Asthma: New Integrative Treatment Strategies for the Next Decades


 ,
,  , , , ,
, , , ,
Abstract
:
1. Introduction
2. Overview of Asthmatic Pathophysiology
- (a)
- Airflow obstruction: In the airway of a patient with asthma, we find the generation of hypertrophy and cellular hyperplasia, giving rise to an increase in the bronchial smooth muscle mass. Generally, this increase is induced by the fibroblasts and pericytes (also denominated Rouget cells) present in the vascular endothelium, which possess the capacity to convert into muscle cells through a process of differentiation. A bronchospasm (the sudden response of an individual with asthma) generates the contraction of the bronchial smooth muscle on being confronted with diverse stimuli, causing the narrowing of the airway with the diminution of the flow. It is known that different factors can regulate bronchial smooth muscle tone, highlighting the epithelial and endothelial cells, mastocytes, and macrophages, as well as inflammatory cells (eosinophils, lymphocytes, neutrocytes, and basophils), which release proinflammatory substances (such as histamine, eicosanoids, and platelet activating factor (PAF)). In addition, direct stimuli release acetylcholine, which induces the bronchospasm to a greater degree [2,9].
- (b)
- (c)
- Inflammation and remodeling of the airway: Inflammation, the principal contributor to the expression of asthma, generates an increase in the reactivity of the airway and recurrent episodes of wheezing, respiratory difficulty, cough, and thoracic oppression. Generally, this inflammation produces edema, angiogenesis with dilation and congestion, and smooth muscle hypertrophy and hyperplasia. Thus, the increase and size of the vessels contributes to the thickening of the bronchial wall, favoring the limitation of the airflow and generating bronchoconstriction. There is evidence that the inflammatory process produces an alteration in the respiratory epithelium. The extension of this alteration or damage may be attributed to a dysfunction in the epidermal growth factor receptors (EGFR), which regulate the epidermal growth factor (EGF), which are indispensable for normal and adequate re-epithelization. The EGF stimulates epithelial proliferation and the production of matrix metalloproteases (MMP), which degrade the extracellular matrix (ECM) and maintain an equilibrium with transforming growth factor beta (TGF-β), which increases the synthesis of the ECM components and inhibits the production of MMP [3,9,10,11,12,13].
3. Risk Factors for Asthma
4. Asthma and Its Relationship with Oxidative Stress
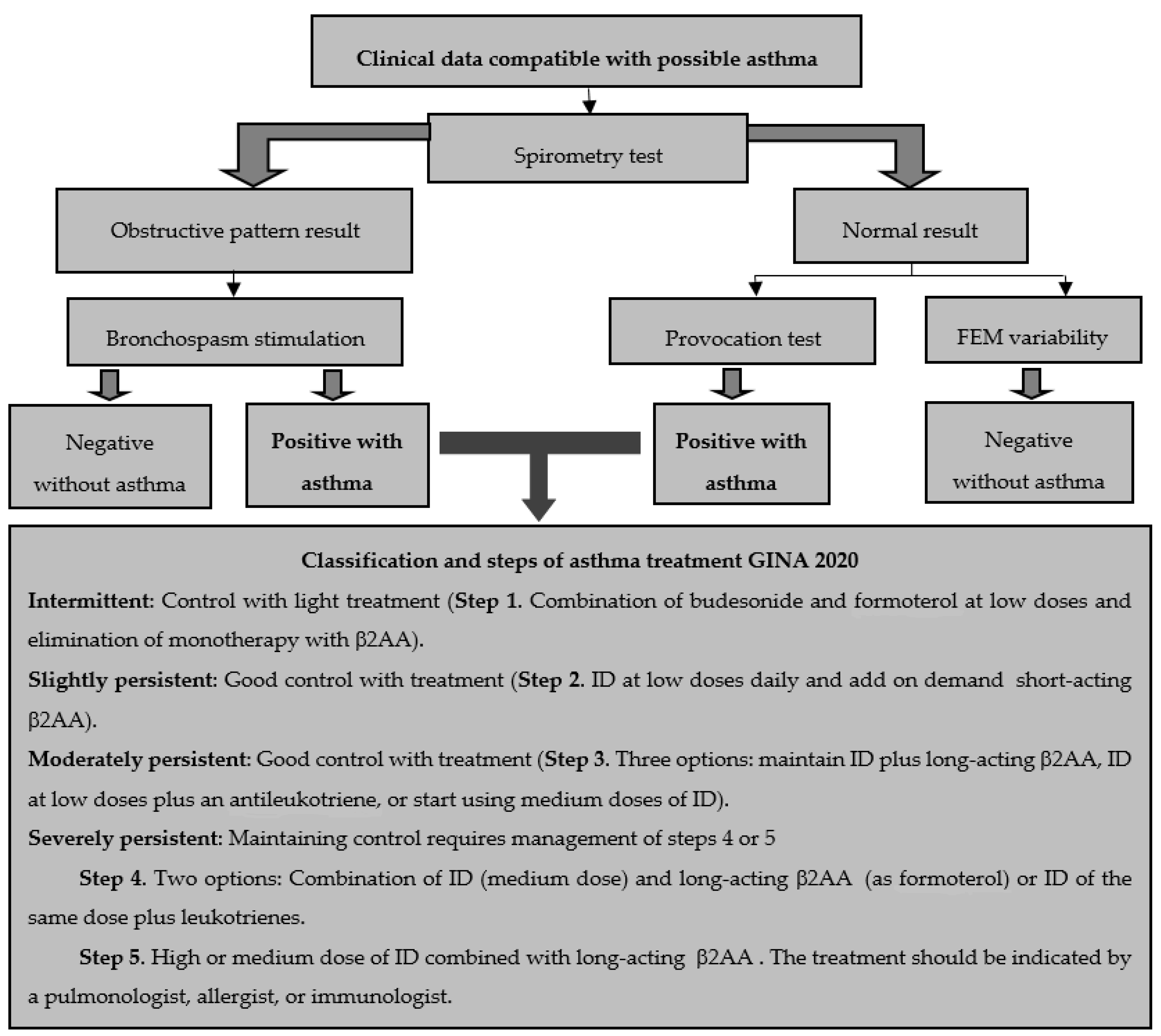
5. Classification and Diagnosis of Asthma
- (a)
- Symptom control: good control, partial control, out of control.
