Residential Links to Air Pollution and School Children with Asthma in Vilnius (Population Study)



Abstract
:1. Introduction
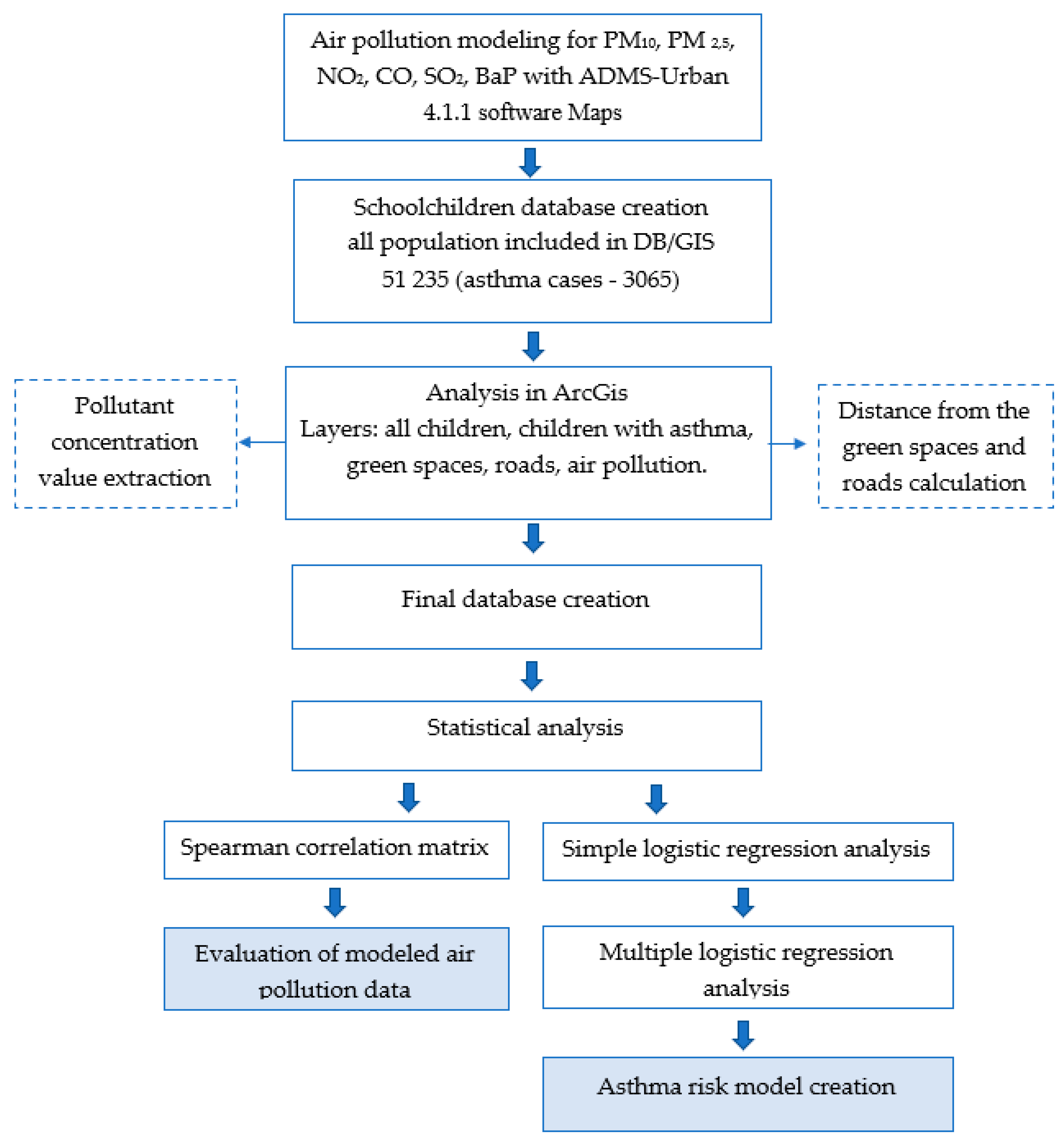
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/ceh/publications/Advance-copy-Oct24_18150_Air-Pollution-and-Child-Health-merged-compressed.pdf?ua=1 (accessed on 5 May 2020).
