
Complex Regional Pain Syndrome in Athletes: Scoping Review

 , , ,
, , ,
Abstract
:1. Introduction
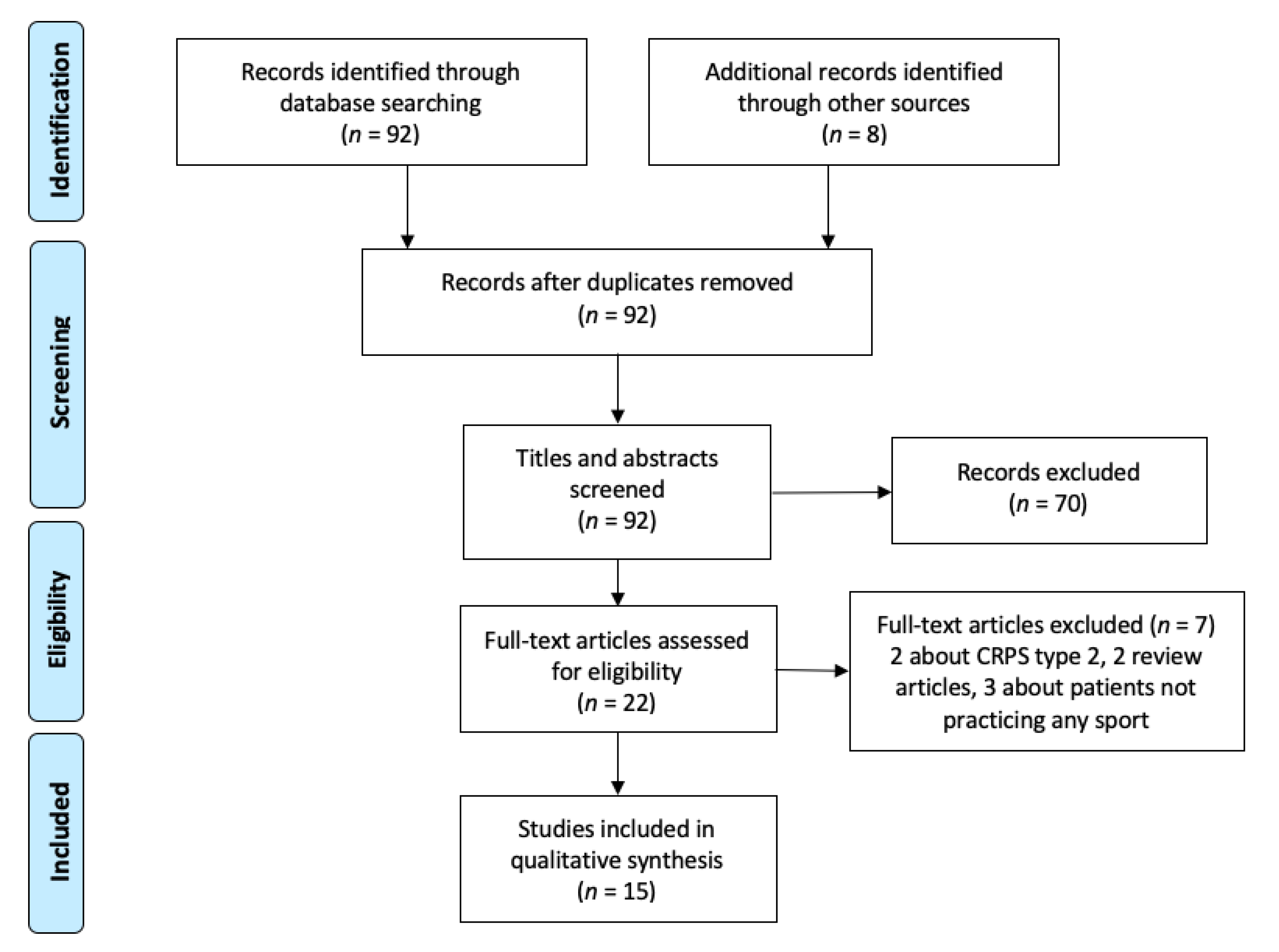
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iolascon, G.; Tarantino, U. Rare diseases in orthopedics: Algodystrophy and aseptic osteonecrosis. Clin. Cases Miner. Bone Metab. 2015, 12 (Suppl. S1), 2–3. [Google Scholar]
- Iolascon, G.; de Sire, A.; Moretti, A.; Gimigliano, F. Complex regional pain syndrome (CRPS) type I: Historical perspective and critical issues. Clin. Cases Miner. Bone Metab. 2015, 12 (Suppl. S1), 4–10. [Google Scholar] [CrossRef]
- De Sire, A.; Paoletta, M.; Moretti, A.; Brandi, M.L.; Iolascon, G. Complex regional pain syndrome: Facts on causes, diagnosis and therapy. Clin. Cases Miner. Bone Metab. 2018, 15, 166–172. [Google Scholar] [CrossRef]
- Goebel, A.; Birklein, F.; Brunner, F.; Clark, J.D.; Gierthmühlen, J.; Harden, N.; Huygen, F.; Knudsen, L.; McCabe, C.; Lewis, J.; et al. The Valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain 2021, 15. [Google Scholar] [CrossRef]
- Gierthmühlen, J.; Binder, A.; Baron, R. Mechanism-based treatment in complex regional pain syndromes. Nat. Rev. Neurol. 2014, 10, 518–528. [Google Scholar] [CrossRef]
- Chang, C.; McDonnell, P.; Gershwin, M.E. Complex regional pain syndrome - Autoimmune or functional neurologic syndrome. J. Transl. Autoimmun. 2020, 4, 100080. [Google Scholar] [CrossRef]
- Rand, S.E.; Basu, S.; Khalid, S. Complex Regional Pain Syndrome: Current Diagnostic and Treatment Considerations. Curr. Sports Med. Rep. 2019, 18, 325–329. [Google Scholar] [CrossRef]
- Harden, N.R.; Bruehl, S.; Perez, R.S.; Birklein, F.; Marinus, J.; Maihofner, C.; Lubenow, T.R.; Buvanendran, A.; Mackey, S.; Graciosa, J.R.; et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain 2010, 150, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Bruehl, S. Complex regional pain syndrome. BMJ 2015, 351, h2730. [Google Scholar] [CrossRef] [Green Version]
- Small, E. Chronic musculoskeletal pain in young athletes. Pediatric Clin. N. Am. 2002, 49, 655–662. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Carayannopoulos, A.G.; Cravero, J.P.; Stinson, M.T.; Sites, B.D. Use of regional blockade to facilitate inpatient rehabilitation of recalcitrant complex regional pain syndrome. PM&R 2009, 1, 194–198. [Google Scholar] [CrossRef]
- Collins, C.K. Physical therapy management of complex regional pain syndrome I in a 14-year-old patient using strain counterstrain: A case report. J. Man. Manip. Ther. 2007, 15, 25–41. [Google Scholar] [CrossRef] [Green Version]
- Feldman, A.B.; Saint-Phard, D. Femoral neck stress fracture complicated by deep venous thrombosis and complex regional pain syndrome: A case report. PM&R 2009, 1, 584–586. [Google Scholar] [CrossRef]