- (b)
- Future risk: depends on FEV1 and other factors that increase the risk of exacerbations, irreversible obstruction, or drug-associated adverse effects.
- (c)
6. Management, Control and the Main Pharmacological Treatments of Asthma
7. Alternative Therapies for Asthma Control
- (a)
- Diet, Vitamins and Food Supplements
- (b)
- Plants and Natural Extracts
- (c)
- Therapy and Integrative Medicine (IM) for Asthmatic Control
8. Perspectives and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beasley, R.; Semprini, A.; Mitchell, E.A. Risk factors for asthma: Is prevention possible? Lancet 2015, 386, 1075–1085. [Google Scholar] [CrossRef]
- The Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2006. Available online: https://ginasthma.org/wp-content/uploads/2019/01/2006-GINA.pdf (accessed on 11 May 2020).
- Del Río-Navarro, B.E.; Hidalgo-Castro, E.M.; Sienra-Monge, J.J.L. Asthma. Bol. Med. Hosp. Infant. Mex. 2009, 66, 3–33. [Google Scholar]
- Global Strategy for Asthma Management and Prevention. Global Initiative for Asthma (GINA) 2020. Available online: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf (accessed on 11 July 2020).
- Larenas-Linnemann, D.; Salas-Hernández, J.; Vázquez-García, J.C.; Ortiz-Aldana, I.; Fernández-Vega, M.; Del Río-Navarro, B.E.; Cano-Salas, M.C.; Luna-Pech, J.A.; Ortega-Martell, J.A.; Romero-Lombard, J.; et al. Mexican Asthma Guidelines: GUIMA 2017. Rev. Alerg. Mex. 2017, 64, s11–s128. [Google Scholar] [PubMed]
- Mexican Institute of Social Security (IMSS). Diagnosis, Treatment and Prevention of Exacerbation of Asthma in Adults. Evidence and Recommendations Master Catalog of Clinical Practice Guidelines: IMSS-806-17 Clinical Practice Guide. México. 2017. Available online: http://www.imss.gob.mx/sites/all/statics/guiasclinicas/806GRR.pdf (accessed on 11 May 2020).
- Plaza-Moral, V.; Alonso-Mostaza, S.; Alvarez-Rodríguez, C.; Gomez-Outes, A.; Gómez-Ruiz, F.; López-Vina, A.; Molina París, J.; Pellegrini-Belinchón, F.J.; Plaza-Zamora, J.; Quintano-Jiménez, J.A.; et al. Spanish guideline on the management of asthma. J. Investig. Allergol. Clin. Immunol. 2016, 1, 1–92. [Google Scholar] [CrossRef]
- Jeffrey, A.Y.; Hubaida, F.; Dawn, C.N. Hormones, Sex, and Asthma. Ann. Allergy Asthma Immunol. 2018, 120, 488–494. [Google Scholar]
- Durán, R. Pathophysiology of asthma: A current view. Rev. Col. Neumol. 2015, 27, 226–230. [Google Scholar]
- Jeffery, P. Inflammation and remodeling in the adult and child with asthma. Pediatr. Pulmonol. 2001, 32, 3–16. [Google Scholar] [CrossRef]
- Rasmussen, F.; Taylor, D.R.; Flannery, E.M.; Cowan, J.O.; Greene, J.M.; Herbison, G.P.; Sears, M.R. Risk factors for airway remodeling in asthma manifested by a low post bronchodilator FEV1/vital capacity ratio. Am. J. Respir. Crit. Care Med. 2002, 165, 1480–1488. [Google Scholar] [CrossRef]
- Holgate, S.T.; Davies, D.E.; Lacke, P.M.; Wilson, S.J.; Puddicombe, S.M.; Lordan, J.L. Epithelial-mesenchymal interactions in the pathogenesis of asthma. J. Allergy Clin. Immunol. 2000, 105, 193–204. [Google Scholar] [CrossRef]
- Joos, G.F. The role of neuroeffector mechanisms in the pathogenesis of asthma. Curr. Allergy Asthma Rep. 2001, 1, 134–143. [Google Scholar] [CrossRef]
- Lemanske, R.F. Inflammatory events in asthma: An expanding equation. J. Allergy Clin. Immunol. 2000, 105, S633–S636. [Google Scholar] [CrossRef] [PubMed]
- Stone, K.D.; Prussin, C.; Metcalfe, D.D. IgE, mast cell, basophils, and eosinophils. J. Allergy Clin. Immunol. 2010, 125, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Aguilar, N.E. Aetiopathogenesis, risk factors, and asthma triggers. NCT 2009, 68, S98–S110. [Google Scholar]
- Maciag, M.C.; Phipatanakul, W. Preventing the development of asthma: Stopping the allergic march. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Mota-Pinto, A.; Todo-Bom, A. The role of the epithelial cell in asthma. Rev. Port. Pneumol. 2009, 15, 461–472. [Google Scholar] [PubMed]
- Huckabee, M.M.; Peebles, R.S., Jr. Novel concepts in virally induced asthma. Clin. Mol. Allergy 2009, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Kallal, L.; Lukas, N. The Role of Chemokines in virus- associated asthma exacerbations. Curr. Allergy Asthma Rep. 2008, 8, 443–450. [Google Scholar] [CrossRef]
