
Can Deep Learning-Based Volumetric Analysis Predict Oxygen Demand Increase in Patients with COVID-19 Pneumonia?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
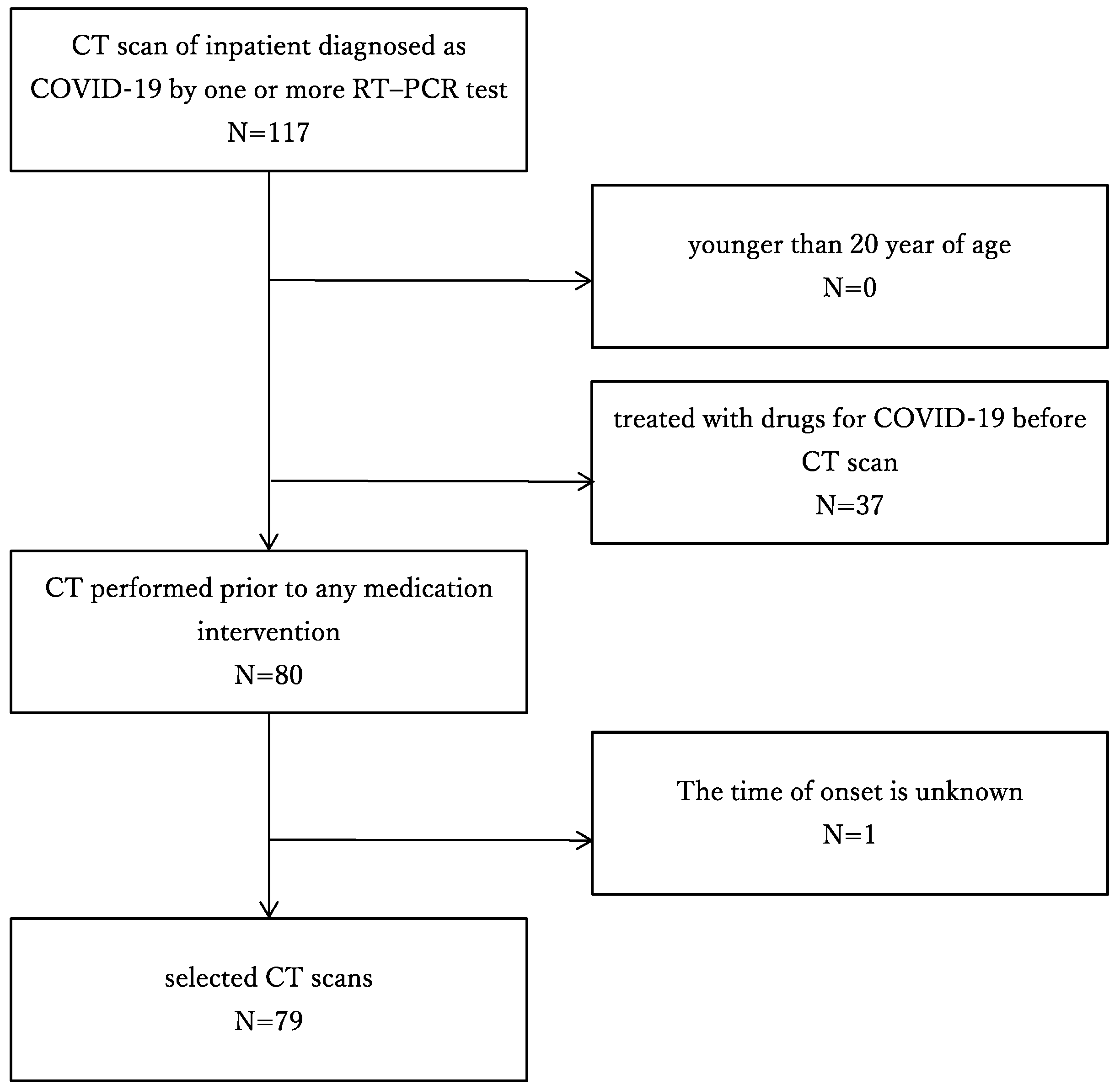
2.1. Study Population