- Hind, K.; Johnson, M.I. Complex regional pain syndrome in a competitive athlete and regional osteoporosis assessed by dual-energy X-ray absorptiometry: A case report. J. Med. Case Rep. 2014, 8, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khadavi, M.J.; Alm, J.C.; Emerson, J.A. Complex regional pain syndrome in a young athlete with von Willebrand disease. Pain Med. 2014, 15, 1011–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladd, A.L.; DeHaven, K.E.; Thanik, J.; Patt, R.B.; Feuerstein, M. Reflex sympathetic imbalance. Response to epidural blockade. Am. J. Sports Med. 1989, 17, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Silvestrini, J.A.; Micheo, W.F. Complex regional pain syndrome in pediatric sports: A case series of three young athletes. Bol. Asoc. Med. Puerto Rico 2006, 98, 31–37. [Google Scholar]
- McAlear, G.E.; Popp, J.K. Complex Regional Pain Syndrome Type I in a Female Division I Soccer Player: A Level 4 CASE Report. Int. J. Athl. Ther. Train. 2021, 26, 191–195. [Google Scholar] [CrossRef]
- Middlemas, D.A. Complex Regional Pain Syndrome Type I in a 10-Year-Old Soccer Player. Athl. Ther. Today 2007, 12, 36–40. [Google Scholar]
- Myers, R.A. Exaggerated pain after injury in the athlete: Complex regional pain considerations. Curr. Sports Med. Rep. 2013, 12, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Rand, S.E. Complex regional pain syndrome in the adolescent athlete. Curr. Sports Med. Rep. 2009, 8, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.; Wheeler, M.; Patel, A. Case series: IV regional anesthesia with ketorolac and lidocaine: Is it effective for the management of complex regional pain syndrome 1 in children and adolescents? Anesth. Analg. 2003, 96, 694–695. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Tominaga, T.; Okawa, K.; Tanaka, K. Recovery from acute pediatric complex regional pain syndrome type I after ankle sprain by early pharmacological and physical therapies in primary care: A case report. J. Pain Res. 2018, 11, 2859–2866. [Google Scholar] [CrossRef] [Green Version]
- Walia, K.S.; Muser, D.E.; Raza, S.S.; Griech, T.; Khan, Y.N. A management of early CRPS I caused by ankle sprain: A case report. Pain Pract. 2004, 4, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; Amato, H. Complex Regional Pain Syndrome in a College Athlete. Athl. Ther. Today 2002, 7, 18–24. [Google Scholar] [CrossRef]
- de Mos, M.; de Bruijn, A.G.; Huygen, F.J.; Dieleman, J.P.; Stricker, B.H.; Sturkenboom, M.C. The incidence of complex regional pain syndrome: A population-based study. Pain 2007, 129, 12–20. [Google Scholar] [CrossRef]
- Abu-Arafeh, H.; Abu-Arafeh, I. Complex regional pain syndrome in children: Incidence and clinical characteristics. Arch. Dis. Child. 2016, 101, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Conn, J.M.; Annest, J.L.; Bossarte, R.M.; Gilchrist, J. Non-fatal sports and recreational violent injuries among children and teenagers, United States, 2001–2003. J. Sci. Med. Sport 2006, 9, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Darrow, C.J.; Collins, C.L.; Yard, E.E.; Comstock, R.D. Epidemiology of severe injuries among United States high school athletes: 2005–2007. Am. J. Sports Med. 2009, 37, 1798–1805. [Google Scholar] [CrossRef]
