Laparoscopic versus Open Transverse-Incision Approach for Right Hemicolectomy: A Systematic Review and Meta-Analysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy, Eligibility Criteria, and Study Selection
2.2. Statistical Analysis
3. Results
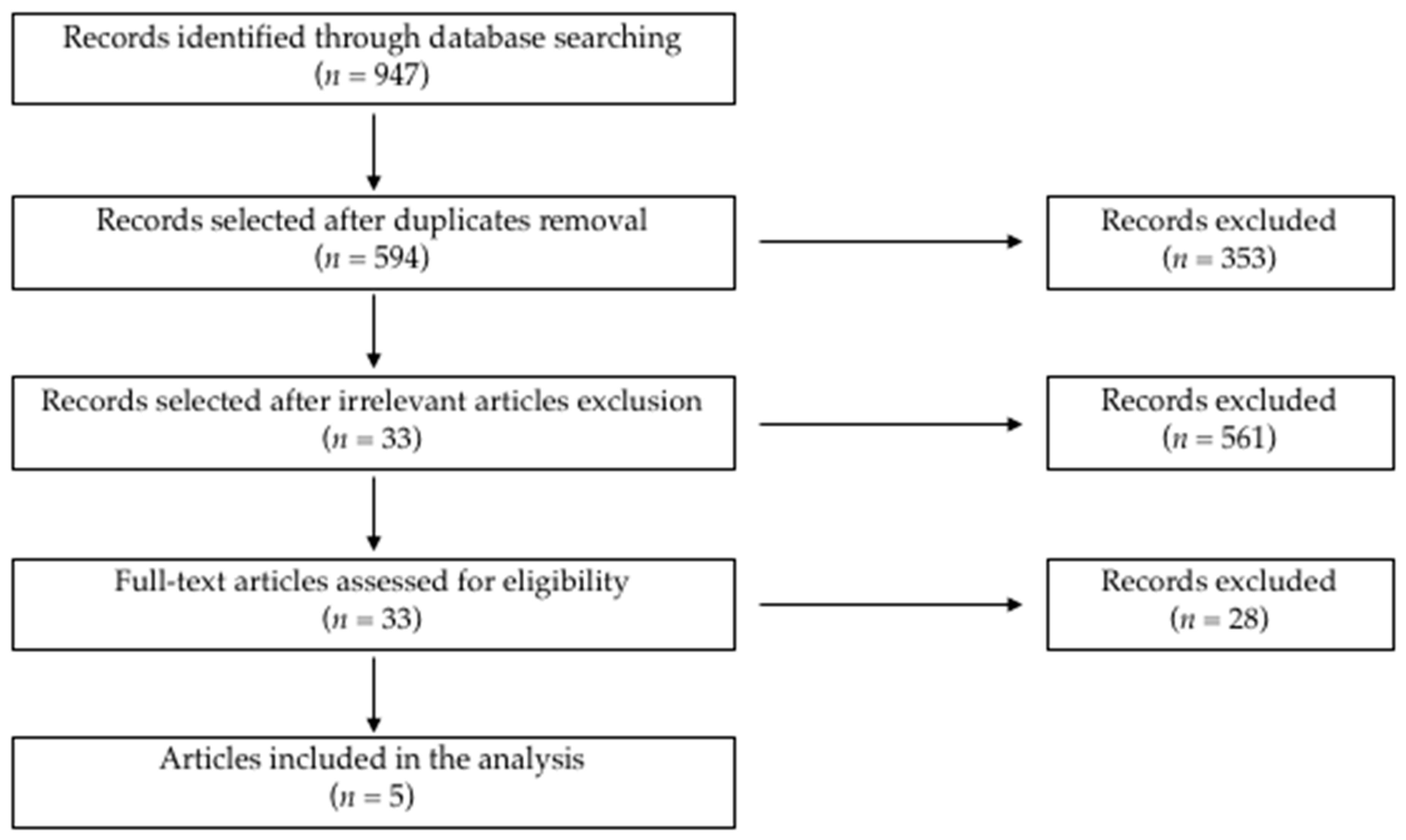
3.1. Literature Search and Study Selection
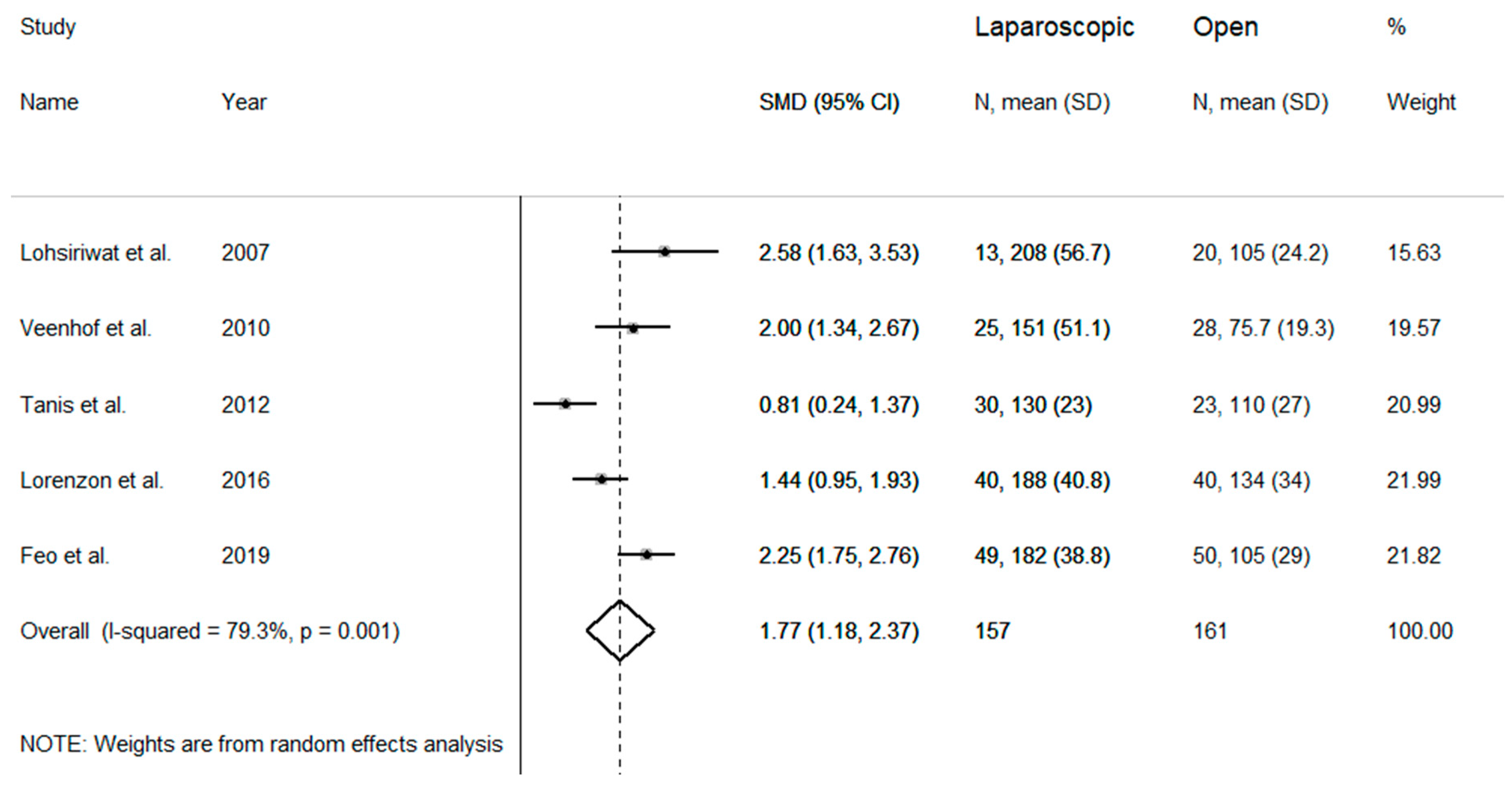
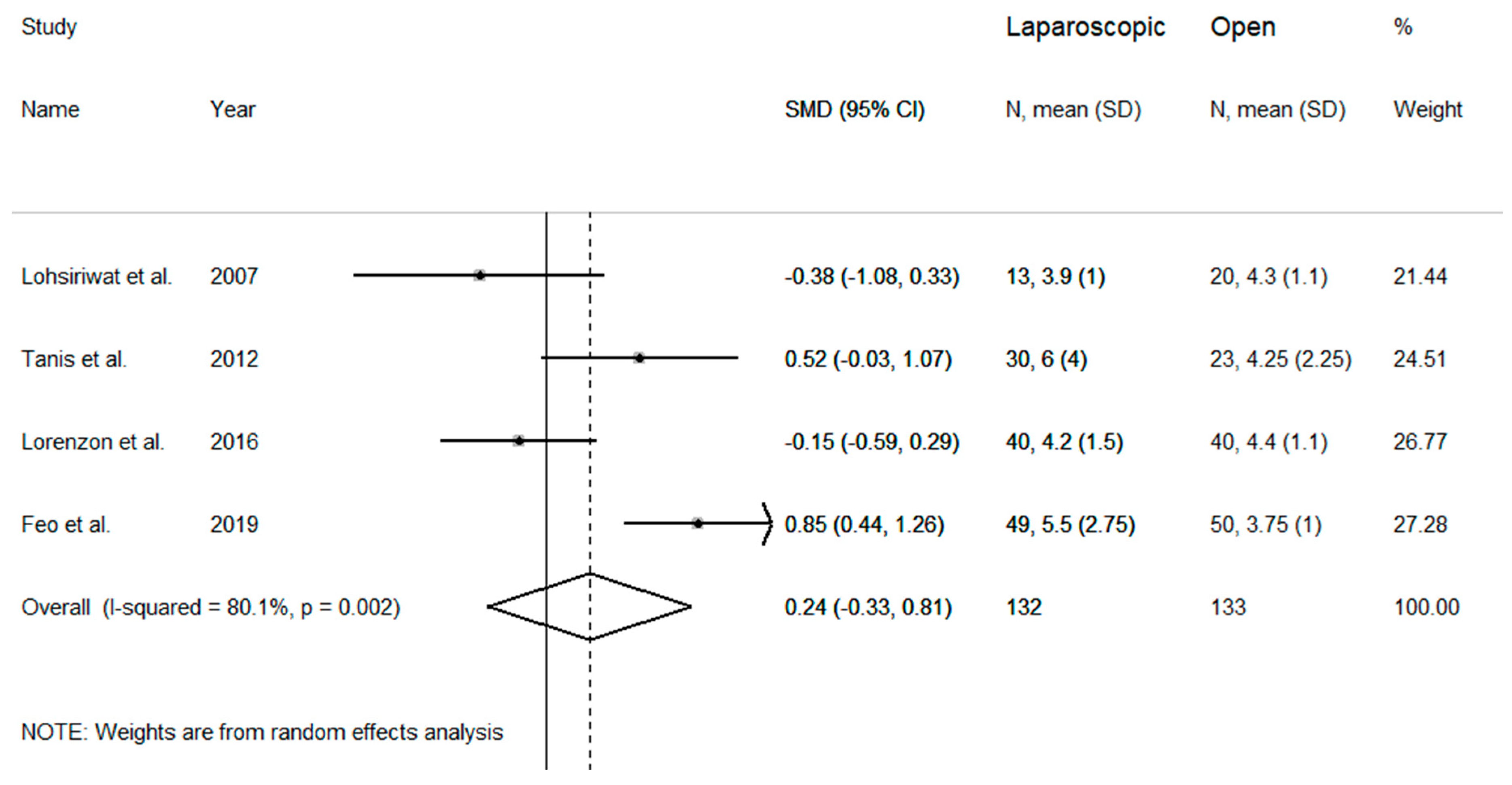
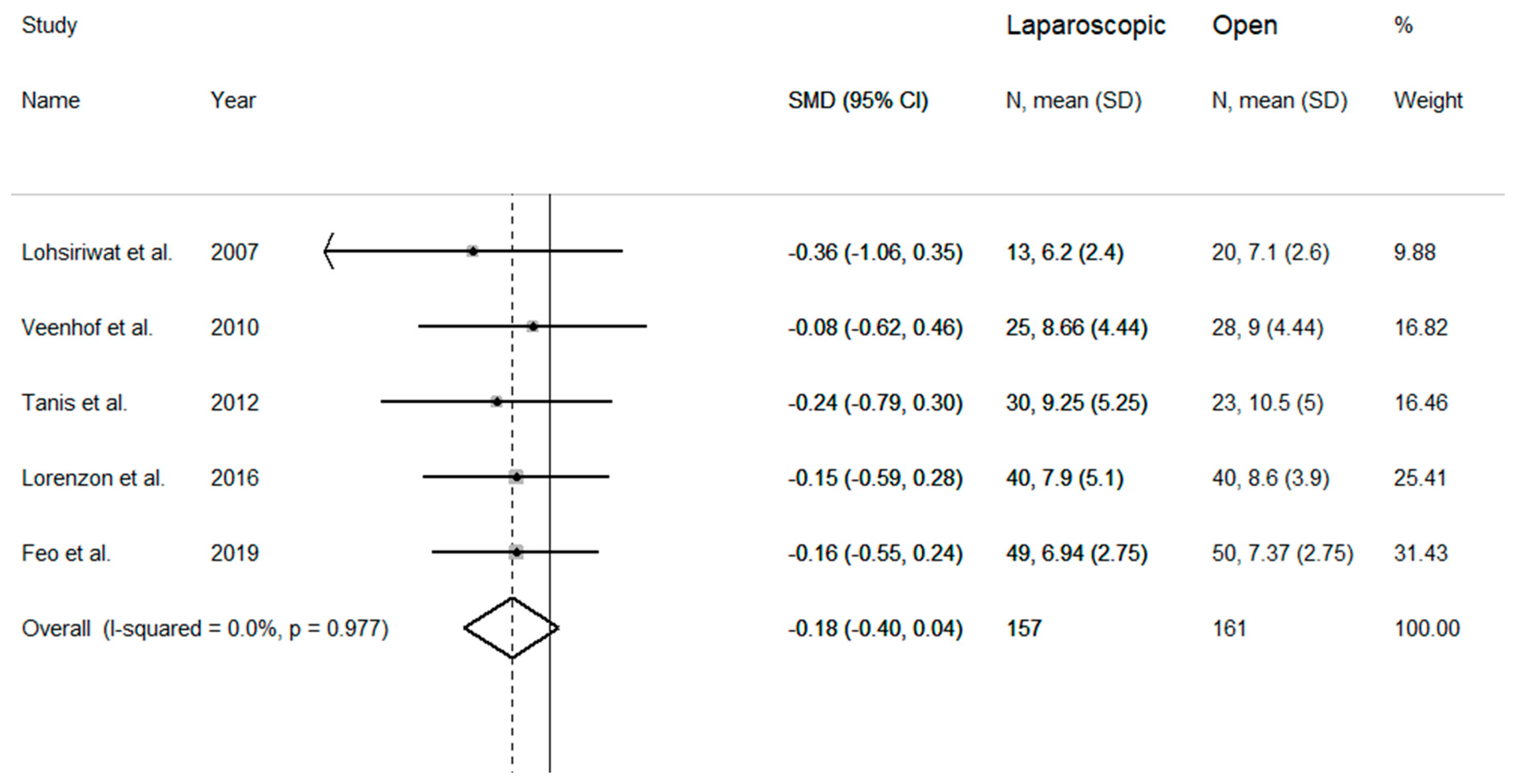
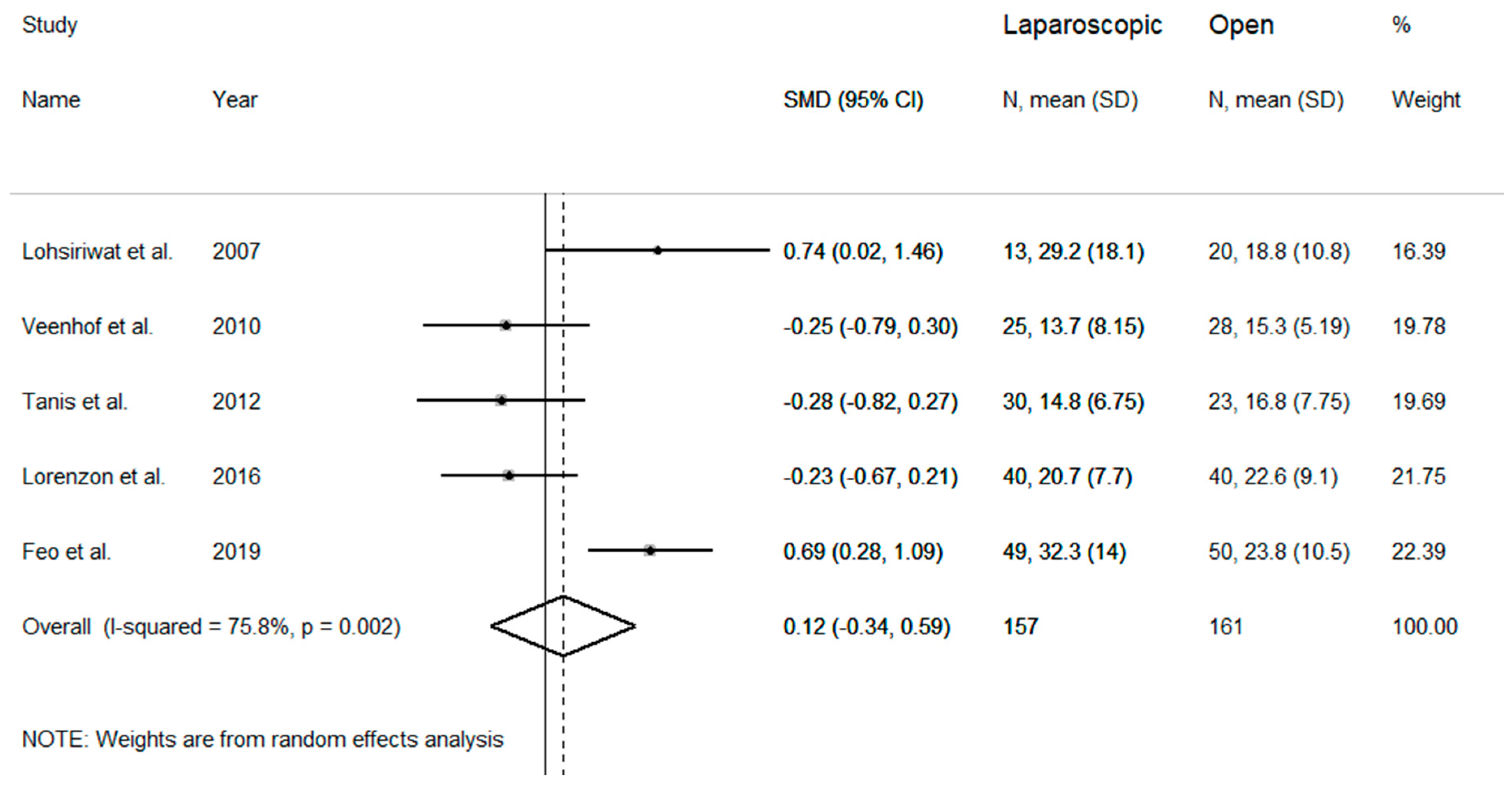
3.2. Meta-Analysis of Studied Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liang, J.T.; Huang, K.C.; Lai, H.S.; Lee, P.H.; Jeng, Y.M. Oncologic results of laparoscopic versus conventional open surgery for stage II or III left-sided colon cancers: A randomized controlled trial. Ann. Surg. Oncol. 2007, 14, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.; Frasson, M.; Zuliani, W.; Vignali, A.; Pecorelli, N.; Di Carlo, V. Randomized clinical trial of laparoscopic versus open left colonic resection. Br. J. Surg. 2010, 97, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Memon, M.A.; Yunus, R.M.; Memon, B.; Awaiz, A.; Khan, S. A Meta-Analysis and Systematic Review of Perioperative Outcomes of Laparoscopic-assisted Rectal