- Reed, C.E.; Kita, H. The role of protease activation of inflammation in allergic respiratory diseases. J. Allergy Clin. Immunol. 2004, 114, 997–1008. [Google Scholar] [CrossRef]
- Abdo, R.A.; Cué, B.M.; Álvarez, C.M. Bronchial asthma: Crisis risk factors and preventive factors. Rev. Cubana Med. Gen. Integr. 2007, 23, 1561–3038. [Google Scholar]
- Furrie, E. Probiotics and allergy. Proc. Nutr. Soc. 2005, 64, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Wood, L.H. Diet, Obesity, and Asthma. Ann. Am. Thorac. Soc. 2017, 14, S332–S338. [Google Scholar] [CrossRef] [PubMed]
- Arias-López, J.C.; Ortíz-Vidal, M.A.; Restrepo, J.C. Asthma in the pediatric population: Risk factors and diagnosis. A current revision. Salutem Sci. Spiritus 2018, 4, 35–40. [Google Scholar]
- Rodrigo, G.J.; Plaza, V. Body mass index and response to emergency department treatment in adults with severe asthma exacerbations: A prospective cohort study. Chest 2007, 132, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Shore, S.A. Obesity and asthma: Possible mechanisms. J. Allergy Clin. Immunol. 2008, 121, 1087–1093. [Google Scholar] [CrossRef]
- Forno, E.; Celedón, J.C. Health Disparities in Asthma. Am. J. Respir. Crit. Care Med. 2012, 185, 1033–1043. [Google Scholar] [CrossRef]
- Akinbami, L.J.; Moorman, J.E.; Simon, A.E.; Schoendorf, K.C. Trends in racial disparities for asthma outcomes among children 0–17 years, 2001–2010. J. Allergy Clin. Immunol. 2014, 134, 547–553. [Google Scholar] [CrossRef] [Green Version]
- Brewer, M.; Kimbro, R.T.; Denney, J.T.; Osiecki, K.M.; Moffett, B.; Lopez, K. Does neighborhood social and environmental context impact race/ethnic disparities in childhood asthma? Health Place 2017, 44, 86–93. [Google Scholar] [CrossRef]
- Schwela, D. Air pollution and health in urban areas. Rev. Environ. Health 2000, 15, 13–42. [Google Scholar] [CrossRef]
- Dreborg, S. The implications of nomenclature. Ann. Allergy Asthma Immunol. 2002, 89, 83–85. [Google Scholar] [CrossRef]
- Jindal, S.K.; Gupta, D. The relationship between tobacco smoke & bronchial asthma. Indian J. Med. Res. 2004, 120, 443–453. [Google Scholar]
- Mortimer, K.; Neugebauer, R.; Lurmann, F.; Alcorn, S.; Balmes, J.; Tager, I. Air pollution and pulmonary function in asthmatic children: Effects of prenatal and lifetime exposures. Epidemiology 2008, 19, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Tarlo, S.M. Irritant-induced asthma in the workplace. Curr. Allergy Asthma Rep. 2014, 14, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Rico-Rosillo, G.; Cambray-Gutiérrez, J.C.; Vega-Robledo, G.B. Occupational asthma. Rev. Aler. Mex. 2015, 62, 48–59. [Google Scholar]
- Bharadwaj, P.; Zivin, J.G.; Mullins, J.T.; Neidell, M. Early-Life Exposure to the Great Smog of 1952 and the Development of Asthma. Am. J. Respir. Crit. Care Med. 2016, 194, 1475–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Santos, O.; Olea-Zapata, R.; Vite-Juárez, N.E.; Gonzales-Saravia, C.A.; Rojas-Galarza, R.A.; Laurrabaquio-Miranda, A.M.; Díaz-Zúñiga, J.A. Sensitization to penicillin allergens in patients suffering from allergic diseases. VacciMonitor 2018, 27, 16–21. [Google Scholar]
- Duce-Gracia, F.; Sebastián-Ariño, A. Medicines and additives whose use may involve risk in the asthmatic patient. Med. Respir. 2013, 6, 29–38. [Google Scholar]
- Rajan, J.P.; Wineinger, N.E.; Stevenson, D.D.; White, A.A. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J. Allergy Clin. Immunol. 2015, 135, 676–681. [Google Scholar] [CrossRef]
- Ishitsuka, Y.; Kondo, Y.; Kadowaki, D. Toxicological Property of Acetaminophen: The Dark Side of a Safe Antipyretic/Analgesic Drug? Biol. Pharm. Bull. 2020, 43, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Hicks-Gómez, J.J.; Sierra-Vargas, M.P.; Olivares-Corichi, I.M.; Torres-Ramos, Y.D.; Guzmán-Grenfell, A.M. Oxidative stress in asthma. Rev. Inst. Nac. Enferm. Resp. Mex. 2005, 18, 70–78. [Google Scholar]
- Zhu, L.Y.; Ni, Z.H.; Luo, X.M.; Wang, X.B. Advance of antioxidants in asthma treatment. World J. Respirol. 2017, 7, 17–28. [Google Scholar] [CrossRef]
