Bilateral Comparisons of Quadriceps Thickness after Anterior Cruciate Ligament Reconstruction

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
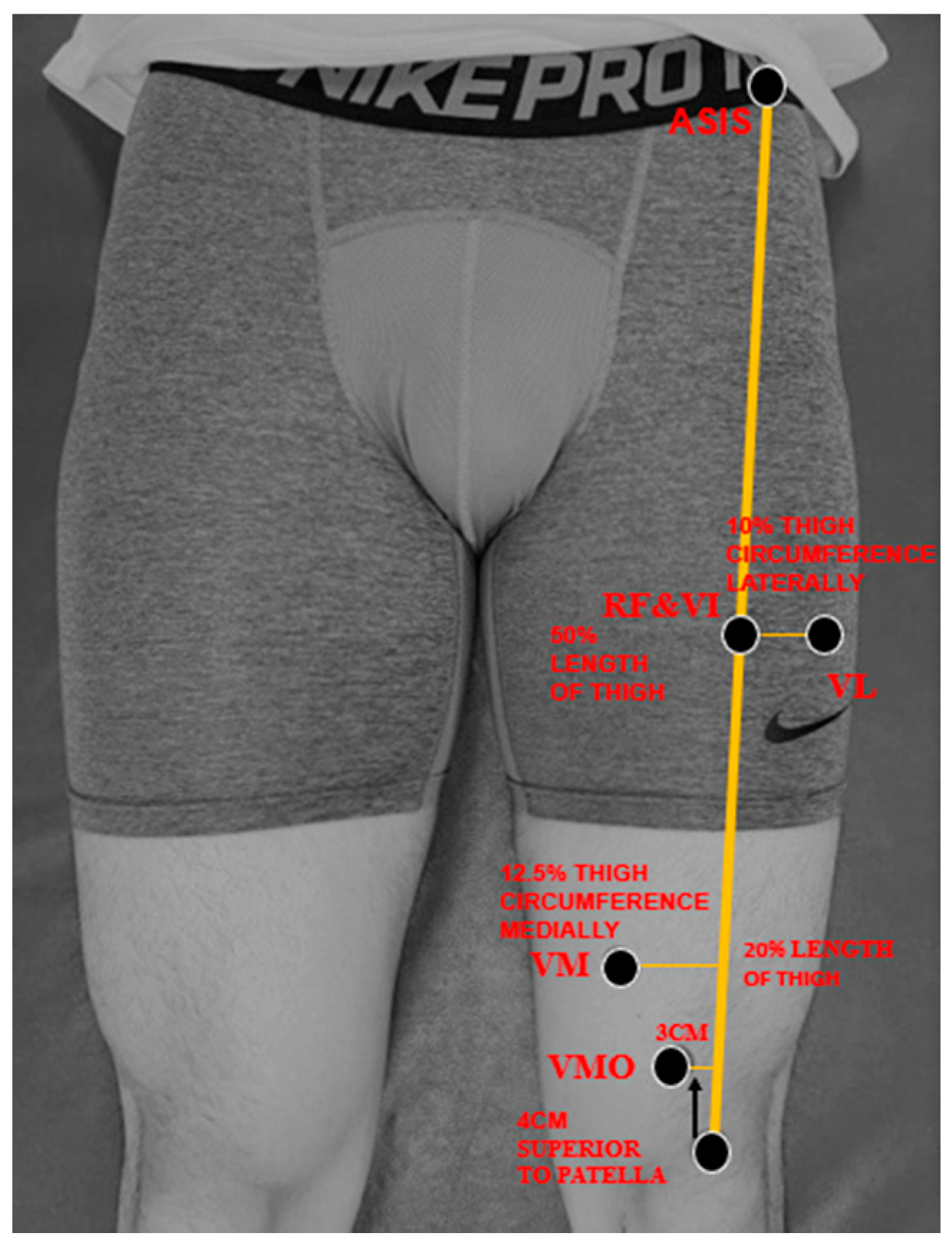
2.3. Muscle Thickness Measurement
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bates, N.A.; Hewett, T.E. Motion analysis and the anterior cruciate ligament: Classification of injury risk. J. Knee Surg. 2016, 29, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Urbach, D.; Nebelung, W.; Weiler, H.T.; Awiszus, F. Bilateral deficit of voluntary quadriceps muscle activation after unilateral ACL tear. Med. Sci. Sports Exerc. 1999, 31, 1691–1696. [Google Scholar] [CrossRef]
- Thomas, A.C.; Wojtys, E.M.; Brandon, C.; Palmieri-Smith, R.M. Muscle atrophy contributes to quadriceps weakness after anterior cruciate ligament reconstruction. J. Sci. Med. Sport 2016, 19, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, E.P.; Nader, G.A. Balancing muscle hypertrophy and atrophy. Nat. Med. 2004, 10, 584–585. [Google Scholar] [CrossRef] [PubMed]
- Vaishya, R.; Agarwal, A.K.; Ingole, S.; Vijay, V. Current trends in anterior cruciate ligament reconstruction: A review. Cureus 2015, 7, e378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukunaga, T.; Johnson, C.D.; Nicholas, S.J.; McHugh, M.P. Muscle hypotrophy, not inhibition, is responsible for quadriceps weakness during rehabilitation after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 573–579. [Google Scholar] [CrossRef]
- LaStayo, P.C.; Woolf, J.M.; Lewek, M.D.; Snyder-Mackler, L.; Reich, T.; Lindstedt, S.L. Eccentric muscle contractions: Their contribution to injury, prevention, rehabilitation, and sport. J. Orthop. Sports Phys. Ther. 2003, 33, 557–571. [Google Scholar] [CrossRef] [Green Version]
- Thomee, R.; Neeter, C.; Gustavsson, A.; Thomee, P.; Augustsson, J.; Eriksson, B.; Karlsson, J. Variability in leg muscle power and hop performance after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1143–1151. [Google Scholar] [CrossRef]
- Kuenze, C.M.; Blemker, S.S.; Hart, J.M. Quadriceps function relates to muscle size following ACL reconstruction. J. Orthop. Res. 2016, 34, 1656–1662. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.Q.; Wang, G.; Nuber, G.W.; Press, J.M.; Koh, J.L. In vivo load sharing among the quadriceps components. J. Orthop. Res. 2003, 21, 565–571. [Google Scholar] [CrossRef]
- Akima, H.; Saito, A. Inverse activation between the deeper vastus intermedius and superficial muscles in the quadriceps during dynamic knee extensions. Muscle Nerve 2013, 47, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Pincivero, D.; Lephart, S.; Moyna, N.; Karunakara, R.; Robertson, R. Neuromuscular activation and RPE in the quadriceps at low and high isometric intensities. Electroencephalogr. Clin. Neurophysiol. 1999, 39, 43–48. [Google Scholar]
- Ando, R.; Saito, A.; Umemura, Y.; Akima, H. Local architecture of the vastus intermedius is a better predictor of knee extension force than that of the other quadriceps femoris muscle heads. Clin. Physiol. Funct. Imaging 2015, 35, 376–382. [Google Scholar] [CrossRef]