- Ranzi, A.; Porta, D.; Badaloni, C.; Cesaroni, G.; Lauriola, P.; Davoli, M.; Forastiere, F. Exposure to air pollution and respiratory symptoms during the first 7 years of life in an Italian birth cohort. Occup. Environ. Med. 2014, 71, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Ou, C.; Chen, J.; Xiang, Y. Particle deposition in tracheobronchial airways of an infant, child and adult. Sci. Total Environ. 2018, 612, 339–346. [Google Scholar] [CrossRef]
- Bateson, T.F.; Schwartz, J. Children’s Response to Air Pollutants. J. Toxicol. Environ. Health Part A 2007, 71, 238–243. [Google Scholar] [CrossRef]
- Choi, H.; Dostal, M.; Pastorkova, A.; Rossner, P.; Šrám, R.; Ho, S.-M. Greater susceptibility of girls to airborne Benzo[a]pyrene for obesity-associated childhood asthma. Environ. Int. 2018, 121, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, C.; Worm, M.; Leynaert, B. Impact of gender on asthma in childhood and adolescence: A GA2LEN review. Allergy 2007, 63, 47–57. [Google Scholar] [CrossRef]
- Dijk, F.N.; De Jongste, J.C.; Postma, D.S.; Koppelman, G.H. Genetics of onset of asthma. Curr. Opin. Allergy Clin. Immunol. 2013, 13, 193–202. [Google Scholar] [CrossRef]
- European Environment Agency. Available online: https://www.eea.europa.eu/publications/european-union-emission-inventory-report-1 (accessed on 5 October 2019).
- Kim, J.J.; Huen, K.; Adams, S.; Smorodinsky, S.; Hoats, A.; Malig, B.; Lipsett, M.; Ostro, B.D. Residential Traffic and Children’s Respiratory Health. Environ. Health Perspect. 2008, 116, 1274–1279. [Google Scholar] [CrossRef] [Green Version]
- Farrell, W.J.; Cavellin, L.D.; Weichenthal, S.; Goldberg, M.; Hatzopoulou, M. Capturing the urban canyon effect on particle number concentrations across a large road network using spatial analysis tools. Build Environ. 2015, 92, 328–334. [Google Scholar] [CrossRef]
- Li, Y.; Wang, S.; Chen, Q. Potential of Thirteen Urban Greening Plants to Capture Particulate Matter on Leaf Surfaces across Three Levels of Ambient Atmospheric Pollution. Int. J. Environ. Res. Public Health 2019, 16, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak, D.J.; Crane, D.E.; Stevens, J.C. Air pollution removal by urban trees and shrubs in the United States. Urban For. Urban Green. 2006, 4, 115–123. [Google Scholar] [CrossRef]
- Li, L.; E Hart, J.; Coull, B.A.; Cao, S.-J.; Spengler, J.D.; Adamkiewicz, G. Effect of Residential Greenness and Nearby Parks on Respiratory and Allergic Diseases among Middle School Adolescents in a Chinese City. Int. J. Environ. Res. Public Health 2019, 16, 991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartley, K.; Ryan, P.; Brokamp, C.; Gillespie, G.L. Effect of greenness on asthma in children: A systematic review. Public Health Nurs. 2020, 37, 453–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, K.; Weinberger, K.R.; Robinson, G.; E Sheffield, P.; Lall, R.; Mathes, R.W.; Ross, Z.; Kinney, P.L.; Matte, T. The associations between daily spring pollen counts, over-the-counter allergy medication sales, and asthma syndrome emergency department visits in New York City, 2002–2012. Environ. Health 2015, 14, 71. [Google Scholar] [CrossRef] [Green Version]
