
Association of ABO Blood Type with Bleeding Severity in Patients with Acute Gastroesophageal Variceal Bleeding

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Materials and Methods
2.1. Study Design and Setting
2.2. Variables
2.3. Statistical Analysis
3. Results
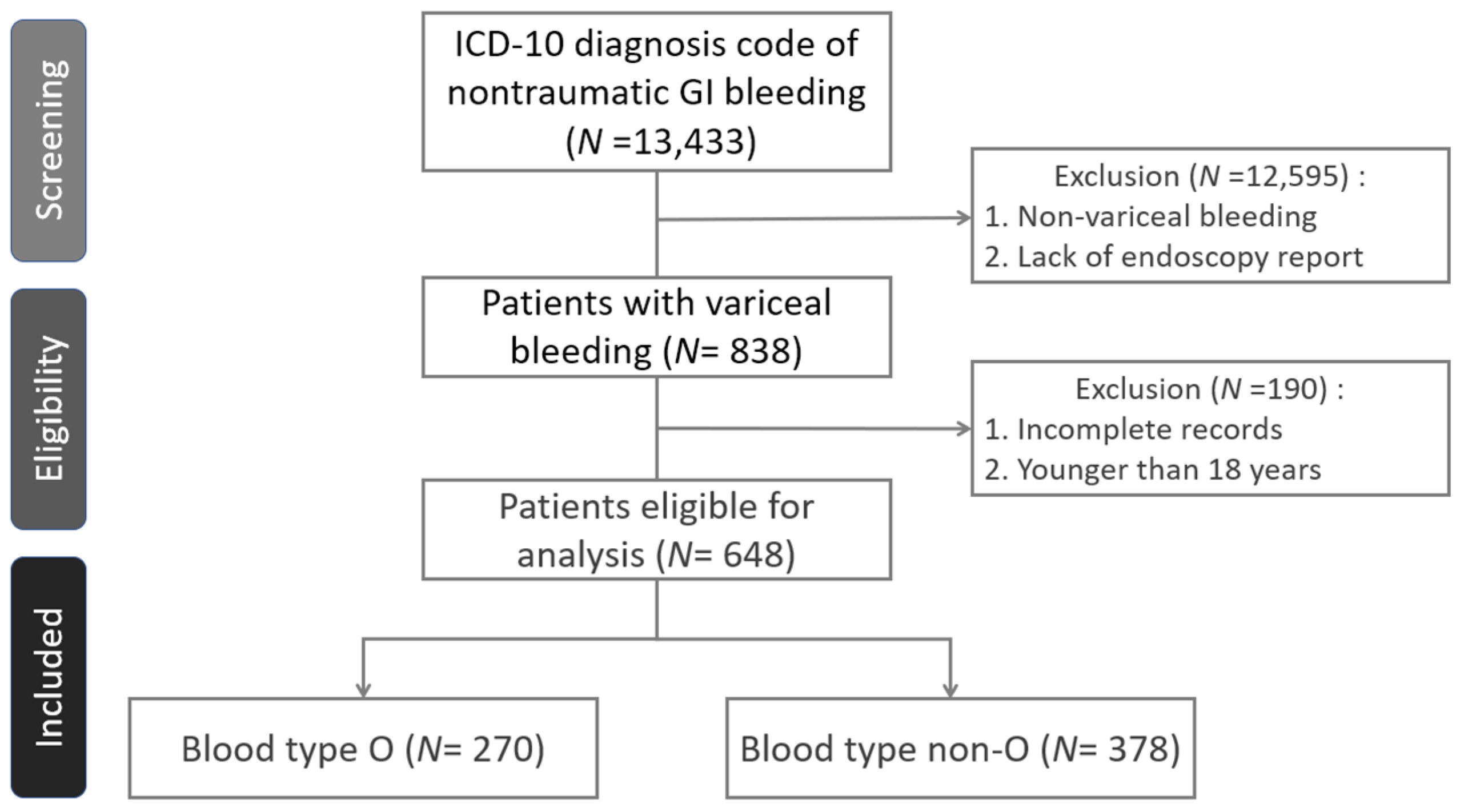
3.1. Participants
3.2. Endoscopic Findings and Treatment
3.3. Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blatchford, O.; Davidson, L.A.; Murray, W.R.; Blatchford, M.; Pell, J. Acute upper gastrointestinal haemorrhage in west of Scotland: Case ascertainment study. BMJ 1997, 315, 510–514. [Google Scholar] [CrossRef]
- Sostres, C.; Lanas, A. Epidemiology and demographics of upper gastrointestinal bleeding: Prevalence, incidence, and mortality. Gastrointest. Endosc. Clin. N. Am. 2011, 21, 567. [Google Scholar] [CrossRef]
- Rockall, T.A.; Logan, R.F.; Devlin, H.B.; Northfield, T.C. Incidence of and mortality from acute upper gastrointestinal hemorrhage in the United Kingdom: Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ 1995, 311, 222. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-Y.; Wu, C.-H.; Wu, M.-S.; Wang, C.-B.; Cheng, J.-S.; Kuo, K.N.; Lin, J.-T. A Nationwide Population-Based Cohort Study Shows Reduced Hospitalization for Peptic Ulcer Disease Associated with H pylori Eradication and Proton Pump Inhibitor Use. Clin. Gastroenterol. Hepatol. 2009, 7, 427–431. [Google Scholar] [CrossRef]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef]
- Rudler, M.; Rousseau, G.; Benosman, H.; Massard, J.; Deforges, L.; Lebray, P.; Poynard, T.; Thabut, D. Peptic ulcer bleeding in patients with or without cirrhosis: Different diseases but the same prognosis? Aliment. Pharmacol. Ther. 2012, 36, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Carbonell, N.; Pauwels, A.; Serfaty, L.; Fourdan, O.; Lévy, V.G.; Poupon, R. Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Hepatology 2004, 40, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Smith, J. The course of patients after variceal hemorrhage. Gastroenterology 1981, 80, 800–809. [Google Scholar] [CrossRef]
- Koransky, J.R.; Galambos, J.T.; Hersh, T.; Warren, W.D. The mortality of bleeding esophageal varices in a private university hospital. Am. J. Surg. 1978, 136, 339–341. [Google Scholar] [CrossRef]
- North Italian Endoscopic Club for the Study and Treatment of Esophageal Varices. Prediction of the first variceal hemorrhage in patients with cirrhosis of the liver and esophageal varices. A prospective multicenter study. N. Engl. J. Med. 1988, 319, 983–989. [CrossRef]