- Kulas, A.S.; Schmitz, R.J.; Shultz, S.J.; Waxman, J.P.; Wang, H.M.; Kraft, R.A.; Partington, H.S. Bilateral quadriceps and hamstrings muscle volume asymmetries in healthy individuals. J. Orthop. Res. 2018, 36, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Kuenze, C.M.; Foot, N.; Saliba, S.A.; Hart, J.M. Drop-landing performance and knee-extension strength after anterior cruciate ligament reconstruction. J. Athl. Train. 2015, 50, 596–602. [Google Scholar] [CrossRef] [Green Version]
- Goetschius, J.; Kuenze, C.M.; Hart, J.M. Knee extension torque variability after exercise in ACL reconstructed knees. J. Orthop. Res. 2015, 33, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.C.; Paterno, M.V.; Ford, K.R.; Myer, G.D.; Hewett, T.E. Strength asymmetry and landing mechanics at return to sport after anterior cruciate ligament reconstruction. Med. Sci. Sports Exerc. 2015, 47, 1426–1434. [Google Scholar] [CrossRef] [Green Version]
- Evangelidis, P.E.; Massey, G.J.; Pain, M.T.; Folland, J.P. Strength and size relationships of the quadriceps and hamstrings with special reference to reciprocal muscle balance. Eur. J. Appl. Physiol. 2016, 116, 593–600. [Google Scholar] [CrossRef]
- Fukunaga, T.; Miyatani, M.; Tachi, M.; Kouzaki, M.; Kawakami, Y.; Kanehisa, H. Muscle volume is a major determinant of joint torque in humans. Acta Physiol. Scand. 2001, 172, 249–255. [Google Scholar] [CrossRef]
- Zwolski, C.; Schmitt, L.C.; Quatman-Yates, C.; Thomas, S.; Hewett, T.E.; Paterno, M.V. The influence of quadriceps strength asymmetry on patient-reported function at time of return to sport after anterior cruciate ligament reconstruction. Am. J. Sports Med. 2015, 43, 2242–2249. [Google Scholar] [CrossRef]
- Konishi, Y.; Oda, T.; Tsukazaki, S.; Kinugasa, R.; Fukubayashi, T. Relationship between quadriceps femoris muscle volume and muscle torque at least 18 months after anterior cruciate ligament reconstruction. Scand. J. Med. Sci. Sports 2012, 22, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Keays, S.L.; Bullock-Saxton, J.E.; Newcombe, P.; Keays, A.C. The relationship between knee strength and functional stability before and after anterior cruciate ligament reconstruction. J. Orthop. Res. 2003, 21, 231–237. [Google Scholar] [CrossRef]
- Yang, J.-H.; Eun, S.-P.; Park, D.-H.; Kwak, H.-B.; Chang, E. The effects of anterior cruciate ligament reconstruction on individual quadriceps muscle thickness and circulating biomarkers. Int. J. Environ. Res. Public Health 2019, 16, 4895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcon, M.; Ciritsis, B.; Laux, C.; Nanz, D.; Nguyen-Kim, T.D.L.; Fischer, M.A.; Andreisek, G.; Ulbrich, E.J. Cross-sectional area measurements versus volumetric assessment of the quadriceps femoris muscle in patients with anterior cruciate ligament reconstructions. Eur. Radiol. 2015, 25, 290–298. [Google Scholar] [CrossRef]