- Fuertes, E.; Markevych, I.; Bowatte, G.; Gruzieva, O.; Gehring, U.; Becker, A.; Berdel, D.; Von Berg, A.; Bergström, A.; Brauer, M.; et al. Residential greenness is differentially associated with childhood allergic rhinitis and aeroallergen sensitization in seven birth cohorts. Allergy 2016, 71, 1461–1471. [Google Scholar] [CrossRef] [Green Version]
- Barone-Adesi, F.; Dent, J.E.; Dajnak, D.; Beevers, S.; Anderson, H.R.; Kelly, F.J.; Cook, D.G.; Whincup, P.H. Long-Term Exposure to Primary Traffic Pollutants and Lung Function in Children: Cross-Sectional Study and Meta-Analysis. PLoS ONE 2015, 10, e0142565. [Google Scholar] [CrossRef]
- White, N.; teWaterNaude, J.; Van Der Walt, A.; Ravenscroft, G.; Roberts, W.; Ehrlich, R. Meteorologically estimated exposure but not distance predicts asthma symptoms in schoolchildren in the environs of a petrochemical refinery: A cross-sectional study. Environ. Health 2009, 8, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khreis, H. Early-Life Exposure to Traffic-Related Air Pollution and Risk of Development of Childhood Asthma. Ph.D. Thesis, Texas A&M University, College Station, TX, USA, 2018. [Google Scholar]
- Alizadeh, M.; Hashtroodi, L.G.; Chavoshzadeh, Z.; Rezaei, N. Effect of Air Pollution in Frequency of Hospitalizations in Asthmatic Children. Acta Med. Iran. 2016, 54, 542–546. [Google Scholar]
- Pollock, J.; Shi, L.; Gimbel, R.W. Outdoor Environment and Pediatric Asthma: An Update on the Evidence from North America. Can. Respir. J. 2017, 2017, 1–16. [Google Scholar] [CrossRef]
- Liu, L.; Poon, R.; Chen, L.; Frescura, A.-M.; Montuschi, P.; Ciabattoni, G.; Wheeler, A.; Dales, R. Acute Effects of Air Pollution on Pulmonary Function, Airway Inflammation, and Oxidative Stress in Asthmatic Children. Environ. Health Perspect. 2008, 117, 668–674. [Google Scholar] [CrossRef]
- Choi, H.; Tabashidze, N.; Rossner, P.; Dostal, M.; Pastorkova, A.; Kong, S.W.; Gmuender, H.; Šrám, R. Altered vulnerability to asthma at various levels of ambient Benzo[a]Pyrene by CTLA4, STAT4 and CYP2E1 polymorphisms. Environ. Pollut. 2017, 231, 1134–1144. [Google Scholar] [CrossRef]
- Kim, J.J.; Smorodinsky, S.; Lipsett, M.; Singer, B.C.; Hodgson, A.T.; Ostro, B. Traffic-related Air Pollution near Busy Roads. Am. J. Respir. Crit. Care Med. 2004, 170, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.; Sale, R.C.; Wakefield, J.C.; Falconer, S.; Elliott, P.; Boucher, B.J. Hospital admissions for asthma and chronic obstructive airways disease in East London hospitals and proximity of residence to main roads. J. Epidemiol. Community Health 2000, 54, 75–76. [Google Scholar] [CrossRef]
- Schikowski, T.; Sugiri, D.; Ranft, U.; Gehring, U.; Heinrich, J.; Wichmann, H.E.; Krämer, U. Long-term air pollution exposure and living close to busy roads are associated with COPD in women. Respir. Res. 2005, 6, 152. [Google Scholar] [CrossRef] [Green Version]
- Ciccone, G.; Forastiere, F.; Agabiti, N.; Biggeri, A.; Bisanti, L.; Chellini, E.; Corbo, G.; Dell’Orco, V.; Dalmasso, P.; Volante, T.F.; et al. Road traffic and adverse respiratory effects in children. SIDRIA Collaborative Group. Occup. Environ. Med. 1998, 55, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Lithuanian Environment Protection Agency. Available online: http://oras.gamta.lt/cms/index?rubricId=07c2cc60-2f42-4afb-8f3b-1e1f6452800f (accessed on 15 October 2018).