2.2. Chest CT Imaging
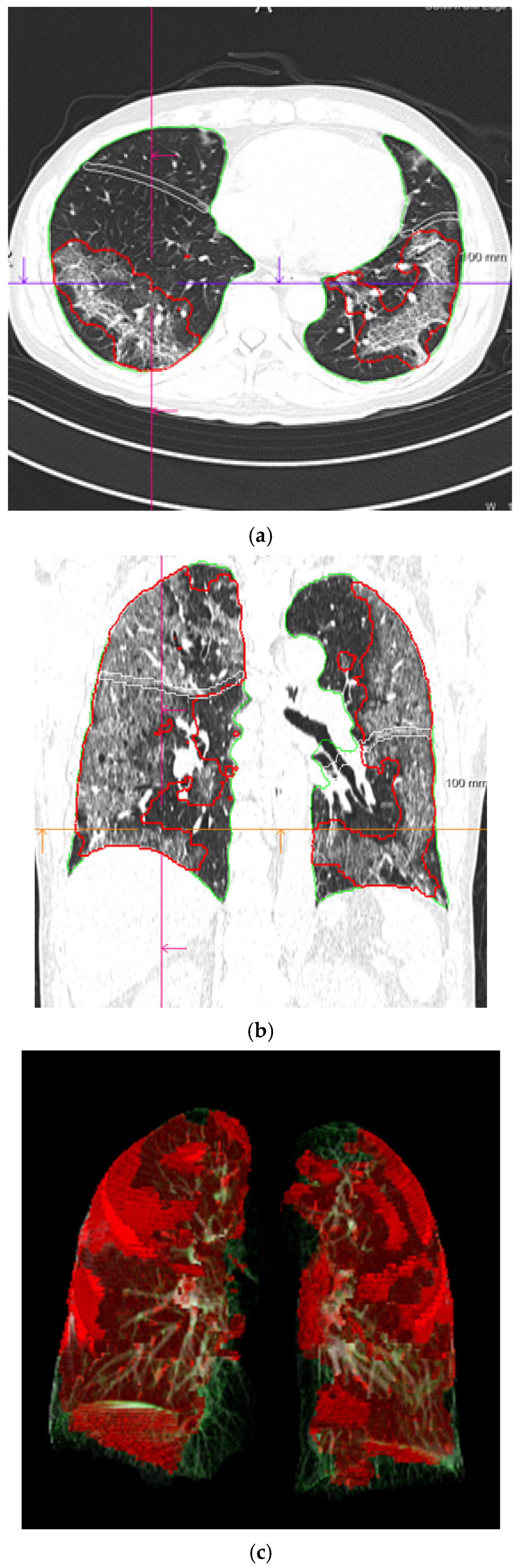
2.3. COVID-19 Pneumonia Analysis Using Deep Learning System
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
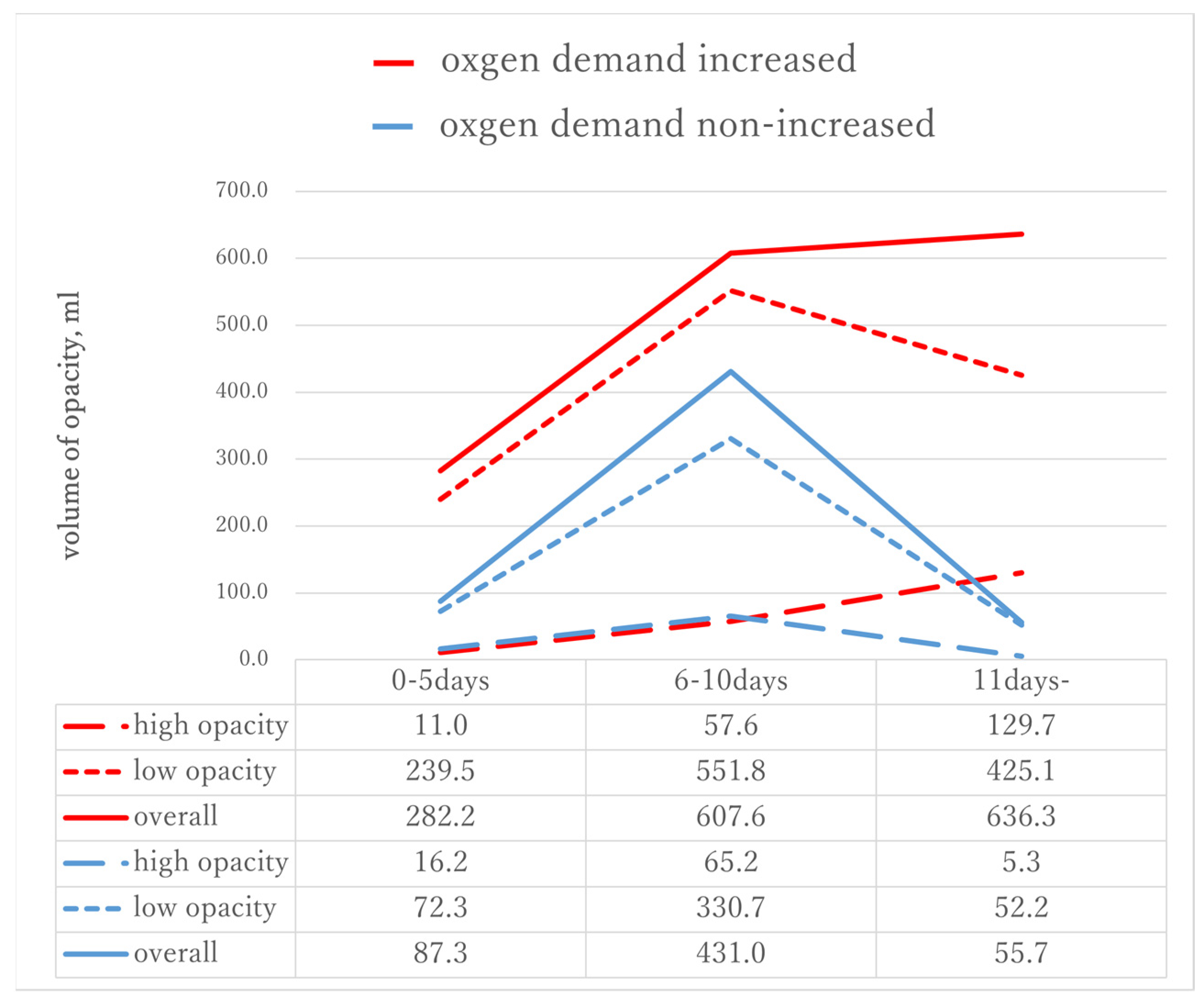
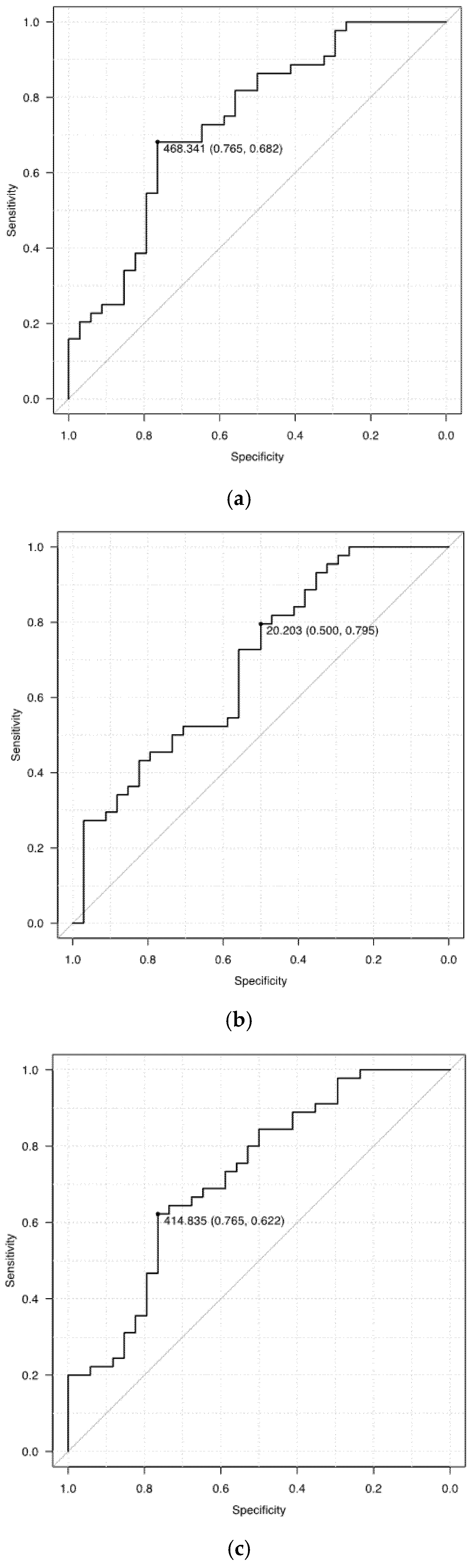
3.2. Volume of Opacities as Predictive Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease 2019 (COVID-19). WHO Health Emergency Dashboard, 2021. Available online: https://covid19.who.int (accessed on 17 September 2021).