- Dworski, R. Oxidant stress in asthma. Thorax 2000, 2, 51–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, M.L.; Wu, W.; Fu, X.A. Tale of two controversies: Defining both role of peroxidase in nitrotyrosine formation in vivo using eosinophil peroxidase and myeloperoxidase-deficient mice, and the nature of peroxidase-generated reactive nitrogen species. J. Biol. Chem. 2002, 277, 17415–17427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.; Chen, Y.; Hazen, S.L. Eosinophil peroxidase nitrates protein tyrosyl residues. Implications for oxidative damage by nitrating intermediates in eosinophilic inflammatory disorders. J. Biol. Chem. 1999, 274, 25933–25944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuo, L.; Otenbaker, N.P.; Rose, B.A.; Salisbury, K.S. Molecular mechanisms of reactive oxygen species-related pulmonary inflammation and asthma. Mol. Immunol. 2013, 56, 57–63. [Google Scholar] [CrossRef]
- Marwick, J.A.; Tudor, C.; Khorasani, N.; Michaeloudes, C.; Bhavsar, P.K.; Chung, K.F. Oxidants induce a corticosteroid-insensitive phosphorylation of histone 3 at serine 10 in monocytes. PLoS ONE 2015, 10, e0124961. [Google Scholar] [CrossRef] [Green Version]
- Shalaby, K.H.; Allard-Coutu, A.; O’Sullivan, M.J.; Nakada, E.; Qureshi, S.T.; Day, B.J.; Martin, J.G. Inhaled birch pollen extract induces airway hyperresponsiveness via oxidative stress but independently of pollen-intrinsic NADPH oxidase activity, or the TLR4-TRIF pathway. J. Immunol. 2013, 191, 922–933. [Google Scholar] [CrossRef]
- Henricks, P.A.; Nijkamp, F.P. Reactive oxygen species as mediators in asthma. Pulm. Pharmacol. Ther. 2001, 14, 409–420. [Google Scholar] [CrossRef]
- Geraghty, P.; Hardigan, A.A.; Wallace, A.M.; Mirochnitchenko, O.; Thankachen, J.; Arellanos, L.; Thompson, V.; D’Armiento, J.M.; Foronjy, R.F. The glutathione peroxidase 1-protein tyrosine phosphatase 1B-protein phosphatase 2A axis. A key determinant of airway inflammation and alveolar destruction. Am. J. Respir. Cell Mol. Biol. 2013, 49, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Lemanske, R.F.J.; Busse, W.W. Asthma. J. Allergy Clin. Immunol. 2003, 111, S502–S519. [Google Scholar] [CrossRef]
- Gurrola-Silva, A.; Huerta-López, J.G. Asthma history. Alerg. Asma e Inmunol. Ped. 2013, 22, 77–86. [Google Scholar]
- Feldman, A.S.; He, Y.; Moore, M.L.; Hershenson, M.B.; Hartert, T.V. Toward primary prevention of asthma. Reviewing the evidence for early-life respiratory viral infections as modifiable risk factors to prevent childhood asthma. Am. J. Respir. Crit. Care Med. 2015, 191, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Quirce, S.; Bobolea, I.; Domínguez-Ortega, J.; Barranco, P. Future biological therapies in asthma. Arch. Bronconeumol. 2014, 50, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Pelaia, C.; Calabrese, C.; Terracciano, R.; De Blasio, F.; Vatrella, A.; Pelaia, G. Omalizumab, the First Available Antibody for Biological Treatment of Severe Asthma: More Than a Decade of Real-Life Effectiveness. Ther. Adv. Respir. Dis. 2018, 12, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales-González, J.A.; Madrigal-Bujaidar, E.; Sánchez-Gutiérrez, M.; Izquierdo-Vega, J.A.; Valadez-Vega, M.D.C.; Álvarez-González, I.; Morales-González, Á.; Madrigal-Santillán, E. Garlic (Allium sativum L.): A Brief Review of Its Antigenotoxic Efects. Foods 2019, 8, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Quiala, M.; Díaz-Pita, G. The effectiveness of herbal medicine in patients suffering from bronchial asthma. Rev. Cienc. Médicas 2012, 16, 118–131. [Google Scholar]
- Olivares-Corichi, I.M.; Guzmán-Grenfell, A.M.; Sierra-Vargas, M.P.; Mendoza-Atencio, R.S.; Hicks-Gómez, J.J. Prospects for the use of antioxidants as adjuvants in the treatment of asthma. Rev. Inst. Nac. Enferm. Resp. Mex. 2005, 18, 154–161. [Google Scholar]
- Barrera-Mendoza, C.C.; Ayala-Mata, F.; Cortés-Rojo, C.; García-Pérez, M.E.; Rodríguez-Orozco, A.R. Antioxidant vitamins in asthma. Rev. Alerg. Mex. 2018, 65, 61–77. [Google Scholar] [CrossRef] [Green Version]