- Beppu, K.; Inokuchi, K.; Koyanagi, N.; Nakayama, S.; Sakata, H.; Kitano, S.; Kobayashi, M. Prediction of variceal hemorrhage by esophageal endoscopy. Gastrointest. Endosc. 1981, 27, 213–218. [Google Scholar] [CrossRef]
- Merli, M.; Nicolini, G.; Angeloni, S.; Rinaldi, V.; De Santis, A.; Merkel, C.; Attili, A.F.; Riggio, O. Incidence and natural history of small esophageal varices in cirrhotic patients. J. Hepatol. 2003, 38, 266–272. [Google Scholar] [CrossRef]
- Sarin, S.K.; Lahoti, D.; Saxena, S.P.; Murthy, N.S.; Makwana, U.K. Prevalence, classification and natural history of gastric varices: A long-term follow-up study in 568 portal hypertension patients. Hepatology 1992, 16, 1343–1349. [Google Scholar] [CrossRef]
- Kim, T.; Shijo, H.; Kokawa, H.; Tokumitsu, H.; Kubara, K.; Ota, K.; Akiyoshi, N.; Iida, T.; Yokoyama, M.; Okumura, M. Risk factors for hemorrhage from gastric fundal varices. Hepatology 1997, 25, 307. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, J.; Laffan, M.A. The relationship between ABO histo-blood group, factor VIII and von Willebrand factor. Transfus. Med. 2001, 11, 343–351. [Google Scholar] [CrossRef]
- Moeller, A.; Weippert-Kretschmer, M.; Prinz, H.; Kretschmer, V. Influence of ABO blood groups on primary hemostasis. Transfusion 2001, 41, 56–60. [Google Scholar] [CrossRef]
- Dentali, F.; Sironi, A.P.; Ageno, W.; Turato, S.; Bonfanti, C.; Frattini, F.; Crestani, S.; Franchini, M. Non-O Blood Type Is the Commonest Genetic Risk Factor for VTE: Results from a Meta-Analysis of the Literature. Semin. Thromb. Hemost. 2012, 38, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Brocco, G.; Manzato, F.; Lippi, G. Influence of the ABO blood type on the platelet function analyzer PFA-100. Thromb. Haemost. 2001, 85, 369–370. [Google Scholar] [CrossRef]
- Massimo, F.; Giuseppe, L. Relative risks of thrombosis and bleeding in different ABO blood groups. Semin. Thromb. Hemost. 2016, 42, 112–117. [Google Scholar]
- Horwich, L.; Evans, D.A.; McConnell, R.B.; Donohoe, W.T. ABO blood groups in gastric bleeding. Gut 1966, 7, 680–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.A.; Horwich, L.; McConnell, R.B.; Bullen, M.F. Influence of the ABO blood groups and secretor status on bleeding and on perforation of duodenal ulcer. Gut 1968, 9, 319–322. [Google Scholar] [CrossRef] [Green Version]
- Bayan, K.; Tüzün, Y.; Yılmaz, Ş.; Dursun, M.; Canoruc, F. Clarifying the Relationship Between ABO/Rhesus Blood Group Antigens and Upper Gastrointestinal Bleeding. Dig. Dis. Sci. 2008, 54, 1029–1034. [Google Scholar] [CrossRef]
- Bahardoust, M.; Naghshin, R.; Mokhtare, M.; Hejrati, A.; Namdar, P.; Talebi, A.; Tavakoli, T.; Amiri, H.; Kiapey, S.H. Association between ABO Blood Group and Clinical Outcomes in Patients with Gastrointestinal Bleeding. Intern. Med. 2018, 8, 1. [Google Scholar]