Resection (LARR) Versus Open Rectal Resection (ORR) for Carcinoma. Surg. Laparosc. Endosc. Percutan. Tech. 2018, 28, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Jiang, Z.L.; Chen, D.Y.; Chen, M.F.; Chen, L.H.; Zhou, P.; Xia, A.X.; Zhu, Y.W.; Jin, H.; Ge, Q.Q. Short- and long-term outcomes of laparoscopic versus open surgery for rectal cancer: A systematic review and meta-analysis of randomized controlled trials. Medicine 2018, 97, e13704. [Google Scholar] [CrossRef] [PubMed]
- Fabozzi, M.; Cirillo, P.; Corcione, F. Surgical approach to right colon cancer: From open technique to robot. State of art. World J. Gastrointest. Surg. 2016, 8, 564–573. [Google Scholar] [CrossRef]
- Jurowich, C.; Lichthardt, S.; Kastner, C.; Haubitz, I.; Prock, A.; Filser, J.; Germer, C.T.; Wiegering, A. Laparoscopic versus open right hemicolectomy in colon carcinoma: A propensity score analysis of the DGAV StuDoQ|ColonCancer registry. PLoS ONE 2019, 14, e0218829. [Google Scholar] [CrossRef]
- Lindgren, P.G.; Nordgren, S.R.; Oresland, T.; Hultén, L. Midline or transverse abdominal incision for right-sided colon cancer: A randomized trial. Colorectal Dis. 2001, 3, 46–50. [Google Scholar] [CrossRef]