- Norte, G.E.; Knaus, K.R.; Kuenze, C.; Handsfield, G.G.; Meyer, C.H.; Blemker, S.S.; Hart, J.M. MRI-based assessment of lower-extremity muscle volumes in patients before and after ACL reconstruction. J. Sport Rehabil. 2018, 27, 201–212. [Google Scholar] [CrossRef]
- Delfino, G.B.; Peviani, S.M.; Durigan, J.L.; Russo, T.L.; Baptista, I.L.; Ferretti, M.; Moriscot, A.S.; Salvini, T.F. Quadriceps muscle atrophy after anterior cruciate ligament transection involves increased mRNA levels of atrogin-1, muscle ring finger 1, and myostatin. Am. J. Phys. Med. Rehabil. 2013, 92, 411–419. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Cheon, S.; Chang, E. Inter-rater reliability of a portable ultrasound for the quadriceps and hamstrings thickness measurement in healthy adults. Exerc. Sci. 2020, 29, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Ruas, C.V.; Pinto, R.S.; Lima, C.D.; Costa, P.B.; Brown, L.E. Test-retest reliability of muscle thickness, echo-intensity and cross sectional area of quadriceps and hamstrings muscle groups using B-mode ultrasound. Int. J. Knowl. Syst. Sci. 2017, 5, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, Y.; Muraoka, Y.; Kubo, K.; Suzuki, Y.; Fukunaga, T. Changes in muscle size and architecture following 20 days of bed rest. J. Gravit. Physiol. 2000, 7, 53–59. [Google Scholar]
- Giles, L.S.; Webster, K.E.; McClelland, J.A.; Cook, J. Can ultrasound measurements of muscle thickness be used to measure the size of individual quadriceps muscles in people with patellofemoral pain? Phys. Ther. Sport 2015, 16, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.S.; Correa, C.S.; Radaelli, R.; Cadore, E.L.; Brown, L.E.; Bottaro, M. Short-term strength training improves muscle quality and functional capacity of elderly women. Age (Dordr) 2014, 36, 365–372. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1988; p. 567. [Google Scholar]
- Saito, A.; Watanabe, K.; Akima, H. Coordination among thigh muscles including the vastus intermedius and adductor magnus at different cycling intensities. Hum. Mov. Sci. 2015, 40, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.; Akima, H. Neuromuscular activation of the vastus intermedius muscle during isometric hip flexion. PLoS ONE 2015, 10, e0141146. [Google Scholar] [CrossRef]
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [Green Version]
- Davies, G.J.; McCarty, E.; Provencher, M.; Manske, R.C. ACL return to sport guidelines and criteria. Curr. Rev. Musculoskelet Med. 2017, 10, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Palmieri-Smith, R.M.; Thomas, A.C. A neuromuscular mechanism of posttraumatic osteoarthritis associated with ACL injury. Exerc. Sport Sci. Rev. 2009, 37, 147–153. [Google Scholar] [CrossRef]
- Hart, J.M.; Turman, K.A.; Diduch, D.R.; Hart, J.A.; Miller, M.D. Quadriceps muscle activation and radiographic osteoarthritis following ACL revision. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 634–640. [Google Scholar] [CrossRef]
- Snyder-Mackler, L.; De, P.L.; Williams, P.R.; Eastlack, M.E. Reflex inhibition of the quadriceps femoris muscle after injury or reconstruction of the anterior cruciate ligament. J. Bone Joint Surg. 1994, 76, 555–560. [Google Scholar] [CrossRef]
