Diabetes/Metab. Res. Rev. 2020, 36, e3257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vileikyte, L.; Gonzalez, J.S.; Leventhal, H.; Peyrot, M.F.; Rubin, R.R.; Garrow, A.; Ulbrecht, J.S.; Cavanagh, P.R.; Boulton, A.J. Patient Interpretation of Neuropathy (PIN) Questionnaire: An instrument for assessment of cognitive and emotional factors associated with foot self-care. Diabetes Care 2006, 29, 2617–2624. [Google Scholar] [CrossRef] [Green Version]
- Perrin, B.M.; Swerissen, H.; Payne, C.B.; Skinner, T. Cognitive representations of peripheral neuropathy and self-reported foot-care behaviour of people at high risk of diabetes-related foot complications. Diabet. Med. 2013, 31, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Corbett, C.; Jolley, J.; Barson, E.; Wraight, P.; Perrin, B.; Fisher, C. Cognition and Understanding of Neuropathy of Inpatients Admitted to a Specialized Tertiary Diabetic Foot Unit with Diabetes-Related Foot Ulcers. Int. J. Low. Extrem. Wounds 2019, 18, 294–300. [Google Scholar] [CrossRef]
- Iversen, M.M.; Tell, G.S.; Espehaug, B.; Midthjell, K.; Graue, M.; Rokne, B.; Berge, L.I.; Østbye, T. Is depression a risk factor for diabetic foot ulcers? 11-years follow-up of the Nord-Trøndelag Health Study (HUNT). J. Diabetes Its Complicat. 2015, 29, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.S.; Vileikyte, L.; Ulbrecht, J.S.; Rubin, R.R.; Garrow, A.P.; Delgado, C.; Cavanagh, P.R.; Boulton, A.J.M.; Peyrot, M. Depression predicts first but not recurrent diabetic foot ulcers. Diabetologia 2010, 53, 2241–2248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, L.H.; Rutter, C.M.; Katon, W.J.; Reiber, G.E.; Ciechanowski, P.; Heckbert, S.R.; Lin, E.H.; Ludman, E.J.; Oliver, M.M.; Young, B.A.; et al. Depression and Incident Diabetic Foot Ulcers: A Prospective Cohort Study. Am. J. Med. 2010, 123, 748–754.e3. [Google Scholar] [CrossRef] [Green Version]
- Murphy, P.T.; Liew, A.; McGuire, B.E.; Bogue, J.; Pilch, M.; Dinneen, S.; O’Loughlin, A.; Doherty, A.; Conneely, S. Do personality and mood difficulties predict foot self-care in diabetes? J. Wound Manag. Off. J. Eur. Wound Manag. Assoc. 2021, 22, 43–54. [Google Scholar] [CrossRef]
- Kloos, C.; Hagen, F.; Lindloh, C.; Braun, A.; Leppert, K.; Müller, N.; Wolf, G.; Müller, U.A. Cognitive Function Is Not Associated with Recurrent Foot Ulcers in Patients With Diabetes and Neuropathy. Diabetes Care 2009, 32, 894–896. [Google Scholar] [CrossRef] [Green Version]
- Westby, M.; Norman, G.; Vedhara, K.; Game, F.; Cullum, N. Psychosocial and behavioural prognostic factors for diabetic foot ulcer development and healing: A systematic review. Diabet. Med. 2020, 37, 1244–1255. [Google Scholar] [CrossRef]
- Lincoln, N.B.; Radford, K.; Game, F.L.; Jeffcoate, W.J. Education for secondary prevention of foot ulcers in people with diabetes: A randomised controlled trial. Diabetologia 2008, 51, 1954–1961. [Google Scholar] [CrossRef]
- Gershater, M.A.; Pilhammar, E.; Apelqvist, J.; Alm-Roijer, C. Patient education for the prevention of diabetic foot ulcers. Eur. Diabetes Nurs. 2011, 8, 102–107b. [Google Scholar] [CrossRef]
- Abbott, C.A.; Chatwin, K.E.; Foden, P.; Hasan, A.N.; Sange, C.; Rajbhandari, S.M.; Reddy, P.N.; Vileikyte, L.; Bowling, F.L.; Boulton, A.J.M.; et al. Innovative intelligent insole system reduces diabetic foot ulcer recurrence at plantar sites: A prospective, randomised, proof-of-concept study. Lancet Digit. Health 2019, 1, e308–e318. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Mishra, R. Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review. Medicina 2021, 57, 377. [Google Scholar] [CrossRef]