- Wood, L.G.; Garg, M.L.; Smart, J.M.; Scott, H.A.; Barker, D.; Gibson, P.G. Manipulating antioxidant intake in asthma: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 96, 534–543. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, M.L.; Wagner, J.G.; Kala, A.; Mills, K.; Wells, H.B.; Alexis, N.E.; Lay, J.C.; Jiang, Q.; Zhang, H.; Zhou, H.; et al. Vitamin E, γ-tocopherol, reduces airway neutrophil recruitment after inhaled endotoxin challenge in rats and in healthy volunteers. Free Radic. Biol. Med. 2013, 60, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Peh, H.Y.; Ho, W.E.; Cheng, C.; Chan, T.K.; Seow, A.C.; Lim, A.Y.; Fong, C.W.; Seng, K.Y.; Ong, C.N.; Wong, W.S. Vitamin E Isoform γ-Tocotrienol Downregulates House Dust Mite-Induced Asthma. J. Immunol. 2015, 195, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Carlsten, C.; MacNutt, M.J.; Zhang, Z.; Sava, F.; Pui, M.M. Anti-oxidant N-acetylcysteine diminishes diesel exhaust-induced increased airway responsiveness in person with airway hyper-reactivity. Toxicol. Sci. 2014, 139, 479–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, C.E.; Arnold, E.; Lasserson, T.J.; Wu, T. Herbal Interventions for Chronic Asthma in Adults and Children: A Systematic Review and Meta-Analysis. Prim. Care Respir. J. 2010, 19, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shergis, J.L.; Wu, L.; Zhang, A.L.; Guo, X.; Lu, C.; Xue, C.C. Herbal medicine for adults with asthma: A systematic review. J. Asthma 2016, 53, 650–659. [Google Scholar] [CrossRef] [PubMed]
- López-Romero, D.; Izquierdo-Vega, J.A.; Morales-González, J.M.; Madrigal-Bujaidar, E.; Chamorro-Cevallos, G.; Sánchez-Gutiérrez, M.; Betanzos-Cabrera, G.; Alvarez-Gonzalez, I.; Morales-González, A.; Madrigal-Santillán, E. Evidence of Some Natural Products With Antigenotoxic Effects. Part 2: Plants, Vegetables, and Natural Resin. Nutrients 2018, 10, 1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, C.Y.; Lu, C.C.; Weng, C.J.; Yen, G.C. Protective effects of Diallyl Sulfide on ovoalbumin-induced pulmonary inflammation of allergic asthma mice by MicroRNA-144. -34a. and -34b/c-modulated Nrf2 activation. J. Agric. Food Chem. 2016, 64, 151–160. [Google Scholar] [CrossRef] [PubMed]
- André, D.M.; Calixto, M.C.; Sollon, C.; Alexandre, E.C.; Leiria, L.O.; Tobar, N.; Anhê, G.F.; Antunes, E. Therapy with resveratrol attenuates obesity-associated allergic airway inflammation in mice. Int. Immunopharmacol. 2016, 38, 298–305. [Google Scholar] [CrossRef]
- Aich, J.; Mabalirajan, U.; Ahmad, T.; Khanna, K.; Rehman, R.; Agrawal, A.; Ghosh, B. Resveratrol attenuates experimental allergic asthma in mice by restoring inositol polyphosphate 4 phosphatase (INPP4A). Int. Immunopharmacol. 2012, 14, 438–443. [Google Scholar] [CrossRef]
- George, M.; Topaz, M. A systematic review of complementary and alternative medicine for asthma self-management. Nurs. Clin. N. Am. 2013, 48, 53–149. [Google Scholar] [CrossRef] [Green Version]
- McClafferty, H. An overview of integrative therapies in asthma treatment. Curr. Allergy Asthma Rep. 2014, 14, 464–472. [Google Scholar] [CrossRef]
- Yeh, G.Y.; Horwitz, R. Integrative Medicine for Respiratory Conditions: Asthma and Chronic Obstructive Pulmonary Disease. Med. Clin. N. Am. 2017, 101, 925–941. [Google Scholar] [CrossRef]
- Kleinman, A.; Eisenberg, L.; Good, B. Culture, illness, and care: Clinical lessons from anthropologic and cross-cultural research. Ann. Intern. Med. 1978, 88, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Ewer, T.C.; Stewart, D.E. Improvement in bronchial hyper-responsiveness in patients with moderate asthma after treatment with a hypnotic technique: A randomised controlled trial. Br. Med. J. 1986, 293, 1129–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anbar, R.D. Hypnosis in pediatrics: Applications at a pediatric pulmonary center. BMC Pediatr. 2002, 2, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galantino, M.L.; Galbavy, R.; Quinn, L. Therapeutic effects of yoga for children: A systematic review of the literature. Pediatr. Phys. Ther. 2008, 20, 66–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vempati, R.; Lal Bijlani, R.; Kumar-Deepak, K. The efficacy of a comprehensive lifestyle modification programme based on yoga in the management of bronchial asthma: A randomized controlled trial. BMC Pulm. Med. 2009, 9, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Tahan, F.; Eke Gungor, H.; Bicici, E. Is yoga training beneficial for exercise-induced bronchoconstriction? Altern. Ther. Health Med. 2014, 20, 18–23. [Google Scholar]