- Peterlin, B.L.; Rosso, A.L.; Nair, S.; Young, W.B.; Schwartzman, R.J. Migraine may be a risk factor for the development of complex regional pain syndrome. Cephalalgia 2010, 30, 214–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duong, H.P.; Konzelmann, M.; Vuistiner, P.; Burrus, C.; Léger, B.; Stiefel, F.; Luthi, F. Psychiatric Comorbidity and Complex Regional Pain Syndrome through the Lens of the Biopsychosocial Model: A Comparative Study. J. Pain Res. 2020, 13, 3235–3245. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Stubhaug, A. Importance of early diagnosis of complex regional pain syndrome (CRPS-1 and C RPS-2): Delayed diagnosis of CRPS is a major problem. Scand. J. Pain 2016, 11, 49–51. [Google Scholar] [CrossRef]
- Grieve, S.; Jones, L.; Walsh, N.; McCabe, C. What outcome measures are commonly used for Complex Regional Pain Syndrome clinical trials? A systematic review of the literature. Eur. J. Pain 2016, 20, 331–340. [Google Scholar] [CrossRef]
- Packham, T.; Holly, J. Mechanism-specific rehabilitation management of complex regional pain syndrome: Proposed recommendations from evidence synthesis. J. Hand Ther. 2018, 31, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Resmini, G.; Ratti, C.; Canton, G.; Murena, L.; Moretti, A.; Iolascon, G. Treatment of complex regional pain syndrome. Clin. Cases Miner. Bone Metab. 2015, 12 (Suppl. S1), 26–30. [Google Scholar] [CrossRef]
- Iolascon, G.; Moretti, A. Pharmacotherapeutic options for complex regional pain syndrome. Expert Opin. Pharmacother. 2019, 20, 1377–1386. [Google Scholar] [CrossRef]


{kind=link}
| Author and Year | Number of Patients | Gender | Age | Sport Practiced | BC | Imaging | Cold/Warm Type | Site |
|---|---|---|---|---|---|---|---|---|
| Carayannopoulos et al., 2009 [12] | 1 | F | 12 | Soccer, basketball, field hockey | No | US | n.a. | Ankle |
| Collins, 2007 [13] | 1 | M | 13 | Baseball, soccer, handball, basketball | No | XR, MRI, BS | n.a. | Ankle |
| Feldman et al., 2009 [14] | 1 | F | 37 | Triathlon | Yes | MRI | n.a. | Lower extremity |
| Hind et al., 2014 [15] | 1 | M | 29 | Powerlifting | Yes | DXA | n.a. | Leg |
| Khadavi et al., 2014 [16] | 1 | F | 17 | Athletics | No | MRI | Cold | Calf |
| Ladd et al., 1989 [17] | 3 | 1 M, 2 F | 18, 20, 31 | Athletics, swimming, hockey | No | No | n.a. | Ankle and knee |
| Martìnez-Silvestrini et al., 2006 [18] | 3 | F | 11, 13, 14 | Athletics, Volleyball | No | XR | n.a. | Foot, ankle, knee |
| McAlear et al., 2021 [19] | 1 | F | 18 | Soccer | No | No | n.a. | Foot |
| Middlemas, 2007 [20] | 1 | F | 10 | Soccer | No | XR, US | Warm | Foot |
| Myers, 2013 [21] | 1 | F | 46 | Running | No | XR | Warm | Knee |
| Rand, 2009 [22] | 1 | F | 10 | Gymnastics | No | MRI | n.a. | Knee |
| Suresh et al., 2002 [23] | 2 | F | 11–15 | Gymnastics, volleyball | No | No | n.a. | Foot and wrist |
| Takahashi et al., 2018 [24] | 1 | M | 12 | Soccer | No | XR, CT | n.a. | Ankle |
| Walia et al., 2004 [25] | 1 | M | 13 | Wrestling | No | XR, MRI, BS | n.a. | Ankle |
| Weber et al., 2002 [26] | 1 | F | 18 | Field hockey | No | XR, BS | Warm | Ankle |
| Authors and Year | Time from Inciting Event | Time to Diagnosis | Comorbidity | Treatment | Main Findings |
|---|---|---|---|---|---|
