Neck Dissection for Cervical Lymph Node Metastases from Remote Primary Malignancies

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Preoperative Workup
2.3. Decision Making of the Dissection Levels in Each Case
2.4. Preoperative Detection Rate of Positive Nodes
2.5. Statistical Analysis
3. Results
3.1. Distribution of p+Ns according to Primary Site
3.2. Diagnostic Accuracy of PET+Ns for Predicting p+Ns
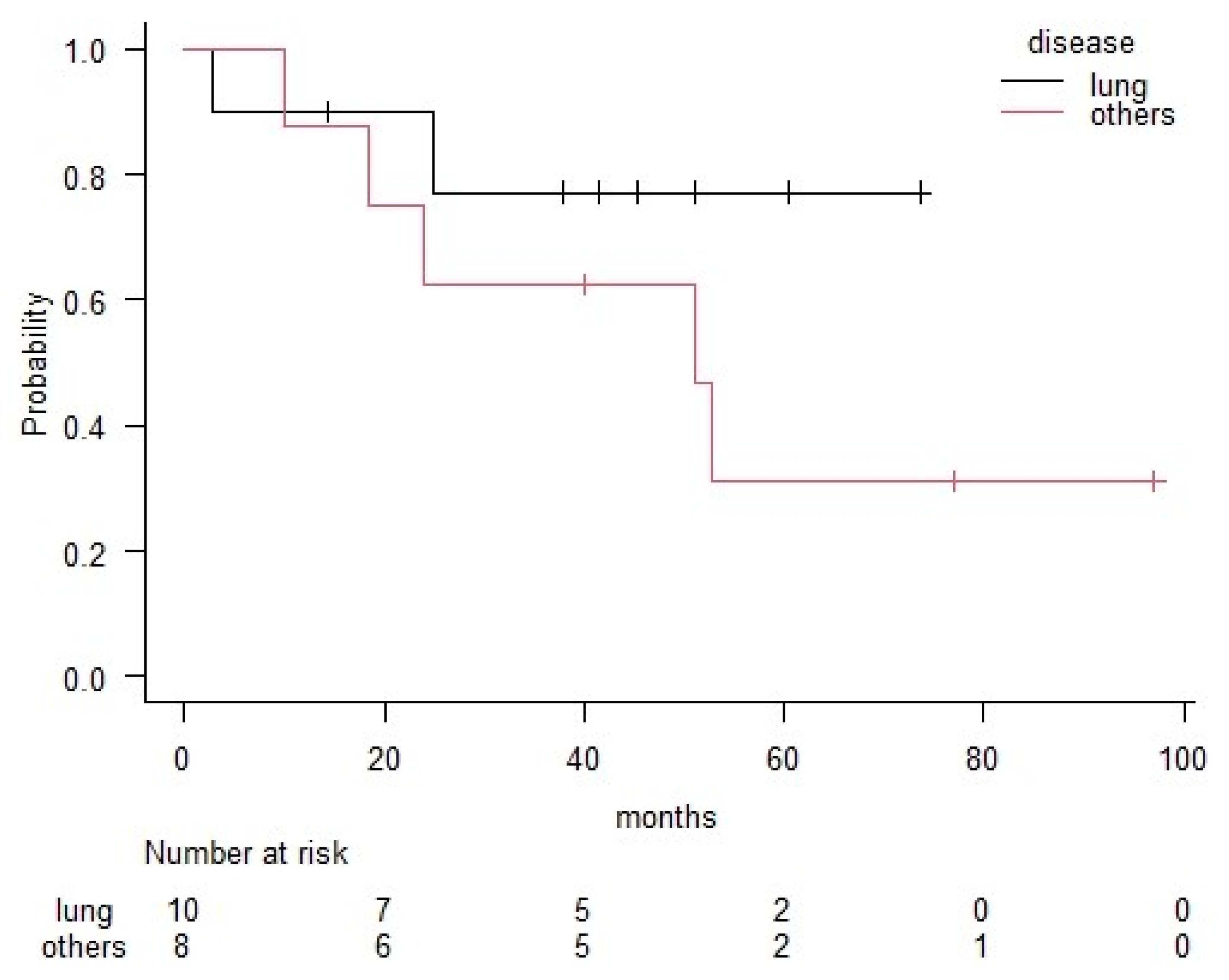
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cheng, B.; Xiong, S.; Li, C.; Liang, H.; Zhao, Y.; Li, J.; Shi, J.; Ou, L.; Chen, Z.; Liang, P.; et al. An annual review of the remarkable advances in lung cancer clinical research in 2019. J. Thorac. Dis. 2020, 12, 1056–1069. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.W.S.; Wu, M.; Cho, W.C.S.; To, K.K.W. Recent advances in the treatment of breast cancer. Front. Oncol. 2018, 8, 227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.; Feifer, A.H.; Gotto, G.T.; Kraus, D.; Motzer, R.; Bosl, G.J.; Bajorin, D.; Feldman, D.R.; Carver, B.; Sheinfeld, J. Outcomes after resection of postchemotherapy residual neck mass in patients with germ cell tumors—An update. Urology 2011, 77, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Watanabe, H.; Tachimori, Y.; Iizuka, T. Evaluation of neck lymph node dissection for thoracic esophageal carcinoma. Ann. Thorac. Surg. 1991, 51, 931–935. [Google Scholar] [CrossRef]
- Lopez, F.; Rodrigo, J.P.; Silver, C.E.; Haigentz, M., Jr.; Bishop, J.A.; Strojan, P.; Hartl, D.M.; Bradley, P.J.; Mendenhall, W.M.; Suárez, C.; et al. Cervical lymph node metastases from remote primary tumor sites. Head Neck 2016, 38 (Suppl. 1), E2374–E2385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robbins, K.T.; Clayman, G.; Levine, P.A.; Medina, J.; Sessions, R.; Shaha, A.; Som, P.; Wolf, G.T. Neck dissection classification update, revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 751–758. [Google Scholar] [CrossRef] [Green Version]
- Asakage, T.; Yokose, T.; Mukai, K.; Tsugane, S.; Tsubono, Y.; Asai, M.; Ebihara, S. Tumor thickness predicts cervical metastasis in patients with stage I/II carcinoma of the tongue. Cancer 1998, 82, 1443–1448. [Google Scholar] [CrossRef]
- Beenken, S.W.; Krontiras, H.; Maddox, W.A.; Peters, G.E.; Soong, S.; Urist, M.M. T1 and T2 squamous cell carcinoma of the oral tongue, prognostic factors and the role of elective lymph node dissection. Head Neck 1999, 21, 124–130. [Google Scholar] [CrossRef]
- The Japan Esophageal Society. Japanese Classification of Esophageal Cancer, 11th ed.; Kanehara Co., Ltd.: Tokyo, Japan, 2015; pp. 2–22. [Google Scholar]