- Hesterberg, T.; Bunn, W.B.; McClellan, R.O.; Hamade, A.K.; Long, C.M.; Valberg, P.A. Critical review of the human data on short-term nitrogen dioxide (NO2) exposures: Evidence for NO2 no-effect levels. Crit. Rev. Toxicol. 2009, 39, 743–781. [Google Scholar] [CrossRef]
- Barck, C.; Lundahl, J.; Halldén, G.; Bylin, G. Brief exposures to NO2 augment the allergic inflammation in asthmatics. Environ. Res. 2005, 97, 58–66. [Google Scholar] [CrossRef]
- Chan, T.-C.; Chen, M.-L.; Lin, I.-F.; Lee, C.-H.; Chiang, P.-H.; Wang, D.-W.; Chuang, J.-H. Spatiotemporal analysis of air pollution and asthma patient visits in Taipei, Taiwan. Int. J. Health Geogr. 2009, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Achakulwisut, P.; Brauer, M.; Hystad, P.; Anenberg, S.C. Global, national, and urban burdens of paediatric asthma incidence attributable to ambient NO2 pollution: Estimates from global datasets. Lancet Planet. Health 2019, 3, e166–e178. [Google Scholar] [CrossRef] [Green Version]
- Oftedal, B.; Nystad, W.; Brunekreef, B.; Nafstad, P. Long-Term Traffic-Related Exposures and Asthma Onset in Schoolchildren in Oslo, Norway. Environ. Health Perspect. 2009, 117, 839–844. [Google Scholar] [CrossRef]
- Sheridan, C.E.; Roscoe, C.J.; Gulliver, J.; De Preux, L.; Fecht, D. Inequalities in Exposure to Nitrogen Dioxide in Parks and Playgrounds in Greater London. Int. J. Environ. Res. Public Health 2019, 16, 3194. [Google Scholar] [CrossRef] [Green Version]
- Khreis, H.; De Hoogh, K.; Nieuwenhuijsen, M.J. Full-chain health impact assessment of traffic-related air pollution and childhood asthma. Environ. Int. 2018, 114, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Ádám, L.; Molnar, F.; Izsák, F.; Havasi, Á.; Lagzi, I.; Mészáros, R. Dispersion modeling of air pollutants in the atmosphere: A review. Open Geosci. 2014, 6, 3. [Google Scholar] [CrossRef]
- Wong, D.W.S.; Yuan, L.; A Perlin, S. Comparison of spatial interpolation methods for the estimation of air quality data. J. Expo. Sci. Environ. Epidemiol. 2004, 14, 404–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Air Pollutants | Quality in 2017 Year (Data from 4 Air Quality Stations) | Air Quality Limits | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| PM10 (days) | 30 | 9 | 3 | 3 | (35 days) > 50 µg/m3 |
| PM10 µg/m3 (annual average) | 35 | 26 | 23 | 19 | 40 µg/m3 |
| PM2.5 µg/m3 (annual average) | 17 | - | - | - | 25 µg/m3 |
| NO2 µg/m3 (annual average) | 34 | 18 | 14 | 15 | 40 µg/m3 |
| SO2 µg/m3 (annual average) | - | 4.5 | 4 | 4.6 | - |
| B[a]P ng/m3 (annual average) | 1.14 | - | - | - | 1 ng/m3 (target value) |
| Age | N (All Children) | n (Children with Asthma) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | All | Boys | Girls | All | |||||||
| Count | % | Count | % | Count | % | Count | % | Count | % | Count | % | |
| 7 | 3209 | 6.3 | 3153 | 6.2 | 6362 | 12.4 | 255 | 8.3 | 161 | 5.3 | 416 | 13.6 |
| 8 | 3097 | 6.0 | 2922 | 5.7 | 6019 | 11.7 | 238 | 7.8 | 149 | 4.9 | 387 | 12.6 |
| 9 | 2871 | 5.6 | 2737 | 5.3 | 5608 | 10.9 | 246 | 8.0 | 138 | 4.5 | 384 | 12.5 |
| 10 | 2501 | 4.9 | 2393 | 4.7 | 4894 | 9.6 | 206 | 6.7 | 117 | 3.8 | 323 | 10.5 |
| 11 | 2363 | 4.6 | 2326 | 4.5 | 4689 | 9.2 | 177 | 5.8 | 100 | 3.3 | 277 | 9.0 |
| 12 | 2150 | 4.2 | 2072 | 4.0 | 4222 | 8.2 | 174 | 5.7 | 113 | 3.7 | 287 | 9.4 |