- Najafi, B.; Reeves, N.D.; Armstrong, D.G. Leveraging smart technologies to improve the management of diabetic foot ulcers and extend ulcer-free days in remission. Diabetes Metab. Res. Rev. 2020, 36, e3239. [Google Scholar] [CrossRef] [Green Version]
- Hazenberg, C.E.V.B.; De Stegge, W.B.A.; Van Baal, S.G.; Moll, F.L.; Bus, S.A. Telehealth and telemedicine applications for the diabetic foot: A systematic review. Diabetes/Metabolism Res. Rev. 2020, 36, e3247. [Google Scholar] [CrossRef]
- Foong, H.F.; Kyaw, B.M.; Upton, Z.; Car, L.T. Facilitators and barriers of using digital technology for the management of diabetic foot ulcers: A qualitative systematic review. Int. Wound J. 2020, 17, 1266–1281. [Google Scholar] [CrossRef] [PubMed]
- Tchero, H.; Noubou, L.; Becsangele, B.; Mukisi-Mukaza, M.; Retali, G.-R.; Rusch, E. Telemedicine in Diabetic Foot Care: A Systematic Literature Review of Interventions and Meta-analysis of Controlled Trials. Int. J. Low. Extrem. Wounds 2017, 16, 274–283. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Sirriyeh, R.R.; Lawton, R.; Gardner, P.; Armitage, G.R. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pr. 2011, 18, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Novice, T.; Vemuri, C.; Gilbert, C.; Fici, A.; VanWieren, E.; Schmidt, B.M. Do Patients with Diabetes Mellitus Want Wearable Technology to Prevent Diabetic Foot Ulcers? J. Diabetes Sci. Technol. 2019, 13, 799–800. [Google Scholar] [CrossRef]
- Najafi, B.; Ron, E.; Enriquez, A.; Marin, I.; Razjouyan, J.; Armstrong, D.G. Smarter Sole Survival: Will Neuropathic Patients at High Risk for Ulceration Use a Smart Insole-Based Foot Protection System? J. Diabetes Sci. Technol. 2017, 11, 702–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyzelman, A.M.; Koelewyn, K.; Murphy, M.; Shen, X.; Yu, E.; Pillai, R.; Fu, J.; Scholten, H.J.; Ma, R. Continuous Temperature-Monitoring Socks for Home Use in Patients with Diabetes: Observational Study. J. Med. Internet. Res. 2018, 20, e12460. [Google Scholar] [CrossRef] [Green Version]
- Macdonald, E.M.; Perrin, B.M.; Hyett, N.; Kingsley, M.I.C. Factors influencing behavioural intention to use a smart shoe insole in regionally based adults with diabetes: A mixed methods study. J. Foot Ankle Res. 2019, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, E.; Perrin, B.; Cleeland, L.; Kingsley, M. Podiatrist-Delivered Health Coaching to Facilitate the Use of a Smart Insole to Support Foot Health Monitoring in People with Diabetes-Related Peripheral Neuropathy. Sensors 2021, 21, 3984. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, E.M.; Perrin, B.M.; Kingsley, M.I.C. Factors influencing Australian podiatrists’ behavioural intentions to adopt a smart insole into clinical practice: A mixed methods study. J. Foot Ankle Res. 2020, 13, 28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Study Design | Participants | Clinical Condition | Sample Size | Type of Device | Data Collection Tools | Main Findings |
|---|---|---|---|---|---|---|---|
| Najafi et al. [29] | Quantitative | Patients | DPN | 17 | Insoles | Questionnaires | The device and smartwatch were considered easy to use and effective by the patients. A high level of satisfaction was reported. More frequent pressure alerts were associated with better adherence, improvement in offloading, and greater satisfaction with the device. |
| Reyzelman et al. [30] | Quantitative | Patients | DPN with and without a history of DFU | 35 | Socks | Questionnaires | Patients described the socks as useful, comfortable, well-designed, and easy to wear. The mobile application was easy to use. Patients were highly satisfied with the device and mobile application. |
