
Physical Agent Modalities in Early Osteoarthritis: A Scoping Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
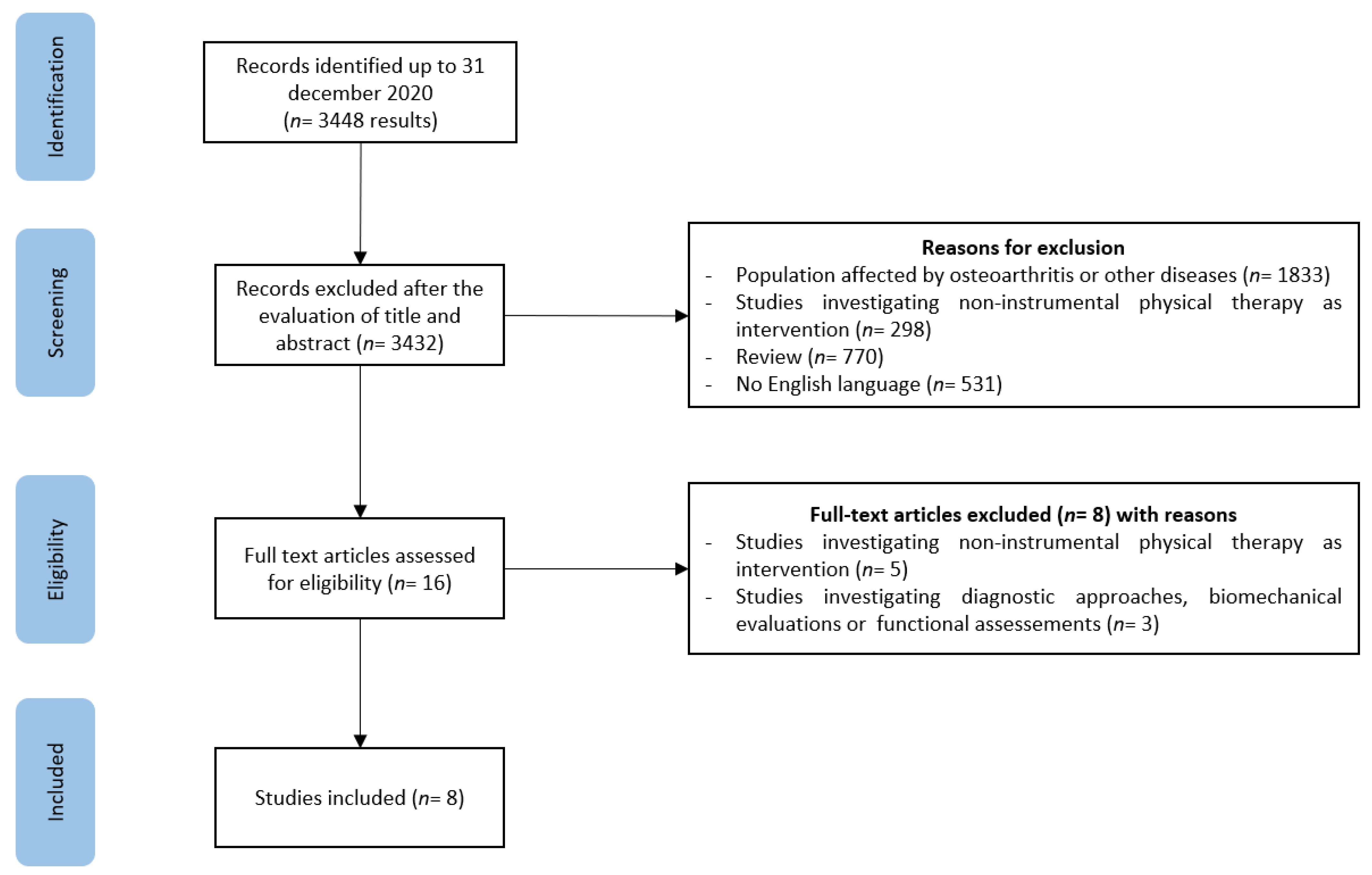
2.1. Search Strategy
2.2. Study Selection
3. Results
3.1. TENS
3.2. ESWT
3.3. LIPUS
3.4. PEMF
3.5. WBV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.P. Osteoarthritis. Nat. Rev. Dis. Primers 2016, 2, 16072. [Google Scholar] [CrossRef] [Green Version]
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, Rev-325. [Google Scholar] [CrossRef]
- Iolascon, G.; Gimigliano, F.; Moretti, A.; De Sire, A.; Migliore, A.; Brandi, M.L.; Piscitelli, P. Early osteoarthritis: How to define, diagnose, and manage. A systematic review. Eur. Geriatr. Med. 2017, 8, 383–396. [Google Scholar] [CrossRef]
- Luyten, F.P.; Denti, M.; Filardo, G.; Kon, E.; Engebretsen, L. Definition and classification of early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migliore, A.; Scirè, C.A.; Carmona, L.; Herrero-Beaumont, G.; Bizzi, E.; Branco, J.; Carrara, G.; Chevalier, X.; Collaku, L.; Aslanidis, S.; et al. The challenge of the definition of early symptomatic knee osteoarthritis: A proposal of criteria and red flags from an international initiative promoted by the Italian Society for Rheumatology. Rheumatol. Int. 2017, 37, 1227–1236, Erratum in 2017, 37, 1237–1238. [Google Scholar] [CrossRef]
- Mahmoudian, A.; Lohmander, L.S.; Jafari, H.; Luyten, F.P. Towards classification criteria for early-stage knee osteoarthritis: A population-based study to enrich for progressors. Semin. Arthritis Rheum. 2021, 51, 285–291. [Google Scholar] [CrossRef]
- Kucharz, E.J.; Szántó, S.; Ivanova Goycheva, M.; Petronijević, M.; Šimnovec, K.; Domżalski, M.; Gallelli, L.; Kamenov, Z.; Konstantynowicz, J.; Radunović, G.; et al. Endorsement by Central European experts of the revised ESCEO algorithm for the management of knee osteoarthritis. Rheumatol. Int. 2019, 39, 1117–1123, Erratum in 2019, 39, 1661–1662. [Google Scholar] [CrossRef] [Green Version]
- Migliore, A.; Paoletta, M.; Moretti, A.; Liguori, S.; Iolascon, G. The perspectives of intra-articular therapy in the management of osteoarthritis. Expert Opin. Drug Deliv. 2020, 17, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Cherian, J.J.; Kapadia, B.H.; Bhave, A.; McElroy, M.J.; Cherian, C.; Harwin, S.F.; Mont, M.A. Use of Transcutaneous Electrical Nerve Stimulation Device in Early Osteoarthritis of the Knee. J. Knee Surg. 2015, 28, 321–327. [Google Scholar] [CrossRef]
- Chou, W.Y.; Cheng, J.H.; Wang, C.J.; Hsu, S.L.; Chen, J.H.; Huang, C.Y. Shockwave Targeting on Subchondral Bone Is More Suitable than Articular Cartilage for Knee Osteoarthritis. Int. J. Med. Sci. 2019, 16, 156–166. [Google Scholar] [CrossRef] [Green Version]
- Hsu, S.L.; Cheng, J.H.; Wang, C.J.; Ko, J.Y.; Hsu, C.H. Extracorporeal Shockwave Therapy Enhances Expression of Pdia-3 Which Is a Key Factor of the 1α,25-Dihydroxyvitamin D 3 Rapid Membrane Signaling Pathway in Treatment of Early Osteoarthritis of the Knee. Int. J. Med. Sci. 2017, 14, 1220–1230. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.H.; Wang, C.J.; Su, S.H.; Huang, C.Y.; Hsu, S.L. Next-generation sequencing identifies articular cartilage and subchondral bone miRNAs after ESWT on early osteoarthritis knee. Oncotarget 2016, 7, 84398–84407. [Google Scholar] [CrossRef] [Green Version]