- Pbert, L.; Madison, J.M.; Druker, S.; Olendzki, N.; Magner, R.; Reed, G.; Allison, J.; Carmody, J. Effect of mindfulness training on asthma quality of life and lung function: A randomised controlled trial. Thorax 2012, 67, 769–776. [Google Scholar] [CrossRef] [Green Version]
- Cotton, S.; Luberto, C.M.; Yi, M.S.; Tsevat, J. Complementary and alternative medicine behaviors and beliefs in urban adolescents with asthma. J. Asthma 2011, 48, 531–538. [Google Scholar] [CrossRef]
- Shen, J.; Oraka, E. Complementary and alternative medicine (CAM) use among children with current asthma. Prev. Med. 2012, 54, 27–31. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Chromosome and Region | Genes, Function and/or Association |
|---|---|
| 1q21.3, 1p31, 1q21 and 1q41 | Related to asthma and atopic march. Possible association with filaggrin, PTGR3, FLG, LELP, and TGFβ2 |
| 2q32q33 | (CTLA-4) associated with cytotoxic T lymphocytes and IgE regulation (ICOS) related to TH2 lymphocytes and cytokine activation (IL-4, IL-5, IL-13) |
| 3q21, 3p25, 3p21.3 | (CD80/86, PPARG CX3CR1) associated with asthma and exacerbations. Activation and regulation of leukotrienes and cytokines from TH1/TH2 lymphocytes |
| 4q11–q13, 4q21–23 | (CXCL9, CXCL10, CXCL11 SPP1, GSNOR) associated with asthma and rhinitis. |
| 5q31–33,35 | Increases production of IgE, eosinophils, cytokines, and interleukins (IL-4, IL-5, IL-9, and IL-13). Relationship with CD14, GRL, GM-FSC and β2AA and/or steroidal receptors |
| 6p 21.3–23, 6q25.1, 6p12 | Relationship with the inflammatory process and TNF-α. Also associated with bronchial hyperreactivity (HLA-DRB1, HLA-DQB1, IL-17F) |
| 7p14–p15 | (AOAH) susceptibility to asthma and IgE |
| 8q21 | (RIP2) associated with severe childhood asthma. |
| 9p21–22 | Susceptibility-related type I interferon gene for asthma and atopic march |
| 10q 11.2.10q24 | (5-LO, PLAU) associated with asthmatic pathogenesis |
| 11q12–13,11p13 | Regulates the beta chain of the receptor for IgE. Additionally associated with anti-inflammatory lung proteins (CC16, CC10. CAT and BDNF). |
| 12q13-24,12q14 and 12q22 | Genes related to asthmatic development (early onset and exacerbations) |
| 14q11.2, 14q32.3, 14q24–q31 | Genes related to childhood asthma. They are also associated with increased bronchial hyperresponsiveness and decreased response to bronchodilator drugs |
| 16p13.13, 16q24.1, 16p11 | (SOCS1) related to adult asthma and atopic march. Possible activation of IL-4 and IL-27. |
| 17q12–q21 | (ORMDL3) relationship with early onset of asthma |
| 19q13.1–13.3 | (PLAUR) increases synthesis of IgE. |
| 20p31, 20q11.2q13.1, 20q12–q13.2 | Possible activation of ADAM 33, MMP9 and CD40 associated with childhood asthma, bronchial hyperactivity and IgE. |
| 21q22.3 | (RUNX1) relationship with asthma and IgE |
| Xp21, Xq13.2–21.1 and CySLTR1 | Associated with atopic march and asthma induced by NSAIDs |
| Agent | Exposure Sites and Individuals | Type of Asthma |
|---|---|---|
| Wood dust (cedar, mahogany, ebony, pine and oak) | Carpenters, furniture makers, sawmills | Occupational |
| Grains (pollen, wheat, barley, coffee, tobacco) | Beekeepers, farmers, bakers, beer industry workers | Occupational |
| Urine and animal hair | Veterinarians, ranchers, farmers, merchants, daily life (home) | Occupational/environmental |
| Irritating reagents and/or chemicals (dyes, acid anhydrides, polyisocyanate polymers, and platinum and persulfate salts) | Textile workers, hairdressers, stylists, polyurethane producers, car paint, glue users | Occupational/environmental |
| Dandruff residue | General employees (offices), daily life (home) | Occupational/environmental |
| Proteases (mites and fungi) | Field, offices, hospitals, daily life (home) | Occupational/environmental |
| Suspended particles (CO, NO2, SO2, O3, diesel) | Gas station and refinery employees. Daily life | Occupational/environmental |
| Tobacco smoke | Employees and workers in general. Daily life | Occupational/environmental |
