Active Pulmonary Tuberculosis Triggered by Interferon Beta-1b Therapy of Multiple Sclerosis: Four Case Reports and a Literature Review

 ,
,  , and
, and
Abstract
:1. Introduction
2. Case Reports
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Karussis, D. The diagnosis of multiple sclerosis and the various related demyelinating syndromes: A critical review. J. Autoimmun. 2014, 48–49, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Grebenciucova, E.; Pruitt, A. Infections in patients receiving multiple sclerosis disease-modifying therapies. Curr. Neurol. Neurosci. Rep. 2017, 17, 88. [Google Scholar] [CrossRef] [PubMed]
- Luna, G.; Alping, P.; Burman, J.; Fink, K.; Fogdell-Hahn, A.; Gunnarsson, M.; Frisell, T. Infection Risks Among Patients with Multiple Sclerosis Treated with Fingolimod, Natalizumab, Rituximab, and Injectable Therapies. JAMA Neurol. 2019, 77. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Bar-Or, A.; Comi, G.; Giovannoni, G.; Hartung, H.P.; Hemmer, B.; Lublin, F.; Montalban, X.; Rammohan, K.W.; Selmaj, K.; et al. OPERA I and OPERA II Clinical Investigators. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N. Engl. J. Med. 2017, 376, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Montalban, X.; Hauser, S.L.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Comi, G.; de Seze, J.; Giovannoni, G.; Hartung, H.P.; Hemmer, B.; et al. ORATORIO Clinical Investigators. Ocrelizumab versus placebo in primary progressive multiple sclerosis. N. Engl. J. Med. 2017, 376, 209–220. [Google Scholar] [CrossRef]
- Sanchez-Salcedo, P.; de-Torres, J.P. Immunomodulating Effects of Glatiramer Acetate and Its Potential Role in Pulmonary Tuberculosis Reactivation. Arch. Bronconeumol. (Engl. Ed.) 2015, 51, 656–657. [Google Scholar] [CrossRef]
- Epstein, D.; Dunn, J.; Deresinski, S. Infectious Complications of Multiple Sclerosis Therapies: Implications for Screening, Prophylaxis, and Management. Open Forum Infect. Dis. 2018, 5, 174. [Google Scholar] [CrossRef] [Green Version]
- Rommer, P.S.; Milo, R.; Han, M.H.; Satyanarayan, S.; Sellner, J.; Hauer, L.; Illes, Z.; Warnke, C.; Laurent, S.; Weber, M.S.; et al. Immunological Aspects of Approved MS Therapeutics. Front. Immunol. 2019, 10, 1564. [Google Scholar] [CrossRef]
- Feng, X.; Bao, R.; Li, L.; Deisenhammer, F.; Arnason, B.G.W.; Reder, A.T. Interferon-β corrects massive gene dysregulation in multiple sclerosis: Short-term and long-term effects on immune regulation and neuroprotection. EBioMedicine 2019, 49, 269–283. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.; Behr, M. Latent Mycobacterium tuberculosis Infection and Interferon-Gamma Release Assays. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Jakimovski, D.; Kolb, C.; Ramanathan, M.; Zivadinov, R.; Weinstock-Guttman, B. Interferon β for Multiple Sclerosis. Cold Spring Harb. Perspect. Med. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Tzelepis, G.E.; McCool, F.D. Respiratory dysfunction in multiple sclerosis. Respir. Med. 2015, 109, 671–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sia, J.K.; Rengarajan, J. Immunology of Mycobacterium tuberculosis infections. Microbiol. Spectr. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Banks, D.A.; Ahlbrand, S.E.; Hughitt, V.K. Mycobacterium tuberculosis Inhibits Autocrine Type I IFN Signaling to Increase Intracellular Survival. J. Immunol. 2019, 202, 2348–2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, X.; Yang, J.; Zhang, Z.; Zhang, L.; Zhu, B.; Lie, L.; Ma, L. Different Signaling Pathways Define Different Interferon-Stimulated Gene Expression during Mycobacteria Infection in Macrophages. Int. J. Mol. Sci. 2019, 20, 663. [Google Scholar] [CrossRef] [Green Version]
- Woo, M.; Wood, C.; Kwon, D.; Park, K.; Fejer, G.; Delorme, V. Mycobacterium tuberculosis Infection and Innate Responses in a New Model of Lung Alveolar Macrophages. Front. Immunol. 2018, 9, 438. [Google Scholar] [CrossRef]
- He, W.; Hu, S.; Du, X.; Wen, Q.; Zhong, X.-P.; Zhou, X.; Zhou, C.; Xiong, W.; Gao, Y.; Zhang, S.; et al. Vitamin B5 Reduces Bacterial Growth via Regulating Innate Immunity and Adaptive Immunity in Mice Infected with Mycobacterium tuberculosis. Front. Immunol. 2018, 9, 365. [Google Scholar] [CrossRef] [Green Version]
- Faridgohar, M.; Nikoueinejad, H. New findings of Toll-like receptors involved in Mycobacterium tuberculosis infection. Pathog. Glob. Health 2017, 111, 256–264. [Google Scholar] [CrossRef]
- Cheng, Y.; Schorey, J.S. Mycobacterium tuberculosis-induced IFN-β production requires cytosolic DNA and RNA sensing pathways. J. Exp. Med. 2018, 215, 2919–2935. [Google Scholar] [CrossRef] [Green Version]
- El-Sahrigy, S.A.F.; Rahman, A.M.O.A.; Samaha, D.Y. The influence of interferon-β supplemented human dendritic cells on BCG immunogenicity. J. Immunol. Methods 2018, 457, 15–21. [Google Scholar] [CrossRef]
- Dow, C.T. Proposing BCG Vaccination for Mycobacterium avium ss. paratuberculosis (MAP) Associated Autoimmune Diseases. Microorganisms 2020, 8, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki-Nakashimada, M.A.; Unzueta, A.; Berenise Gámez-González, L.; González-Saldaña, N.; Sorensen, R.U. BCG: A vaccine with multiple faces. Hum. Vaccin. Immunother. 2020, 1–10. [Google Scholar] [CrossRef]