- Xia, P.; Shen, S.; Lin, Q.; Cheng, K.; Ren, S.; Gao, M.; Li, X. Low-Intensity Pulsed Ultrasound Treatment at an Early Osteoarthritis Stage Protects Rabbit Cartilage From Damage via the Integrin/Focal Adhesion Kinase/Mitogen-Activated Protein Kinase Signaling Pathway. J. Ultrasound. Med. 2015, 34, 1991–1999. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; He, H.; Zhou, Y.; Zhou, Y.; Gao, Q.; Wang, P.; He, C. Pulsed electromagnetic field at different stages of knee osteoarthritis in rats induced by low-dose monosodium iodoacetate: Effect on subchondral trabecular bone microarchitecture and cartilage degradation. Bioelectromagnetics 2017, 38, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Lad, D.; Petrera, M.; Karnatzikos, G. Symptomatic Early Osteoarthritis of the Knee Treated With Pulsed Electromagnetic Fields: Two-Year Follow-up. Cartilage 2014, 5, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, Z.; Liu, Q.; Su, J.; Wang, T.; Li, T. Effect of whole body vibration on HIF-2α expression in SD rats with early knee osteoarthritis. J. Bone Miner. Metab. 2020, 38, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Kon, E.; Longo, U.G.; Madry, H.; Marchettini, P.; Marmotti, A.; Van Assche, D.; Zanon, G.; Peretti, G.M. Non-surgical treatments for the management of early osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Xie, Y.; Luo, X.; Ji, Q.; Lu, C.; He, C.; Wang, P. Effects of therapeutic ultrasound on pain, physical functions and safety outcomes in patients with knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2016, 30, 960–971. [Google Scholar] [CrossRef]
- Zeng, C.; Li, H.; Yang, T.; Deng, Z.H.; Yang, Y.; Zhang, Y.; Lei, G.H. Electrical stimulation for pain relief in knee osteoarthritis: Systematic review and network meta-analysis. Osteoarthr. Cartil. 2015, 23, 189–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKnight, P.E.; Kasle, S.; Going, S.; Villanueva, I.; Cornett, M.; Farr, J.; Wright, J.; Streeter, C.; Zautra, A. A comparison of strength training, self-management, and the combination for early osteoarthritis of the knee. Arthritis Care Res. 2010, 62, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vad, V.; Hong, H.M.; Zazzali, M.; Agi, N.; Basrai, D. Exercise recommendations in athletes with early osteoarthritis of the knee. Sports Med. 2002, 32, 729–739. [Google Scholar] [CrossRef]
- Chen, L.; Ye, L.; Liu, H.; Yang, P.; Yang, B. Extracorporeal Shock Wave Therapy for the Treatment of Osteoarthritis: A Systematic Review and Meta-Analysis. Biomed. Res. Int. 2020, 2020, 1907821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, J.; Min, Z.; Xia, Z.; Cheng, B.; Lan, B.; Zhang, F.; Han, Y.; Wang, K.; Sun, J. The hsa-miR-181a-5p reduces oxidation resistance by controlling SECISBP2 in osteoarthritis. BMC Musculoskelet. Disord. 2018, 19, 355. [Google Scholar] [CrossRef]


{kind=link}
| (“Electric Stimulation Therapy” [Mesh] OR “Pulsed Electromagnetic field” OR “Low-Level Light Therapy” [Mesh] OR “Laser Therapy” [Mesh] OR “Magnetic Field Therapy” [Mesh] OR “Extracorporeal Shockwave Therapy” [Mesh] OR “Hyperthermia, Induced” [Mesh] OR “Cryotherapy” [Mesh] OR “Vibration therapy” OR “Whole Body Vibration” OR “Physical Therapy Modalities” [Mesh]) AND (“Osteoarthritis” [Mesh] OR “Osteoarthritis, Spine” [Mesh] OR “Osteoarthritis, Knee” [Mesh] OR “Osteoarthritis, Hip” [Mesh] OR “Early Osteoarthritis”) |