- Chauleur, C.; Cochery-Nouvellon, E.; Mercier, E.; Aya, G.; Fabbro-Peray, P.; Mismetti, P.; Lissade-Lavigne, G.; Gris, J.-C. Some hemostasis variables at the end of the population distributions are risk factors for severe postpartum hemorrhages. J. Thromb. Haemost. 2008, 6, 2067–2074. [Google Scholar] [CrossRef] [PubMed]
- Takayama, W.; Endo, A.; Koguchi, H.; Sugimoto, M.; Murata, K.; Otomo, Y. The impact of blood type O on mortality of severe trauma patients: A retrospective observational study. Crit. Care 2018, 22, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, J.G.; Greenberg, C.S.; Patton, H.M.; Caldwell, S.H. AGA Clinical Practice Update: Coagulation in Cirrhosis. Gastroenterology 2019, 157, 34–43.e1. [Google Scholar] [CrossRef] [PubMed]
- Lisman, T.; Bongers, T.N.; Adelmeijer, J.; Janssen, H.L.; De Maat, M.P.; De Groot, P.G.; Leebeek, F.W. Elevated levels of von Willebrand Factor in cirrhosis support platelet adhesion despite reduced functional capacity. Hepatology 2006, 44, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, A.; Primignani, M.; Lemma, L.; Chantarangkul, V.; Mannucci, P.M. Evidence that low protein C contributes to the procoagulant imbalance in cirrhosis. J. Hepatol. 2013, 59, 265–270. [Google Scholar] [CrossRef]
- Sinegre, T.; Duron, C.; Lecompte, T.; Pereira, B.; Massoulier, S.; Lamblin, G.; Abergel, A.; Lebreton, A. Increased factor VIII plays a significant role in plasma hypercoagulability phenotype of patients with cirrhosis. J. Thromb. Haemost. 2018, 16, 1132–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Franchis, R. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laine, L.; Spiegel, B.; Rostom, A.; Moayyedi, P.; Kuipers, E.J.; Bardou, M.; Sung, J.J.Y.; Barkun, A.N. Methodology for Randomized Trials of Patients With Nonvariceal Upper Gastrointestinal Bleeding: Recommendations From an International Consensus Conference. Am. J. Gastroenterol. 2010, 105, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Elsebaey, M.A.; Elashry, H.; Elbedewy, T.A.; Elhadidy, A.A.; Esheba, N.; Ezat, S.; Negm, M.S.; Abo-Amer, Y.E.-E.; El Abgeegy, M.; Elsergany, H.F.; et al. Predictors of in-hospital mortality in a cohort of elderly Egyptian patients with acute upper gastrointestinal bleeding. Medicine 2018, 97, e0403. [Google Scholar] [CrossRef]