- Williams, G.N.; Buchanan, T.S.; Barrance, P.J.; Axe, M.J.; Snyder-Mackler, L. Quadriceps weakness, atrophy, and activation failure in predicted noncopers after anterior cruciate ligament injury. Am. J. Sports Med. 2005, 33, 402–407. [Google Scholar] [CrossRef]
- Appell, H.-J.; Glöser, S.; Duarte, J.; Zellner, A.; Soares, J. Skeletal muscle damage during tourniquet-induced ischaemia. Eur. J. Appl. Physiol. 1993, 67, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, H.C. Tourniquet use during knee replacement surgery may contribute to muscle atrophy in older adults. Exerc. Sport Sci. Rev. 2016, 44, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiganti, M.R.; Meyer, B.C.; Chang, E.; Romanelli, D.A.; An, Y.W. Altered cortical activation after anterior cruciate ligament reconstruction during single-leg balance task. Transl. Sports Med. 2020. [Google Scholar] [CrossRef]
- Sonnery-Cottet, B.; Saithna, A.; Quelard, B.; Daggett, M.; Borade, A.; Ouanezar, H.; Thaunat, M.; Blakeney, W.G. Arthrogenic muscle inhibition after ACL reconstruction: A scoping review of the efficacy of interventions. Br. J. Sports Med. 2019, 53, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtney, C.A.; Rine, R.M. Central somatosensory changes associated with improved dynamic balance in subjects with anterior cruciate ligament deficiency. Gait Posture 2006, 24, 190–195. [Google Scholar] [CrossRef]
- Kim, H.-J.; Lee, J.-H.; Lee, D.-H. Proprioception in patients with anterior cruciate ligament tears: A meta-analysis comparing injured and uninjured limbs. Am. J. Sports Med. 2017, 45, 2916–2922. [Google Scholar] [CrossRef]
- Mendias, C.L.; Lynch, E.B.; Davis, M.E.; Sibilsky Enselman, E.R.; Harning, J.A.; DeWolf, P.D.; Makki, T.A.; Bedi, A. Changes in circulating biomarkers of muscle atrophy, inflammation, and cartilage turnover in patients undergoing anterior cruciate ligament reconstruction and rehabilitation. Am. J. Sports Med. 2013, 41, 1819–1826. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Age, years | 30.4 ± 5.9 |
| Mass, kg | 69.9 ± 10.8 |
| Height, cm | 170.8 ± 8.0 |
| Average time between injury and ACLR, days | 18.3 ± 12.1 |
| Body mass index, kg/m2 | 23.8 ± 2.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Cheon, S.; Jun, H.-P.; Huang, Y.-L.; Chang, E. Bilateral Comparisons of Quadriceps Thickness after Anterior Cruciate Ligament Reconstruction. Medicina 2020, 56, 335. https://doi.org/10.3390/medicina56070335
Lee J-H, Cheon S, Jun H-P, Huang Y-L, Chang E. Bilateral Comparisons of Quadriceps Thickness after Anterior Cruciate Ligament Reconstruction. Medicina. 2020; 56(7):335. https://doi.org/10.3390/medicina56070335
Chicago/Turabian StyleLee, Joo-Hyun, Soul Cheon, Hyung-Pil Jun, Yu-Lun Huang, and Eunwook Chang. 2020. "Bilateral Comparisons of Quadriceps Thickness after Anterior Cruciate Ligament Reconstruction" Medicina 56, no. 7: 335. https://doi.org/10.3390/medicina56070335