- Herbst, R.S.; Morgensztern, D.; Boshoff, C. The biology and management of non-small cell lung cancer. Nature 2018, 553, 446–454. [Google Scholar] [CrossRef]
- Cagle, P.T.; Allen, T.C.; Olsen, R.J. Lung cancer biomarkers, present status and future developments. Arch. Pathol. Lab. Med. 2013, 137, 1191–1198. [Google Scholar] [CrossRef]
- Naylor, E.C.; Desani, J.K.; Chung, P.K. Targeted therapy and immunotherapy for lung cancer. Surg. Oncol. Clin. N. Am. 2016, 25, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, T.; Kusanale, A.; Colbert, S.; Brennan, P.A. Supraclavicular metastases from distant primaries, what is the role of the head and neck surgeon? Br. J. Oral Maxillofac. Surg. 2013, 51, 288–293. [Google Scholar] [CrossRef]
- Chen, S.C.; Chen, M.F.; Hwang, T.L.; Chao, T.C.; Lo, Y.F.; Hsueh, S.; Chang, J.T.; Leung, W.M. Prediction of supraclavicular lymph node metastasis in breast carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 614–619. [Google Scholar] [CrossRef]
- Olivotto, I.A.; Chua, B.; Allan, S.J.; Speers, C.H.; Chia, S.; Ragaz, J. Long-term survival of patients with supraclavicular metastases at diagnosis of breast cancer. J. Clin. Oncol. 2003, 21, 851–854. [Google Scholar] [CrossRef]
- Pedersen, A.N.; Moller, S.; Steffensen, K.D.; Haahr, V.; Jensen, M.; Kempel, M.M.; Jepsen, S.L.; Madsen, E.L.; Roslind, A.; Sandberg, E.; et al. Supraclavicular recurrence after early breast cancer, a curable condition? Breast Cancer Res. Treat. 2011, 125, 815–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, R.A.; Valero, V.; Buzdar, A.U.; Booser, D.J.; Ames, F.; Strom, E.; Ross, M.; Theriault, R.L.; Frye, D.; Kau, S.W.; et al. Long-term results of combined-modality therapy for locally advanced breast cancer with ipsilateral supraclavicular metastases, The University of Texas M.D. Anderson Cancer Center experience. J. Clin. Oncol. 2001, 19, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Bisase, B.; Kerawala, C. Survey of UK practice for management of breast cancer metastases to the neck. Ann. R. Coll. Surg. Engl. 2012, 94, 484–489. [Google Scholar] [CrossRef]
- Kim, J.S.; Kim, K.; Shin, K.H.; Kim, J.H.; Ahn, S.D.; Kim, S.S.; Kim, Y.B.; Chang, J.S.; Choi, D.H.; Park, W.; et al. Cervical lymph node involvement above the supraclavicular fossa in breast cancer, comparison with stage IIIC (KROG 18-02). J. Breast Cancer 2020, 23, 194–204. [Google Scholar] [CrossRef]
- The Japanese Breast Cancer Society Clinical Practice Guidelines for Breast Cancer. CQ 8b. Available online: http://jbcs.gr.jp/guidline/2018/index/gekaryoho/g4-cq-8/ (accessed on 11 June 2020).