- Lohsiriwat, V.; Lohsiriwat, D.; Boonnuch, W.; Chinswangwatanakul, V.; Akaraviputh, T.; Methasade, A.; Lertakyamanee, N. Comparison between midline and right transverse incision in right hemicolectomy for right-sided colon cancer: A retrospective study. J. Med. Assoc. Thai 2009, 92, 1003–1008. [Google Scholar]
- Brown, S.R.; Goodfellow, P.B. Transverse verses midline incisions for abdominal surgery. Cochrane Database Syst. Rev. 2005, CD005199. [Google Scholar] [CrossRef]
- Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 December 2019).
- Veenhof, A.A.; Van der Pas, M.H.; Van der Peet, D.L.; Bonjer, H.J.; Meijerink, W.J.; Cuesta, M.A.; Engel, A.F. Laparoscopic versus transverse Incision right colectomy for colon carcinoma. Colorectal Dis. 2011, 13, e1–e5. [Google Scholar] [CrossRef]
- Tanis, E.; Van Geloven, A.A.; Bemelman, W.A.; Wind, J. A comparison of short-term outcome after laparoscopic, transverse, and midline right-sided colectomy. Int. J. Colorectal Dis. 2012, 27, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Feo, C.F.; Feo, C.V.; Fancellu, A.; Ginesu, G.C.; Cherchi, G.; Zese, M.; Targa, S.; Porcu, A. Laparoscopic versus open transverse-incision right hemicolectomy: A retrospective comparison study. ANZ J. Surg. 2019, 89, E292–E296. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A. Assessing the Influence of a Single Study in the Meta-Anyalysis Estimate. Stata Technical Bulletin. 1999, Volume 8. Available online: https://EconPapers.repec.org/RePEc:tsj:stbull:y:1999:v:8:i:47:sbe26 (accessed on 16 December 2019).
- Lohsiriwat, V.; Lohsiriwat, D.; Chinswangwatanakul, V.; Akaraviputh, T.; Lert-Akyamanee, N. Comparison of short-term outcomes between laparoscopically-assisted vs. transverse-incision open right hemicolectomy for right-sided colon cancer: A retrospective study. World J. Surg. Oncol. 2007, 5, 49. [Google Scholar] [CrossRef] [Green Version]
- Lorenzon, L.; Montebelli, F.; Mercantini, P.; Sebastiani, S.; Ziparo, V.; Ferri, M. Right Colectomy for Cancer: A Matched Comparison of Three Different Surgical Approaches. J. Investig. Surg. 2016, 29, 405–412. [Google Scholar] [CrossRef]
- Santoro, A.; Boselli, C.; Renzi, C.; Gubbiotti, F.; Grassi, V.; Di Rocco, G.; Cirocchi, R.; Redler, A. Transverse skin crease versus vertical midline incision versus laparoscopy for right hemicolectomy: A systematic review--current status of right hemicolectomy. BioMed Res. Int. 2014, 2014, 643685. [Google Scholar] [CrossRef] [Green Version]