- Ministry of Health, Labour and Welfare. Situation Report. Available online: https://www.mhlw.go.jp/stf/covid-19/kokunainohasseijoukyou_00006.html#1-1 (accessed on 17 September 2021).
- Oran, D.P.; Topol, E. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M. Chronic obstructive pulmonary disease is associated with severe coronavirus disease 2019 (COVID-19). Respir. Med. 2020, 167, 105941. [Google Scholar] [CrossRef]
- Jain, V.; Yuan, J.-M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 65, 533–546. [Google Scholar] [CrossRef]
- Parekh, M.; Donuru, A.; Balasubramanya, R.; Kapur, S. Review of the Chest CT Differential Diagnosis of Ground-Glass Opacities in the COVID Era. Radiology 2020, 297, E289–E302. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [Green Version]
- Kanne, J.P.; Little, B.P.; Chung, J.H.; Elicker, B.M.; Ketai, L.H. Essentials for Radiologists on COVID-19: An Update—Radiology Scientific Expert Panel. Radiology 2020, 296, E113–E114. [Google Scholar] [CrossRef] [Green Version]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.J.; Qiu, J.; Wu, B.; Huang, T.; Gao, Y.; Wang, Z.P.; Chen, Y.; Chen, F. Early chest CT features of patients with 2019 novel coronavirus (COVID-19) pneumonia: Relationship to diagnosis and prognosis. Eur. Radiol. 2020, 30, 6178–6185. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Fujioka, T.; Katsuta, L.; Kikuchi, Y.; Oda, G.; Nakagawa, T.; Kitazume, Y.; Kubota, K.; Tateishi, U. Feasibility of new fat suppression for breast MRI using pix2pix. Jpn. J. Radiol. 2020, 38, 1075–1081. [Google Scholar] [CrossRef]
- Fujioka, T.; Kubota, K.; Mori, M.; Kikuchi, Y.; Katsuta, L.; Kasahara, M.; Oda, G.; Ishiba, T.; Nakagawa, T.; Tateishi, U. Distinction between benign and malignant breast masses at breast ultrasound using deep learning method with convolutional neural network. Jpn. J. Radiol. 2019, 37, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Adachi, M.; Fujioka, T.; Mori, M.; Kubota, K.; Kikuchi, Y.; Xiaotong, W.; Oyama, J.; Kimura, K.; Oda, G.; Nakagawa, T.; et al. Detection and Diagnosis of Breast Cancer Using Artificial Intelligence Based Assessment of Maximum Intensity Projection Dynamic Contrast-Enhanced Magnetic Resonance Images. Diagnostics 2020, 10, 330. [Google Scholar] [CrossRef] [PubMed]
- Chartrand, G.; Cheng, P.; Vorontsov, E.; Drozdzal, M.; Turcotte, S.; Pal, C.J.; Kadoury, S.; Tang, A. Deep Learning: A Primer for Radiologists. Radiographics 2017, 37, 2113–2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka, T.; Yashima, Y.; Oyama, J.; Mori, M.; Kubota, K.; Katsuta, L.; Kimura, K.; Yamaga, E.; Oda, G.; Nakagawa, T.; et al. Deep-learning approach with convolutional neural network for classification of maximum intensity projections of dynamic contrast-enhanced breast magnetic resonance imaging. Magn. Reson. Imaging 2021, 75, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gouda, W.; Yasin, R. COVID-19 disease: CT Pneumonia Analysis prototype by using artificial intelligence, predicting the disease severity. Egypt. J. Radiol. Nucl. Med. 2020, 51, 1–11. [Google Scholar] [CrossRef]