| Macdonald et al. [31] | Mixed | Patients | Diabetic patients with and without a history of DFU | 53 | Insoles | Questionnaires/focus groups | Attitude, self-efficacy, performance expectancy, and effort expectancy were predictors of the patients’ behavioural intention to use an insole system. |
| Macdonald et al. [33] | Mixed | Podiatrists | - | 111 | Insoles | Questionnaires/focus groups | Podiatrists considered the insole device as a useful tool for monitoring diabetic foot disease. Performance expectancy was the main predictor of the intention to use the device in clinical practice. Providers raised several concerns about the cost, type of footwear, and functionality of the insole device with elderly and remote populations. |
| Macdonald et al. [32] | Mixed | Patients/Podiatrists | DPN | 10/2 | Insoles | Questionnaires/focus groups | Patient perspective: Performance expectancy, attitude, and behaviour intention decreased significantly after 4 weeks of intervention. The patients were particularly concerned about alert intrusiveness and restricted choice of footwear. Although they appreciated the potential benefits of the smart insole, they did not intend to adopt its current version in the future. Provider perspective: Patients’ negative experiences with the insole device negatively impacted the podiatrists’ view of the device. Although the device was regarded as being useful for foot monitoring, podiatrists were of the opinion that its performance and usability require several improvements. |
| Criteria (Score: 0 to 3 Points) | Quantitative Studies [29,30] (Mean Values) | Mixed Studies [31,32,33] (Mean Values) |
|---|---|---|
| Explicit theoretical framework | 1.5 | 3 |
| Statement of aims/objectives in main body of report | 2.25 | 2.7 |
| Clear description of research setting | 2.25 | 1.5 |
| Evidence of sample size considered in terms of analysis | 0.25 | 1.3 |
| Representative sample of target group of a reasonable size | 0.75 | 1.3 |
| Description of procedure for data collection | 1.75 | 2.5 |
| Rationale for choice of data collection tool(s) | 2 | 3 |
| Detailed recruitment data | 0.75 | 1.3 |
| Statistical assessment of reliability and validity of measurement tool(s) (Quantitative only) | 0.75 | 1.3 |
| Fit between stated research question and method of data collection (Quantitative only) | 1.75 | 2.7 |
| Fit between stated research question and format and content of data collection tool e.g., interview schedule (Qualitative only) | - | 2.5 |
| Fit between research question and method of analysis (Quantitative only) | 1.5 | 3 |
| Good justification for analytic method selected | 1.25 | 2 |
| Assessment of reliability of analytic process (Qualitative only) | - | 2.5 |
| Evidence of user involvement in design | 0 | 0 |
| Strengths and limitations critically discussed | 1.5 | 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlando, G.; Prior, Y.; Reeves, N.D.; Vileikyte, L. Patient and Provider Perspective of Smart Wearable Technology in Diabetic Foot Ulcer Prevention: A Systematic Review. Medicina 2021, 57, 1359. https://doi.org/10.3390/medicina57121359
Orlando G, Prior Y, Reeves ND, Vileikyte L. Patient and Provider Perspective of Smart Wearable Technology in Diabetic Foot Ulcer Prevention: A Systematic Review. Medicina. 2021; 57(12):1359. https://doi.org/10.3390/medicina57121359
Chicago/Turabian StyleOrlando, Giorgio, Yeliz Prior, Neil D. Reeves, and Loretta Vileikyte. 2021. "Patient and Provider Perspective of Smart Wearable Technology in Diabetic Foot Ulcer Prevention: A Systematic Review" Medicina 57, no. 12: 1359. https://doi.org/10.3390/medicina57121359