| Latex | Health professionals, anyone who uses it | Occupational/environmental |
| Others (climate changes and stress) | Daily life, employees in general | Occupational/environmental |
| Medicines (β-lactams and NSAIDs) | Health professionals, daily life (home) | Pharmacological |
| Number | Objectives |
|---|---|
| 1 | Absence and/or decrease in chronic symptoms |
| 2 | Reduce the frequency of exacerbations |
| 3 | Encourage a normal lifestyle without limitations that allows exercise |
| 4 | Maintain normal lung function with minimal adverse effects during treatment |
| 5 | Decrease the need to use rescue treatments |
| Pharmacological Group | Name (s) | Mechanism of Action | Adverse Effects |
|---|---|---|---|
| Bronchodilator Potential | |||
| β2 Adrenergic Agonists |
First-line drugs. Albuterol, Terbutaline, Pirbuterol and Levalbuterol (Short Action) Formoterol, arformoterol, idacaterol and salmeterol (Long-acting) | They activate adenyl cyclase through the β2AA-receptor and relax smooth muscle, increase mucociliary clearance, and decrease vascular permeability | Uncommon when administered by inhalation. Mainly: Tachycardia, hyperglycemia, hypokalemia, and fine tremors |
| Anticholinergics | Second-line drugs Ipatropium bromide, and tiotropium bromide. Atropine (prototype agent) | They block the constriction of the smooth muscle of the airways and the secretion of mucus to the muscarinic receptors (M2, M3) of the lung | Atropine: produces thick secretions, blurred vision and cardiac stimulation (all of them limiting its use). Ipatropium bromide: antagonizes both receptors (M3/M2) causing bronchodilation/bronchoconstriction. Effects related to bronchitis, exacerbation of COPD and headaches |
| Methylxanthines | Third or fourth line drug Theophylline | Ability to relax the bronchial smooth muscle and pulmonary vessels. Its effect is related to the non-selective inhibition of phosphodiesterase. | According to international guides, its use in children has decreased. Short and long-term effects related to nausea, vomiting, arrhythmias, and gastrointestinal bleeding |
| Control of inflammation | |||
| Corticosteroids | Beclomethasone Dipropionate Budesonide Fluticasone propionate Ciclesonide Mometasone | Inhalable agents (sometimes administered systemically) that inhibit the inflammatory response by preventing the release of phospholipase A2 and inflammatory cytokines | High and/or accumulated doses can produce suppression of the hypothalamic–pituitary–adrenal glands axis, osteoporosis, cataracts, skin atrophy, weight gain, diabetes, hypertension, psychological disorders and immunosuppression |
| Antileukotrienes | Zileuton (a) Zafirlukast, montelukast pobilukast and pranlukast (b) | Two mechanisms of action: (a) Inhibition of the enzyme 5-lipooxygenase and (b) antagonistic effect of the cysteinyl leukotriene-1-receptor (CysLT1) | They can cause headache, rash, insomnia, dizziness, tremor, nausea, vomiting, abdominal pain, heartburn, diarrhea, anorexia, constipation, increased liver enzymes, leukopenia, thrombocytopenia, fever, edema, alopecia, and menstrual irregularities |
| Chromones | Cromolin (Sodium chromoglycate) Nedocromil | They phosphorylate a myosin-like protein in the cell membrane, responsible for the release of mediators from mast cells and prevent the release of histamine | They appear to have a high safety profile, so they can be used in infants and children under the age of two. In general, they cause irritation in the throat and cough when inhaled. While orally they can cause headache and diarrhea |
| Agent | Characteristic and/or Property |
|---|---|
| MoAb anti IgE | |
| Quilizumab 8D6 | 8D6 has an affinity for a conformational epitope in the CH3 domain of IgE. Unlike omalizumab, it can bind to low affinity receptors making it more competitive. The other agent has been studied subcutaneously in three doses (150, 300 and 450 mg) in patients with uncontrolled allergic asthma with ID |
| MoAb anti IL-5 | |