| Inclusion Criteria |
|---|
|
| Exclusion Criteria |
|
| Author, Year | Physical Therapy Modality | Study Design | Sample Size: Total (Group) | Administration | Main Findings |
|---|---|---|---|---|---|
| Cherian et al., 2015 [12] | TENS | Prospective, randomized, single-blinded trial, including EKOA patients (Kellgren–Lawrence grade 1) | n = 23 TENS group = 13 Control group = 10 | TENS: device included in a brace to wear for the entire day Pulse waveform: asymmetric, biphasic, and simple modulated Pulse rate: 12 s intervals of grouped pulses Voltage current: 48–400 μs at 50% peak amplitude Duration of the intervention: 3 months Control: self-directed exercise therapy and/or corticosteroid injections | TENS significantly improved quadriceps strength, TUGT, objective KSS score, LEFS, and physical component of SF-36 compared to controls. |
| Chou et al., 2019 [13] | ESWT | Preclinical study on EKOA rat model (ACLT + MM) | n = 50 5 groups (10 rats in each group) | Group I Sham: arthrotomy of left knee Group II Meniscus: arthrotomy and ESWT applied to the medial edge of the meniscus Group III OA: anterior cruciate ligament transacted (ACLT) and medial meniscectomy (MMx) Group IV T(M): ACLT and MMx of left knee and ESWT applied to the proximal medial tibia plateaus Group V Articular Cartilage: The animals received ACLT and MMx of left knee and ESWT applied to the articular cartilage surface of the proximal medial tibia plateaus One ESWT at 1-week post-surgery with ultrasound guidance ESWT: 800 impulses at 0.25 mJ/mm | ESWT applied to the subchondral bone has protective effects for articular cartilage, synovium, and subchondral bone. |
| Hsu et al., 2017 [14] | ESWT | Preclinical study on EKOA rat model (ACLT) | n = 144 | Group I: normal control (NC) Group II: EKOA induced by ACLT Group III: EKOA induced by ACLT receiving ESWT (800 impulses at 0.18 mJ/mm2, 4 Hz frequency) to the subchondral bone of the medial tibia plate. 12 rats in each group were sacrificed at 2, 4, 8, and 12 weeks post-surgery. Of the 12 rats at 2 weeks post-surgery, the articular cartilage and subchondral bone of tibia of 6 rats were used for proteome analysis and the joints of another 6 rats for immunohistochemistry analysis. | ESWT might affect chondrocytes’ and osteoblasts’ functions in the joint environment by modulating several factors of the rapid membrane signaling pathway, including Pdia-3, ERK1, OPG, ALP, and MMP13. These factors significantly increased at 2 weeks post-treatment, resulting in favorable histological changes. |
| Cheng et al., 2016 [15] | ESWT | Preclinical study on EKOA rat model (ACLT + MM) | n = 30 | Group I: sham Group II: OA Group III: OA + ESWT applied on the subchondral bone of the medial tibia plateau One ESWT at 1-week post-surgery. ESWT: 800 impulses at 0.22 mJ/mm and 4 Hz frequency Histological and miRNA analyses were performed after 4 weeks. A set of 729 miRNAs expressed in cartilage and subchondral bone was obtained. | ESWT induced expression of miRNA to control genes correlated with cartilage development and bone remodeling. In the ESWT group, the articular surface damage was not obvious and only mild fibrillation was observed. |