- Hanafy, A.S.; Badawi, R.; Basha, M.A.A.; Selim, A.; Yousef, M.; Elnawasany, S.; Mansour, L.; Elkhouly, R.A.; Hawash, N.; Abd-Elsalam, S. A novel scoring system for prediction of esophageal varices in critically ill patients. Clin. Exp. Gastroenterol. 2017, 10, 315–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.S.; Choi, J.; Shin, W.C. AIMS65 scoring system is comparable to Glasgow-Blatchford score or Rockall score for prediction of clinical outcomes for non-variceal upper gastrointestinal bleeding. BMC Gastroenterol. 2019, 19, 136. [Google Scholar] [CrossRef] [Green Version]
- Bangaru, S.; Benhammou, J.N.; Tabibian, J.H. Noninvasive scores for the prediction of esophageal varices and risk stratification in patients with cirrhosis. World J. Hepatol. 2020, 12, 908–918. [Google Scholar] [CrossRef] [PubMed]
- ElSebaey, M.A.; Tawfik, M.A.; Ezzat, S.; Selim, A.; Elashry, H.; Abd-Elsalam, S. Endoscopic injection sclerotherapy versus N-Butyl-2 Cyanoacrylate injection in the management of actively bleeding esophageal varices: A randomized controlled trial. BMC Gastroenterol. 2019, 19, 23. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number of ER Visits | Total Patient Number (N = 327) |
|---|---|
| 1 | 179 |
| 2 | 69 |
| 3 | 36 |
| 4 | 20 |
| 5 | 10 |
| 6 | 4 |
| 7 | 5 |
| 8 | 2 |
| 9 | 2 |
| Total Patient Number | Total (N = 327) | Type O (N = 142) | Type Non-O (N = 185) | p Value |
|---|---|---|---|---|
| Characteristics | ||||
| Age mean ± SD—years | 63.09 ± 15.12 | 64.2 ± 12.30 | 65.1 ± 13.39 | 0.516 |
| Male sex–no. (%) | 219 (67.0) | 98 (69.0) | 121 (65.4) | 0.569 |
| Coexisting diseases–no. (%) | ||||
| Hypertension (%) | 77 (23.5) | 31 (21.8) | 46 (24.9) | 0.611 |
| Diabetes mellitus (%) | 112 (34.3) | 53 (37.3) | 59 (31.9) | 0.422 |
| End-stage renal disease with hemodialysis (%) | 22 (6.7) | 11 (7.7) | 11 (5.9) | * |
| Hepatoma (%) | 127 (38.8) | 49 (34.5) | 78 (42.2) | 0.196 |
| Total Patient ER visits | Total (N = 648) | Type O (N = 270) | Type non-O (N = 378) | p Value |
| Initial data on admission | ||||
| Hemoglobin level ± SD—g/dL | 8.83 ± 2.61 | 8.98 ± 2.45 | 8.73 ± 2.24 | 0.271 |
| Platelet count ± SD—103/µL | 120 ± 79.24 | 124.88 ± 92.73 | 116.58 ± 74.19 | 0.613 |
| Prothrombin time ± SD—seconds | 16.1 ± 4.40 (1.46 ± 0.38) | 16.12 ± 4.33 (1.47 ± 0.42) | 16.08 ± 5.16 (1.45 ± 0.39) | 0.598 (0.926) |
| Systolic blood pressure ± SD—mmHg | 125.2 ± 28.6 | 127.0 ± 25.6 | 124.0 ± 25.1 | 0.123 |
| Systolic blood pressure < 90 mmHg–no. (%) | 96 (14.8) | 38 (14.1) | 58 (15.3) | 0.705 |
| Mean blood pressure ± SD—mmHg | 90.28 ± 20.5 | 91.9 ± 19.1 | 89.1 ± 17.9 | 0.072 |
| Mean blood pressure < 65 mmHg–no. (%) | 42 (6.5) | 20 (7.4) | 22 (5.8) | 0.420 |
| Heart rate–beats/min | 98.16 (23.47) | 97.92 | 98.32 | 0.859 |
| Heart rate > 100 beats/min–no. (%) | 306 (47.2) | 133 (49.3) | 173 (45.8) | 0.445 |