- Arezzo, A.; Passera, R.; Ferri, V.; Gonella, F.; Cirocchi, R.; Morino, M. Laparoscopic right colectomy reduces short-term mortality and morbidity. Results of a systematic review and meta-analysis. Int. J. Colorectal Dis. 2015, 30, 1457–1472. [Google Scholar] [CrossRef]
- Rausa, E.; Kelly, M.E.; Asti, E.; Aiolfi, A.; Bonitta, G.; Bonavina, L. Right hemicolectomy: A network meta-analysis comparing open, laparoscopic-assisted, total laparoscopic, and robotic approach. Surg. Endosc. 2019, 33, 1020–1032. [Google Scholar] [CrossRef]
- Vela, N.; Bubis, L.D.; Davis, L.E.; Mahar, A.L.; Kennedy, E.; Coburn, N.G. Comparison of Patient-Reported Outcomes in Laparoscopic and Open Right Hemicolectomy: A Retrospective Cohort Study. Dis. Colon Rectum. 2019, 2, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.S.; Meng, F.C.; Lin, J.K. Procedural and post-operative complications associated with laparoscopic versus open abdominal surgery for right-sided colonic cancer resection: A systematic review and meta-analysis. Medicine 2020, 99, e22431. [Google Scholar] [CrossRef] [PubMed]
- Chaouch, M.A.; Dougaz, M.W.; Mesbehi, M.; Jerraya, H.; Nouira, R.; Khan, J.S.; Dziri, C. A meta-analysis comparing hand-assisted laparoscopic right hemicolectomyand open right hemicolectomy for right-sided colon cancer. World J. Surg. Oncol. 2020, 18, 91. [Google Scholar] [CrossRef]