| 13 | 2109 | 4.1 | 1988 | 3.9 | 4097 | 8.0 | 151 | 4.9 | 73 | 2.4 | 224 | 7.3 |
| 14 | 1988 | 3.9 | 1848 | 3.6 | 3836 | 7.5 | 140 | 4.6 | 55 | 1.8 | 195 | 6.4 |
| 15 | 1881 | 3.7 | 1804 | 3.5 | 3685 | 7.2 | 125 | 4.1 | 62 | 2.0 | 187 | 6.1 |
| 16 | 1934 | 3.8 | 1870 | 3.6 | 3804 | 7.4 | 126 | 4.1 | 65 | 2.1 | 191 | 6.2 |
| 17 | 2058 | 4.0 | 1971 | 3.8 | 4029 | 7.9 | 126 | 4.1 | 68 | 2.2 | 194 | 6.3 |
| All | 26,161 | 51 | 25,084 | 49 | 51,245 | 100.0 | 1964 | 64.1 | 1101 | 35.9 | 3065 | 100 |
| PM10 | PM2.5 | NO2 | SO2 | CO | B[a]P | |
|---|---|---|---|---|---|---|
| PM10 | 0.97 | 0.51 | 0.17 | 0.53 | 0.74 | |
| PM2.5 | 0.97 | 0.51 | 0.17 | 0.53 | 0.74 | |
| NO2 | 0.51 | 0.51 | 0.19 | 0.85 | 0.73 | |
| SO2 | 0.17 | 0.17 | 0.19 | 0.68 | 0.22 | |
| CO | 0.53 | 0.53 | 0.85 | 0.68 | 0.65 | |
| B[a]P | 0.74 | 0.74 | 0.73 | 0.22 | 0.65 | |
| Proximity to Intensive Roads | −0.18 | −0.18 | −0.28 | −0.19 | −0.30 | −0.29 |
| Proximity to Green Spaces | 0.24 | 0.23 | 0.22 | 0.13 | 0.14 | 0.28 |
| β coef. | OR | CI 95% | p-Value | |
|---|---|---|---|---|
| Age | −0.03623 | 0.964 | (0.953 to 0.975) | <0.001 * |
| Gender (male = 1) | 0.56988 | 1.768 | (1.639 to 1.907) | <0.001 * |
| PM10 | 0.01198 | 1.012 | (1.003 to 1.021) | 0.008 * |
| PM2.5 | 0.03655 | 1.037 | (1.010 to 1.064) | 0.006 * |
| SO2 | 0.07612 | 1.079 | (0.984 to 1.184) | 0.107 |
| NO2 | 0.01635 | 1.165 | (1.005 to 1.027) | 0.003 * |
| CO | 0.44336 | 1.558 | (0.687 to 3.519) | 0.287 |
| B[a]P | 0.21984 | 1.246 | (1075 to 1.440) | 0.003 * |
| Proximity to Roads | −0.10100 | 0.904 | (0.723 to 1.123) | 0.368 |
| Proximity to Green Spaces | 0.33120 | 1.393 | (1.121 to 1.742) | 0.002 * |
| β coef. | OR | CI 95% | p-Value | |
|---|---|---|---|---|
| Age | −0.03672 | 0.964 | (0.953 to 0.975) | <0.001 * |
| Gender (male = 1) | 0.57130 | 1.770 | (1.641 to 1.911) | <0.001 * |
| NO2 | 0.01347 | 1.013 | (1.002 to 1.025) | 0.018 * |
| Proximity to Green Spaces | 0.22038 | 1.336 | (1.060 to 1.653) | 0.013 * |
| PM10 | 0.00015 | 1.0002 | (0.998 to 1.002) | 0.860 |
| PM2.5 | 0.00012 | 1.0001 | (0.998 to 1.003) | 0.925 |
| B[a]P | 0.00620 | 1.006 | (0.955 to 1.059) | 0.815 |
| β coef. | OR | CI 95% | p-Value | |
|---|---|---|---|---|
| Age | −0.05200 | 0.949 | (0.931 to 0.968) | <0.001 * |
| Gender (male = 1) | 0.30535 | 1.357 | (1.029 to 1.791) | 0.003 * |
| NO2 | 0.01340 | 1.013 | (1.002 to 1.025) | 0.019 * |
| Proximity to Green Spaces | 0.28264 | 1.327 | (1.061 to 1.654) | 0.013 * |
| Age × Gender (male = 1) | 0.02402 | 1.024 | (1.000 to 1.050) | 0.051 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alasauskas, S.; Ustinaviciene, R.; Kavaliauskas, M. Residential Links to Air Pollution and School Children with Asthma in Vilnius (Population Study). Medicina 2020, 56, 346. https://doi.org/10.3390/medicina56070346
Alasauskas S, Ustinaviciene R, Kavaliauskas M. Residential Links to Air Pollution and School Children with Asthma in Vilnius (Population Study). Medicina. 2020; 56(7):346. https://doi.org/10.3390/medicina56070346
Chicago/Turabian StyleAlasauskas, Sarunas, Ruta Ustinaviciene, and Mindaugas Kavaliauskas. 2020. "Residential Links to Air Pollution and School Children with Asthma in Vilnius (Population Study)" Medicina 56, no. 7: 346. https://doi.org/10.3390/medicina56070346