| Xia et al., 2015 [16] | LIPUS | Preclinical study on rabbit EKOA model (ACLT) | n = 36 | Group I: early control (6) Group II: early osteoarthritis (6) Group III: early treatment (6) Group IV: late control (6) Group V: late osteoarthritis (6) Group VI: late treatment (6) The early and late treatment groups were exposed to low-intensity pulsed US 4 and 8 weeks after surgery | LIPUS protects cartilage from damage in early-stage osteoarthritis via the integrin/FAK/MAPK pathway |
| Yang et al., 2017 [17] | PEMF | Preclinical study on EKOA rat model (induced by low-dose of MIA) | n = 75 | Group I: OA (30) Group II: pre-emptive PEMF (10) from day 0 to end of week 4 Group III: early PEMF (10) from week 4 to end of week 8 Group IV: delayed PEMF (10) end of week 8 to end of week 12 Group V: control (15) After 1 week, rats in OA and PEMF groups were injected with 0.2 mg MIA through the infrapatellar ligament of the right knee only once. MIA was dissolved in sterile physiologic saline and administered in a 50 mL microsyringe. Control rats received a 50 mL sterile physiologic saline injection. PEMF: Frequency of 75 Hz Intensity of 1.6 mT Duration: 2 h/day for 1 months during the activities of daily life | Pre-emptive and early PEMF treatment significantly increased bone and cartilage synthesis and decreased bone and cartilage degradation Pre-emptive PEMF treatment has a more beneficial effect on subchondral trabecular bone microarchitecture. Delayed PEMF treatment only increased bone synthesis The time point of treatment initiation is crucial for treating OA |
| Gobbi et al., 2014 [18] | PEMF | Prospective study (EKOA patients Kellgren–Lawrence grade 0–2) | n = 22 | PEMF (4 h per day) for 45 days The maximum intensity of the magnetic field was 1.5 mT and the frequency was 75 Hz. 1- and 2-year follow-up. | PEMF reduced symptoms (pain and joint swelling) and improved knee function and activity level in EKOA patients at the 1-year follow-up, especially in young patients. These effects decreased at 2-year follow-up |
| Wang et al., 2020 [19] | WBV | Preclinical study on EKOA rat model (induced by 0.15 mL mixture of 4% papain and 0.03 mmol/L l-cysteine into knee joint cavity) | n = 40 | Group I: sham control (SC) Group II: high frequency 60 Hz (HV1) Group III: high frequency 40 Hz (HV2) Group IV: middle frequency 20 Hz (MV) Group V: low frequency 10 Hz (LV) WBV (peak acceleration 0.3 g): 40 min/day and 5 days/week | WBV could alleviate the degeneration of articular cartilage. WBV regulates related gene expression at both mRNA and protein levels. HIF-2α could be a therapeutic target. The effect of WBV seems frequency-dependent: lower frequency shows better effects |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Letizia Mauro, G.; Scaturro, D.; Gimigliano, F.; Paoletta, M.; Liguori, S.; Toro, G.; Iolascon, G.; Moretti, A. Physical Agent Modalities in Early Osteoarthritis: A Scoping Review. Medicina 2021, 57, 1165. https://doi.org/10.3390/medicina57111165
Letizia Mauro G, Scaturro D, Gimigliano F, Paoletta M, Liguori S, Toro G, Iolascon G, Moretti A. Physical Agent Modalities in Early Osteoarthritis: A Scoping Review. Medicina. 2021; 57(11):1165. https://doi.org/10.3390/medicina57111165
Chicago/Turabian StyleLetizia Mauro, Giulia, Dalila Scaturro, Francesca Gimigliano, Marco Paoletta, Sara Liguori, Giuseppe Toro, Giovanni Iolascon, and Antimo Moretti. 2021. "Physical Agent Modalities in Early Osteoarthritis: A Scoping Review" Medicina 57, no. 11: 1165. https://doi.org/10.3390/medicina57111165