- Lessmann, N.; Sánchez, C.I.; Beenen, L.; Boulogne, L.H.; Brink, M.; Calli, E.; Charbonnier, J.-P.; Dofferhoff, T.; van Everdingen, W.M.; Gerke, P.K.; et al. Automated Assessment of COVID-19 Reporting and Data System and Chest CT Severity Scores in Patients Suspected of Having COVID-19 Using Artificial Intelligence. Radiology 2021, 298, E18–E28. [Google Scholar] [CrossRef] [PubMed]
- Ni, Q.; Sun, Z.Y.; Qi, L.; Chen, W.; Yang, Y.; Wang, L.; Zhang, X.; Yang, L.; Fang, Y.; Xing, Z.; et al. A deep learning approach to characterize 2019 coronavirus disease (COVID-19) pneumonia in chest CT images. Eur. Radiol. 2020, 30, 6517–6527. [Google Scholar] [CrossRef]
- Ito, R.; Iwano, S.; Naganawa, S. A review on the use of artificial intelligence for medical imaging of the lungs of patients with coronavirus disease 2019. Diagn. Interv. Radiol. 2020, 26, 443–448. [Google Scholar] [CrossRef]
- Gao, K.; Su, J.; Jiang, Z.; Zeng, L.-L.; Feng, Z.; Shen, H.; Rong, P.; Xu, X.; Qin, J.; Yang, Y.; et al. Dual-branch combination network (DCN): Towards accurate diagnosis and lesion segmentation of COVID-19 using CT images. Med. Image Anal. 2021, 67, 101836. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2012, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Rorat, M.; Jurek, T.; Simon, K.; Guziński, M. Value of quantitative analysis in lung computed tomography in patients severely ill with COVID-19. PLoS ONE 2021, 16, e0251946. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhang, Q.; Huang, C.; Shi, C.; Wang, L.; Shi, N.; Fang, C.; Shan, F.; Mei, X.; Shi, J.; et al. CT quantification of pneumonia lesions in early days predicts progression to severe illness in a cohort of COVID-19 patients. Theranostics 2020, 10, 5613–5622. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Liu, T.; Xue, X.; Luo, G.; Wang, X.; Shen, Y.; Fang, Q.; Sheng, J.; Chen, F.; Liang, T. CT Quantification and Machine-learning Models for Assessment of Disease Severity and Prognosis of COVID-19 Patients. Acad. Radiol. 2020, 27, 1665–1678. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All | Increased Oxygen Demand | Nonincreased Oxygen Demand | p-Value | |
|---|---|---|---|---|---|
| Number of subjects, n | 79 | 45 | 34 | - | |
| Baseline characteristics | |||||
| Age, years | 62 [46, 77] | 65 [54, 77] | 51.5 [36, 71.5] | 0.025 | |
| Sex, male, % | 56 (70.9%) | 38 (84.4%) | 18 (52.9%) | 0.005 | |
| Height, cm | 168.5 [163.0, 177.8] | 173.0 [165.0, 179.0] | 164.4 [158.5, 169.3] | 0.008 | |
| Weight, kg | 65.0 [49.0, 74.9] | 67.0 [55.0, 80.0] | 56.5 [48.0, 70.0] | 0.052 | |
| Body mass index | 23.0 [20.8, 25.5] | 24.4 [21.6, 28.1] | 21.4 [19.1, 23.7] | 0.005 | |
| Onset to CT duration, days | 9.0 [6.0, 13.0] | 7.0 [5.0, 9.0] | 10.5 [8.3, 14.0] | 0.005 | |
| Status at the CT scan | |||||
| Oxygen demand, % | none | 56 (70.9%) | 26 (57.8%) | 30 (88.2%) | 0.173 |
| exist | 14 (12.7%) | 10 (22.2%) | 4 (11.8%) | ||
| no data | 9 (11.4%) | 9 (20.0%) | 0 (0.0%) | ||
| Mechanical ventilation, % | 1 (1.3%) | 1 (2.2%) | 0 (0.0%) | 1 | |
| Body temperature, °C | 37.0 [36.7, 37.9] | 37.6 [36.9, 38.0] | 36.7 [36.5, 37.1] | 0.001 | |