| Mepolizumab Reslizumab Benralizumab TPI-ASM8 | IL-5 is a cytosine modulator of chemotaxis and degranulation of eosinophils. Its receptor is composed of two subunits: (a) specific subunit-α (IL-5Rα) for IL-5 and (b) βc subunit (IL-5Rcβ) responsible for the transduction signal that is shared with specific α subunits of IL-3 receptors and macrophage and granulocyte colony stimulating factor (GM-CSF). Mepolizumab (best known monoclonal antibodies (MoAb) from this group) and together with Reslizumab neutralize IL-5. While Benralizumab acts on IL-5Rα and TPI-ASM8 on IL-5Rβc |
| IL-4 Antagonists | |
| Pascolizumab Altrakincept Pitrakinra Dulipumab | Both IL-4 and IL-13 play an important role in TH2 and B lymphocyte responses for IgE synthesis. Despite the fact that both interleukins have different actions in asthma, most of the MoAb are in development or some controlled evaluation studies are being initiated |
| MoAb IL-13 | |
| Lebrikizumab Anrukinzumab Tralokinumab | All three MoAbs are under evaluation in controlled clinical trials. The main information found corresponds to Anrukinzumab and lebrikizumab. The former has been tested in patients with mild allergic asthma showing a slight reduction in asthmatic responses, while lebrikizumab has been administered subcutaneously to individuals with uncontrolled moderate to severe persistent asthma |
| Anti-IL-9 monoclonal antibodies | |
| MEDI-528 | IL-9 (produced by TH2 lymphocytes and mast cells) has shown to have an increased expression in the airways of asthmatic individuals. Studies evaluating subjects with mild and moderate asthma suggested that MEDI-528 binds this interleukin and has an acceptable safety profile and a decrease in exacerbations and FEV1 after doing physical exercise. |
| Anti-TNF-α | |
| Etanercept Infliximab Adalimumab Golimumab | The four MoAb agents are still under evaluation. Etanercept is a dimeric protein that binds to free TNF-α by neutralizing it; however, it has not shown improvement in any asthmatic parameter so far. While in a single study, golimumab apparently had action on severe asthma. Infliximab (considered for moderate persistent asthma) and adalimumab (tested for severe chronic asthma) have apparently shown reduced exacerbations. Unfortunately, there are no verifying results of its efficacy and safety |
| MoAb against T cells | |
| Daclizumab Keliximab Oxelumab KB003 | There is little information on these drugs. Inflammation of the airway is known to involve the activation of T lymphocytes, with an increase in T CD25 + cells, in concentrations of IL-2, and a chain receptor of soluble IL-2 (IL-2R). In a single study, daclizumab was confirmed to act on this receptor and appears to have activity against uncontrolled moderate-severe asthma. Apparently, Oxelumab has an effect in patients with controlled mild allergic asthma by blocking OX40. This mechanism is related to the costimulation between the dendritic cell and the T lymphocyte. On the other hand, KB003 has shown changes in FEV1 and lowered the number of exacerbations in individuals with uncontrolled moderate to severe asthma. Keliximab has only been used in the treatment of rheumatoid arthritis |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arteaga-Badillo, D.A.; Portillo-Reyes, J.; Vargas-Mendoza, N.; Morales-González, J.A.; Izquierdo-Vega, J.A.; Sánchez-Gutiérrez, M.; Álvarez-González, I.; Morales-González, Á.; Madrigal-Bujaidar, E.; Madrigal-Santillán, E. Asthma: New Integrative Treatment Strategies for the Next Decades. Medicina 2020, 56, 438. https://doi.org/10.3390/medicina56090438
Arteaga-Badillo DA, Portillo-Reyes J, Vargas-Mendoza N, Morales-González JA, Izquierdo-Vega JA, Sánchez-Gutiérrez M, Álvarez-González I, Morales-González Á, Madrigal-Bujaidar E, Madrigal-Santillán E. Asthma: New Integrative Treatment Strategies for the Next Decades. Medicina. 2020; 56(9):438. https://doi.org/10.3390/medicina56090438
Chicago/Turabian StyleArteaga-Badillo, Diego A., Jacqueline Portillo-Reyes, Nancy Vargas-Mendoza, José A. Morales-González, Jeannett A. Izquierdo-Vega, Manuel Sánchez-Gutiérrez, Isela Álvarez-González, Ángel Morales-González, Eduardo Madrigal-Bujaidar, and Eduardo Madrigal-Santillán. 2020. "Asthma: New Integrative Treatment Strategies for the Next Decades" Medicina 56, no. 9: 438. https://doi.org/10.3390/medicina56090438