| Child-Pugh Score (Level)–no. (%) | 0.845 | |||
| 5 to 6 (A) | 223 (36.0) | 89 (32.9) | 146 (38.6) | |
| 7 to 9 (B) | 298 (46.0) | 122 (45.3) | 174 (46.1) | |
| 10 to 15 (C) | 117 (18.1) | 59 (21.9) | 58 (15.3) | |
| Risk factors for bleeding | ||||
| Aspirin or clopidogrel use (%) | 14 (2.2) | 7 (2.6) | 7 (1.9) | * |
| Warfarin or direct oral anticoagulant use (%) | 3 (0.5) | 2 (0.7) | 1 (0.3) | * |
| Characteristics | Total (N = 648) | Type O (N = 270) | Type Non-O (N = 378) | p Value |
|---|---|---|---|---|
| Gastroesophageal varices appearance | ||||
| White nipple sign (%) | 23 (3.5) | 10 (3.7) | 13 (3.4) | * |
| Red color sign, active bleeding (%) | 299 (46.1) | 123 (45.6) | 176 (46.6) | 0.459 |
| Endoscopic treatment | ||||
| Rubber ligation (%) | 302 (46.6) | 124 (45.9) | 178 (47.1) | 0.668 |
| Histoacryl injection (%) | 43 (6.6) | 17 (6.3) | 26 (6.9) | * |
| S-B tube insertion (%) | 17 (2.6) | 8 (3.0) | 9 (2.4) | * |
| Mortality | Total (N = 327) | Type O (N = 142) | Type Non-O (N = 185) | p Value |
|---|---|---|---|---|
| All-cause in-hospital mortality–no. (%) | 46 (14.1) | 16 (11.2) | 30 (16.2) | 0.265 |
| All-cause 7-day mortality–no. (%) | 13 (4.0) | 4 (2.8) | 9 (4.9) | 0.306 |
| All-cause 30-day mortality–no. (%) | 51 (15.6) | 21 (14.8) | 30 (16.2) | 0.532 |
| Total (N = 648) | Type O (N = 270) | Type Non-O (N = 378) | p Value | |
|---|---|---|---|---|
| ICU admission–no. (%) | 52 (8) | 21 (7.8) | 31 (8.9) | 0.857 |
| Admission days ± SD | 8.37 ± 7.2 | 8.31 ± 11.68 | 7.38 ± 7.52 | 0.832 |
| Further bleeding | ||||
| Further bleeding confirmed by PES in 7 days (%) | 37 (5.7) | 21 (7.8) | 16 (4.2) | 0.408 |
| Further bleeding confirmed by PES in 30 days (%) | 59 (9.1) | 34 (12.6) | 25 (6.9) | 0.539 |
| Pack RBC transfusion amount | 2.16 ± 2.37 | 1.96 ± 2.25 | 2.31 ± 2.26 | 0.071 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, W.-Y.; Hong, M.-Y.; Lin, C.-H.; Chang, P.-P.; Chu, S.-C.; Kao, C.-L. Association of ABO Blood Type with Bleeding Severity in Patients with Acute Gastroesophageal Variceal Bleeding. Medicina 2021, 57, 1323. https://doi.org/10.3390/medicina57121323
Lin W-Y, Hong M-Y, Lin C-H, Chang P-P, Chu S-C, Kao C-L. Association of ABO Blood Type with Bleeding Severity in Patients with Acute Gastroesophageal Variceal Bleeding. Medicina. 2021; 57(12):1323. https://doi.org/10.3390/medicina57121323
Chicago/Turabian StyleLin, Wei-Yu, Ming-Yuan Hong, Chih-Hao Lin, Peng-Peng Chang, Shao-Chung Chu, and Chia-Lung Kao. 2021. "Association of ABO Blood Type with Bleeding Severity in Patients with Acute Gastroesophageal Variceal Bleeding" Medicina 57, no. 12: 1323. https://doi.org/10.3390/medicina57121323