| WBC, 103/μL | 5500 [4025, 6900] | 5300 [3670, 6750] | 5600 [4550, 7250] | 0.313 | |
| LYM, % | 19.00 [10.60, 25.30] | 15.65 [9.28, 19.67] | 24.20 [18.15, 28.45] | 0.004 | |
| CRP, mg/dL | 4.96 [1.47, 11.97] | 9.92 [3.76, 15.59] | 2.13 [0.08, 7.88] | <0.001 | |
| LDH, U/L | 292.0 [219.0, 409.0] | 321.0 [284.0, 467.5] | 242.0 [191.5, 314.5] | 0.001 | |
| Lung volume, mL | 4197.2 [3424.6, 4895.8] | 4517.6 [3541.0, 5167.2] | 3828.0 [3352.1, 4575.8] | 0.059 | |
| Volume of opacity, mL | 446.3 [63.8, 767.0] | 585.3 [212.8, 916.1] | 132.8 [10.7, 456.1] | <0.001 | |
| Volume of high opacity, mL | 55.2 [8.2, 102.7] | 71.4 [27.0, 165.4] | 25.1 [0.9, 78.5] | 0.006 | |
| Volume of low opacity, mL | 336.2 [59.0, 655.1] | 440.3 [165.6, 718.0] | 95.1 [10.4, 405.6] | 0.001 | |
| Onset to CT Duration, Days | Type of Opacity | All | Increased Oxygen Demand | Nonincreased Oxygen Demand | p-Value |
|---|---|---|---|---|---|
| 0–5 days | high opacity | 15.3 [6.0, 71.4] | 11.0 [5.7, 87.4] | 16.2 [11.1, 17.9] | 0.752 |
| low opacity | 72.3 [33.8, 500.2] | 239.5 [37.1, 508.9] | 72.33 [33.8, 76.2] | 0.343 | |
| overall | 87.3 [45.2, 526.8] | 282.2 [42.4, 612.4] | 87.3 [50.0, 96.2] | 0.399 | |
| 6–10 days | high opacity | 57.6 [32.7, 126.8] | 57.62 [42.5, 146.9] | 65.2 [13.4, 87.3] | 0.224 |
| low opacity | 480.5 [286.7, 782.44] | 551.8 [361.5, 1106.3] | 330.7 [125.7, 527.7] | 0.044 | |
| overall | 562.5 [329.0, 930.1] | 607.6 [416.3, 1245.5] | 430.98 [134.6, 613.2] | 0.040 | |
| ≥11 days | high opacity | 57.8 [0.9, 127.6] | 129.7 [46.0, 294.5] | 5.28 [0.0, 62.1] | 0.018 |
| low opacity | 165.6 [10.0, 519.7] | 425.1 [152.9, 648.6] | 52.2 [1.5, 388.6] | 0.056 | |
| overall | 325.0 [10.6, 749.7] | 636.3 [252.9, 890.1] | 55.73 [1.6, 446.3] | 0.027 |
| Period | Number | Opacity | High Opacity | Low Opacity |
|---|---|---|---|---|
| Total | 79 | 0.737 (0.624–0.851) | 0.691 (0.572–0.811) | 0.722 (0.607–0.837) |
| 0–5 days | 17 | 0.633 (0.342–0.925) | 0.45 (0.132–0.768) | 0.650 (0.362–0.938) |
| 6–10 days | 35 | 0.714 (0.529–0.898) | 0.373 (0.167–0.579) | 0.710 (0.523–0.898) |
| ≥11 days | 27 | 0.759 (0.574–0.943) | 0.776 (0.593–0.96) | 0.724 (0.528–0.919) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, M.; Fujioka, T.; Horii, T.; Kimura, K.; Kimura, M.; Hashimoto, Y.; Kitazume, Y.; Kishino, M.; Tateishi, U. Can Deep Learning-Based Volumetric Analysis Predict Oxygen Demand Increase in Patients with COVID-19 Pneumonia? Medicina 2021, 57, 1148. https://doi.org/10.3390/medicina57111148
Takahashi M, Fujioka T, Horii T, Kimura K, Kimura M, Hashimoto Y, Kitazume Y, Kishino M, Tateishi U. Can Deep Learning-Based Volumetric Analysis Predict Oxygen Demand Increase in Patients with COVID-19 Pneumonia? Medicina. 2021; 57(11):1148. https://doi.org/10.3390/medicina57111148
Chicago/Turabian StyleTakahashi, Marie, Tomoyuki Fujioka, Toshihiro Horii, Koichiro Kimura, Mizuki Kimura, Yurika Hashimoto, Yoshio Kitazume, Mitsuhiro Kishino, and Ukihide Tateishi. 2021. "Can Deep Learning-Based Volumetric Analysis Predict Oxygen Demand Increase in Patients with COVID-19 Pneumonia?" Medicina 57, no. 11: 1148. https://doi.org/10.3390/medicina57111148