- Kahokehr, A.A.; Sammour, T.; Sahakian, V.; Zargar-Shoshtari, K.; Hill, A.G. Influences on length of stay in an enhanced recovery program after colonic surgery. Colorectal Dis. 2011, 13, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Jurowich, C.; Lichthardt, S.; Matthes, N.; Kastner, C.; Haubitz, I.; Prock, A.; Filser, J.; Löb, S.; Germer, C.T.; Wiegering, A. Comparison of conventional access routes for right hemicolectomy in colon cancer-data from the DGAV StuDoQ registry. Int. J. Colorectal Dis. 2019, 34, 161–167. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and Publication Year | Country and Study Period | Type | No. | Lap | Open | Gender (M/F) | Age (Mean ± SD or Median and Range) | Anastomosis | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Lap | Open | Lap | Open | |||||||
| Lohsiriwat et al., 2007 | Thailand 2004–2006 | full-text | 33 | 13 | 20 | 6/7 | 7/13 | 56.9 ± 13.5 | 65.2 ± 16.0 | EA |
| Veenhof et al., 2011 | The Netherlands 2005–2009 | full-text | 53 | 25 | 28 | 13/12 | 9/19 | 68 (61–69) | 75 (67–78) | N/A |
| Tanis et al., 2012 | The Netherlands 2006–2009 | full-text | 53 | 30 | 23 | 12/18 | 10/13 | 75 (31–85) | 73 (54–85) | EA |
| Lorenzon et al., 2016 | Italy 2005–2014 | full-text | 80 | 40 | 40 | 17/23 | 20/20 | 70.4 ± 9.2 | 71.4 ± 11.9 | EA |
| Feo et al., 2019 | Italy 2013–2016 | full-text | 99 | 49 | 50 | 23/26 | 24/26 | 69.0 (40–84) | 70.0 (50–82) | EA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feo, C.F.; Paliogiannis, P.; Fancellu, A.; Zinellu, A.; Ginesu, G.C.; Feo, C.V.; Porcu, A. Laparoscopic versus Open Transverse-Incision Approach for Right Hemicolectomy: A Systematic Review and Meta-Analysis. Medicina 2021, 57, 80. https://doi.org/10.3390/medicina57010080
Feo CF, Paliogiannis P, Fancellu A, Zinellu A, Ginesu GC, Feo CV, Porcu A. Laparoscopic versus Open Transverse-Incision Approach for Right Hemicolectomy: A Systematic Review and Meta-Analysis. Medicina. 2021; 57(1):80. https://doi.org/10.3390/medicina57010080
Chicago/Turabian StyleFeo, Claudio F., Panagiotis Paliogiannis, Alessandro Fancellu, Angelo Zinellu, Giorgio C. Ginesu, Carlo V. Feo, and Alberto Porcu. 2021. "Laparoscopic versus Open Transverse-Incision Approach for Right Hemicolectomy: A Systematic Review and Meta-Analysis" Medicina 57, no. 1: 80. https://doi.org/10.3390/medicina57010080