- Lange, C.; Mandalakas, A.M.; Kalsdorf, B. Clinical Application of Interferon-γ Release Assays for the Prevention of Tuberculosis in Countries with Low Incidence. Pathog. Immun. 2016, 1, 308–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navas, C.; Torres-Duque, C.A.; Munoz-Ceron, J.; Álvarez, C.; García, J.R.; Zarco, L.; Vélez, L.A.; Awad, C.; Castro, C.A. Diagnosis and treatment of latent tuberculosis in patients with multiple sclerosis, expert consensus. On behalf of the Colombian Association of Neurology, Committee of Multiple Sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2018, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldassari, L.E.; Feng, J.; Macaron, G.; Planchon, S.M.; Alshehri, E.; Moss, B.P.; Ontaneda, D.; Willis, M.A. Tuberculosis screening in multiple sclerosis: Effect of disease-modifying therapies and lymphopenia on the prevalence of indeterminate TB screening results in the clinical setting. Mult. Scler. J. Exp. Transl. Clin. 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Graf, J.; Leussink, V.I.; Dehmel, T.; Dehmel, T.; Ringelstein, M.; Goebels, N.; Adams, O.; MacKenzie, C.R.; Warnke, C.; Feldt, T.; et al. Infectious risk stratification in multiple sclerosis patients receiving immunotherapy. Ann. Clin. Transl. Neurol. 2017, 4, 909–914. [Google Scholar] [CrossRef] [Green Version]
- Sirbu, C.A.; Budisteanu, M.; Falup-Pecurariu, C. Monoclonal antibodies—A revolutionary therapy in multiple sclerosis. Neurol. Neurochir. Pol. 2020, 54, 21–27. [Google Scholar] [CrossRef]
- Zak, D.E.; Penn-Nicholson, A.; Scriba, T.J.; Thompson, E.; Suliman, S.; Amon, L.M.; Mahomed, H.; Erasmus, M.; Whatney, W.; Hussey, G.D.; et al. A blood RNA signature for tuberculosis disease risk: A prospective cohort study. Lancet 2016, 387, 2312–2322. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Case 1 | Case 2 | Case 3 | Case 4 |
|---|---|---|---|---|
| Gender | F | M | F | F |
| MS diagnosis form | 26, RRMS | 32, SPMS | 30, RRMS | 37, RRMS |
| Age of IFNβ-1b treatment initiation | 27 | 45 | 32 | 39 |
| MRI brain scan | 2001, 2002, 2003, 2009, 2011, 2019 | 1998, 2000, 2007 | 2014, 2015, 2019 | 2006, 2008, 2015, 2018 |
| EDSS progression | 1 (2001); 5.5 (2019) | 3.5 (2000); 5.5 (2019); | 1 (2015); 4 (2019) | 1 (2007); 1.5 (2019) |
| Time between IFNβ-1b treatment initiation and TB | 12 months | 48 months | 36 months | 84 months |
| Treatments other than IFNβ-1b before TB | Methylprednisolone, antidepressants | Methylprednisolone, beta-blocker, antihypertensive, statins, antidepressants | Methylprednisolone | Methylprednisolone |
| Onset of active TB, | 28 y | 49 y | 35 y | 46 y |
| Onset of symptoms prior to TB | 6 w | 3 w | 3 w | 4 w |
| Respiratory symptoms | Hemoptysis, asthenia, weight and appetite loss, a sharp twinge in left side of chest | Asthenia, loss of appetite, productive cough, exertional dyspnea | A twinge in the left side of chest, weight loss | Asthenia, fever, persistent nonproductive cough |
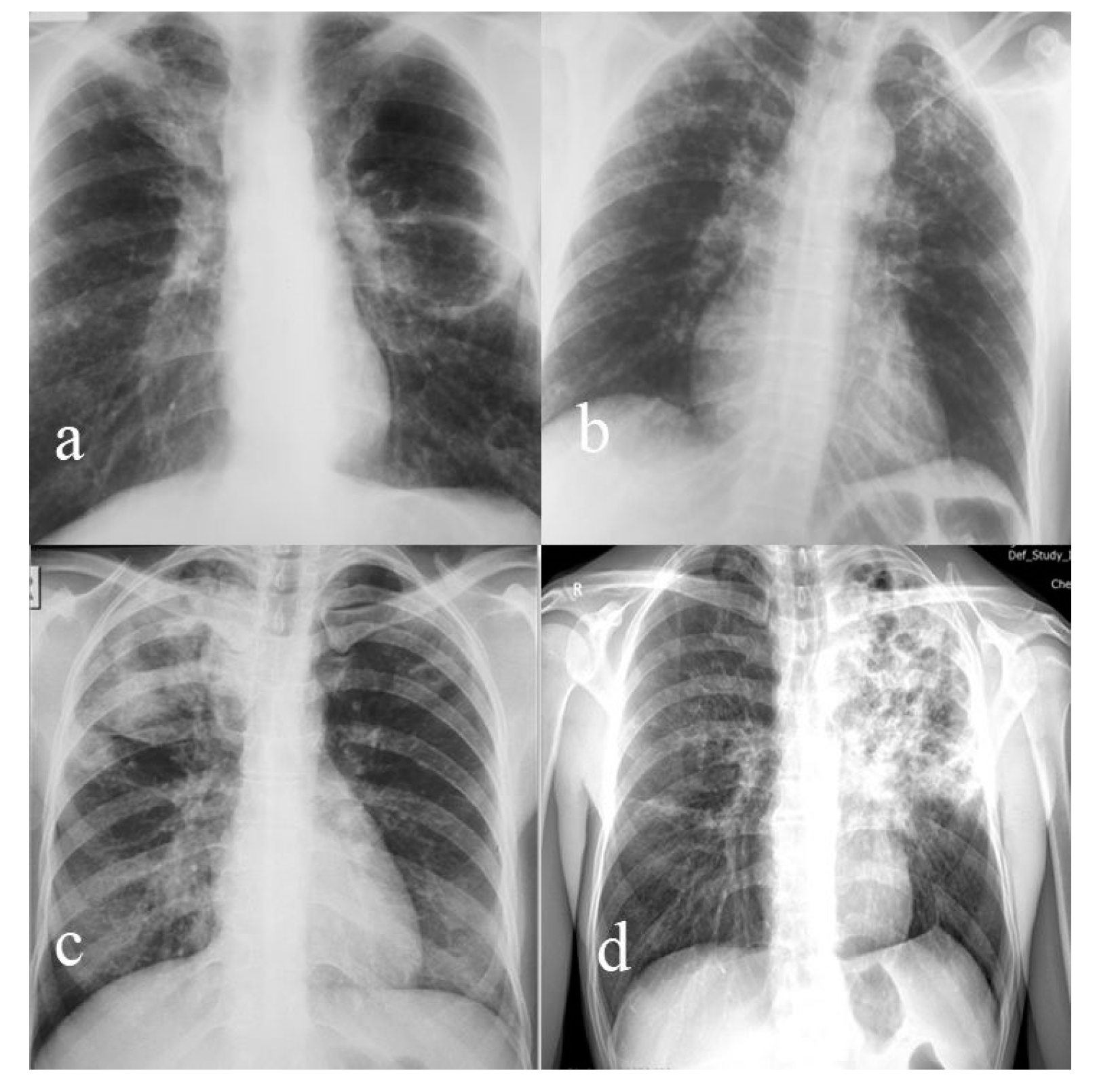
| Radiological presentation (Figure 1) | Nodular and caseous cavitary lesions | Bilateral apical ulcerated fibrocaseous lesions with bronchogenic disseminations | Caseous-cavitary lesions | Infiltrative nodular and bronchial forms |