| Carayannopoulos et al., 2009 [12] | Unknown time after ankle sprains | 2 years | Not reported | P, PT, OT, CBT, RNB | Pain relief, increased ankle RoM and functional independence |
| Collins, 2007 [13] | 15 months from ankle sprain | 2 months | Not reported | P, PT | Pain relief, improvement of gait cadence and pattern, endurance, weight bearing tolerance, ankle RoM and strength (+) |
| Feldman et al., 2009 [14] | 6 weeks after femoral fracture | 6 weeks | Osteopenia, amenorrhea, depression | P, PT, LSPB | Reduced discomfort, normalization of local color and temperature |
| Hind et al., 2014 [15] | Years after orthopedic surgery | 4 years | Calve–Perthes disease | LSPB, P, SCS | Not reported |
| Khadavi et al., 2014 [16] | Months after gastrocnemius strain | 6 months | Type 1 von Willebrand disease | P, PT | Improvement of passive RoM (knee extension and ankle dorsiflexion) and gait distance, reduced device usage and increased weight-bearing tolerance |
| Ladd et al., 1989 [17] | 3 months after ACL reconstruction; weeks after overuse; 10 days after ankle sprain | 10 days–3 months | Sprain and osteoarthritis | LSPB, P, PT | Return to activity (3–27 months) |
| Martìnez-Silvestrini et al., 2006 [18] | 1 day after ankle sprain; 3 days after overuse; 2.5 months after ankle sprain | 2 days–2.5 months | Depression | P, PT | Reduced edema and pain, improvement of RoM |
| McAlear et al., 2021 [19] | 2 weeks after tarsal tunnel release surgery | 2 weeks | Depression | LSPB | Return to activity |
| Middlemas, 2007 [20] | No leading cause | 2–3 weeks | Not available | P, PT | Improvement of weight bearing tolerance and independence in ADL, return to activity |
| Myers, 2013 [21] | No leading cause | 10 days | Not available | P, PT | Pain relief and increased RoM |
| Rand, 2009 [22] | 7 weeks after knee injury | 6 weeks | Migraine | PT, LSPB, P, CBT | Return to activity (8 weeks) |
| Suresh et al., 2002 [23] | 1 year after metatarsal avulsion; 2 months after wrist injury | 2 months–1 year | Not available | P, PT, RNB | Return to activity (3 months), pain relief |
| Takahashi et al., 2018 [24] | 5 days after ankle sprain | 10 days | Not available | P, PT | Return to activity (35 days), pain relief |
| Walia et al., 2004 [25] | Unknown time after ankle sprain | Not known | Not available | P, PT, LSPB | Pain relief and gait improvement |
| Weber et al., 2002 [26] | 16 days after ankle sprain | 1 month | Not available | PT, LSPB | Improvement of symptoms, return to activity (2 months) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moretti, A.; Palomba, A.; Paoletta, M.; Liguori, S.; Toro, G.; Iolascon, G. Complex Regional Pain Syndrome in Athletes: Scoping Review. Medicina 2021, 57, 1262. https://doi.org/10.3390/medicina57111262
Moretti A, Palomba A, Paoletta M, Liguori S, Toro G, Iolascon G. Complex Regional Pain Syndrome in Athletes: Scoping Review. Medicina. 2021; 57(11):1262. https://doi.org/10.3390/medicina57111262
Chicago/Turabian StyleMoretti, Antimo, Angela Palomba, Marco Paoletta, Sara Liguori, Giuseppe Toro, and Giovanni Iolascon. 2021. "Complex Regional Pain Syndrome in Athletes: Scoping Review" Medicina 57, no. 11: 1262. https://doi.org/10.3390/medicina57111262