- See, W.A.; Laurenzo, J.F.; Dreicer, R.; Hoffman, H.T. Incidence and management of testicular carcinoma metastatic to the neck. J. Urol. 1996, 155, 590–592. [Google Scholar] [CrossRef]
- Chen, J.; Wu, S.; Zheng, X.; Pan, J.; Zhu, K.; Chen, Y.; Li, J.; Liao, L.; Lin, Y.; Liao, Z. Cervical lymph node metastasis classified as regional nodal staging in thoracic esophageal squamous cell carcinoma after radical esophagectomy and three-field lymph node dissection. BMC Surg. 2014, 14, 110. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.; Hwang, Y.; Lee, H.J.; Park, I.K.; Kim, Y.T.; Kang, C.H. Patterns and prognostic significance of cervical lymph node metastasis and the efficacy of cervical node dissection in esophageal cancer. Korean J. Thorac. Cardiovasc. Surg. 2017, 50, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Roh, J.L.; Yeo, N.K.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S. Utility of 2-[18F] fluoro-2-deoxy-D-glucose positron emission tomography and positron emission tomography/computed tomography imaging in the preoperative staging of head and neck squamous cell carcinoma. Oral Oncol. 2007, 43, 887–893. [Google Scholar] [CrossRef]
- Castaldi, P.; Leccisotti, L.; Bussu, F.; Micciche, F.; Rufini, V. Role of (18)F-FDG PET-CT in head and neck squamous cell carcinoma. Acta Otorhinolaryngol. Ital. 2013, 33, 1–8. [Google Scholar] [PubMed]
- Yamazaki, Y.; Saitoh, M.; Notani, K.; Tei, K.; Totsuka, Y.; Takinami, S.; Kanegae, K.; Inubushi, M.; Tamaki, N.; Kitagawa, Y. Assessment of cervical lymph node metastases using FDG-PET in patients with head and neck cancer. Ann. Nucl. Med. 2008, 22, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuis, E.J.; Castelijns, J.A.; Pijpers, R.; van den Brekel, M.W.; Brakenhoff, R.H.; van der Waal, I.; Snow, G.B.; Leemans, C.R. Wait-and-see policy for the N0 neck in early-stage oral and oropharyngeal squamous cell carcinoma using ultrasonography-guided cytology, is there a role for identification of the sentinel node? Head Neck 2002, 24, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Borgemeester, M.C.; van den Brekel, M.W.; van Tinteren, H.; Smeele, L.E.; Pameijer, F.A.; van Velthuysen, M.L.; Balm, A.J. Ultrasound-guided aspiration cytology for the assessment of the clinically N0 neck, factors influencing its accuracy. Head Neck 2008, 30, 1505–1513. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cases | Age | Sex | Primary | Histology | Previous Treatment | Dissected Side | Adjuvant Therapy | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Surgery | CT | RT | CT | RT | ||||||
| 1 | 49 | M | Lung | Adeno. | ◯ | ◯ | L | ◯ | ||
| 2 | 61 | M | Lung | Adeno. | ◯ | ◯ | L | |||
| 3 | 67 | M | Lung | Adeno. | ◯ | R | ◯ | |||
| 4 | 71 | M | Lung | Adeno. | ◯ | ◯ | L | ◯ | ||
| 5 | 41 | F | Lung | Adeno | ◯ | ◯ | L | ◯ | ||
| 6 | 49 | F | Lung | Adeno | ◯ | ◯ | ◯ | R | ◯ | |
| 7 | 75 | F | Lung | Adeno-squamous | ◯ | ◯ | R | |||
| 8 | 51 | M | Lung | SCC | ◯ | ◯ | L | ◯ | ◯ | |