| TB localization | Apical segment (Fowler) left lower lobe | Bilateral upper lobes | Right upper lobe | Left upper lobe |
| Initial bacteriological examination of sputum | Negative AFB smear; positive for M. tuberculosis culture | Positive smear and culture | Positive smear and culture | Negative smear, positive culture |
| Category of the treatment regimen | 2HRZS (5/7) +4HR (3/7) | 2HRZE (7/7) +4HR (3/7) | 2HRZE (7/7) + 6HR (3/7) | 3HRZOfx (7/7) + 1HROfx (7/7) +8 OfxPr (3/7) (H-intolerance) |
| Treatment duration (months) | 6 | 6 | 8 | 12 |
| Bacteriological follow up after treatment initiation | Negative at 2, 4, 6 months | Negative at 2, 4, 6 months | Negative at 2, 4, 6, 8 months | Negative at 2, 4, 6, 8 months |
| Chest X-ray after DOT treatment | Left fibronodular sequelae | Right post-TB fibronodular sequelae | Right post-TB fibronodular sequelae | Several left subclavicular fibromicronodular lesions |
| Comorbidities | Anxiety–depressive disorder, osteopenia, vitamin D deficiency, Escherichia Coli urinary tract infection | Neurocognitive disorder, arterial hypertension, dyslipidemia, vitamin D deficiency | Depressive disorder, urinary incontinence | Depressive disorder, vitamin D deficiency |
| Special considerations and particularities of the case | Recurrence with extensive caseous–cavitary TB lesions left lung 14 years later. Positive sputum smear and culture. After 11 months of Category II treatment regimen, the bacteriological follow ups at 1, 3, 5, 8, and 11 months were negative (evaluated as cured). | Bladder tumor (invasive papillary urothelial carcinoma T2bN0M0 Grade III) Left ureterohydronephrosis | - | In 1996, recurrent transient vision loss, labeled retrobulbar optic neuritis, treated for 1 year with oral corticosteroids. Received an individualized treatment regimen due to isoniazid intolerance and exclusion of E due to its ocular side effects. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirbu, C.A.; Dantes, E.; Plesa, C.F.; Docu Axelerad, A.; Ghinescu, M.C. Active Pulmonary Tuberculosis Triggered by Interferon Beta-1b Therapy of Multiple Sclerosis: Four Case Reports and a Literature Review. Medicina 2020, 56, 202. https://doi.org/10.3390/medicina56040202
Sirbu CA, Dantes E, Plesa CF, Docu Axelerad A, Ghinescu MC. Active Pulmonary Tuberculosis Triggered by Interferon Beta-1b Therapy of Multiple Sclerosis: Four Case Reports and a Literature Review. Medicina. 2020; 56(4):202. https://doi.org/10.3390/medicina56040202
Chicago/Turabian StyleSirbu, Carmen Adella, Elena Dantes, Cristina Florentina Plesa, Any Docu Axelerad, and Minerva Claudia Ghinescu. 2020. "Active Pulmonary Tuberculosis Triggered by Interferon Beta-1b Therapy of Multiple Sclerosis: Four Case Reports and a Literature Review" Medicina 56, no. 4: 202. https://doi.org/10.3390/medicina56040202