| 9 | 63 | F | Lung | SCC | ◯ | ◯ | ◯ | R | ◯ | ◯ |
| 10 | 63 | M | Lung | SCC | ◯ | ◯ | ◯ | R | ||
| 11 | 47 | F | Mammary | Adeno. | ◯ | ◯ | ◯ | R | ◯ | ◯ |
| 12 | 73 | F | Mammary | Adeno. | ◯ | ◯ | ◯ | L | ◯ | ◯ |
| 13 | 55 | M | Thymus | Malignant thymoma | ◯ | ◯ | ◯ | R | ||
| 14 | 60 | M | Esophagus | SCC | ◯ | ◯ | R | ◯ | ||
| 15 | 69 | M | Stomach | Adeno. | ◯ | ◯ | L | ◯ | ||
| 16 | 79 | F | Cervix | SCC | ◯ | ◯ | L | ◯ | ||
| 17 | 42 | F | Ovary | Endometrioid adeno. | ◯ | ◯ | L | ◯ | ||
| 18 | 30 | M | Testis | Germ cell tumor | ◯ | ◯ | L | |||
| Lung | Mammary | Thymus | Upper GI | Pelvic | Total | |
|---|---|---|---|---|---|---|
| L2 | 1/1 | 0/1 | 1/2 | |||
| L3 | 1/5 | 1/1 | 0/1 | 1/2 | 3/9 | |
| L4 | 4/5 | 1/1 | 1/1 | 2/3 | 8/10 | |
| L5 | 1/3 | 1/1 | 1/2 | 3/6 | ||
| R2 | 0/1 | 1/1 | 1/2 | |||
| R3 | 1/4 | 1/1 | 0/1 | 0/1 | 2/7 | |
| R4 | 5/5 | 1/1 | 1/1 | 0/1 | 7/8 | |
| R5 | 2/4 | 1/1 | 0/1 | 3/6 | ||
| Total | 15/28 | 6/6 | 1/3 | 2/6 | 4/7 | 28/50 |
| Case | Age | Sex | Primary | Histology | Number of LNs | Number of Levels | ||
|---|---|---|---|---|---|---|---|---|
| PET+Ns | p+Ns | PET+Ns | p+Ns | |||||
| 1 | 49 | M | Lung | Adeno. | 1 | 1 | 1 | 1 |
| 2 | 61 | M | Lung | Adeno. | 1 | 1 | 1 | 1 |
| 3 | 67 | M | Lung | Adeno. | 2 | 1 | 1 | 1 |
| 4 | 71 | M | Lung | Adeno. | 2 | 7 | 2 | 3 |
| 5 | 41 | F | Lung | Adeno. | 1 | 1 | 1 | 1 |
| 6 | 49 | F | Lung | Adeno. | 1 | 10 | 1 | 2 |
| 7 | 75 | F | Lung | Adeno-squamous | 1 | 1 | 1 | 1 |
| 8 | 51 | M | Lung | SCC | 1 | 1 | 1 | 1 |
| 9 | 63 | F | Lung | SCC | 3 | 8 | 1 | 3 |
| 10 | 63 | M | Lung | SCC | 1 | 1 | 1 | 1 |
| 11 | 47 | F | Mammary | Adeno. | 2 | 3 | 2 | 3 |
| 12 | 73 | F | Mammary | Adeno. | N/A | 17 | N/A | 3 |
| 13 | 55 | M | Thymus | Malignant thymoma | 3 | 5 | 1 | 1 |
| 14 | 60 | M | Esophagus | SCC | 1 | 1 | 1 | 1 |
| 15 | 69 | M | Stomach | Adeno. | 1 | 1 | 1 | 1 |
| 16 | 79 | F | Cervix | SCC | 1 | 20 | 1 | 3 |
| 17 | 42 | F | Ovary | Endometrioid adeno. | 1 | 1 | 1 | 1 |
| 18 | 30 | M | Testis | Germ cell tumor | 1 | 0 | 1 | 0 |
| Total | 24 | 80 | 19 | 28 | ||||
| Pathology | ||||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| PET | positive | 18 | 1 | 26 |
| negative | 8 | 7 | 8 | |
| total | 19 | 15 | 34 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shinohara, S.; Harada, H.; Kikuchi, M.; Takebayashi, S.; Hamaguchi, K. Neck Dissection for Cervical Lymph Node Metastases from Remote Primary Malignancies. Medicina 2020, 56, 343. https://doi.org/10.3390/medicina56070343
Shinohara S, Harada H, Kikuchi M, Takebayashi S, Hamaguchi K. Neck Dissection for Cervical Lymph Node Metastases from Remote Primary Malignancies. Medicina. 2020; 56(7):343. https://doi.org/10.3390/medicina56070343
Chicago/Turabian StyleShinohara, Shogo, Hiroyuki Harada, Masahiro Kikuchi, Shinji Takebayashi, and Kiyomi Hamaguchi. 2020. "Neck Dissection for Cervical Lymph Node Metastases from Remote Primary Malignancies" Medicina 56, no. 7: 343. https://doi.org/10.3390/medicina56070343