Pediatric Scoliosis Surgery—A Comprehensive Analysis of Treatment-Specific Variables and Trends in Latvia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Method, Data Acquisition, and Selection
2.2. Statistical Analysis
3. Results
3.1. Included Subjects, Gender, Age, Type of Operation Diagnosis
3.2. Curve Types and Direction
3.3. Idiopathic vs. Non-Idiopathic
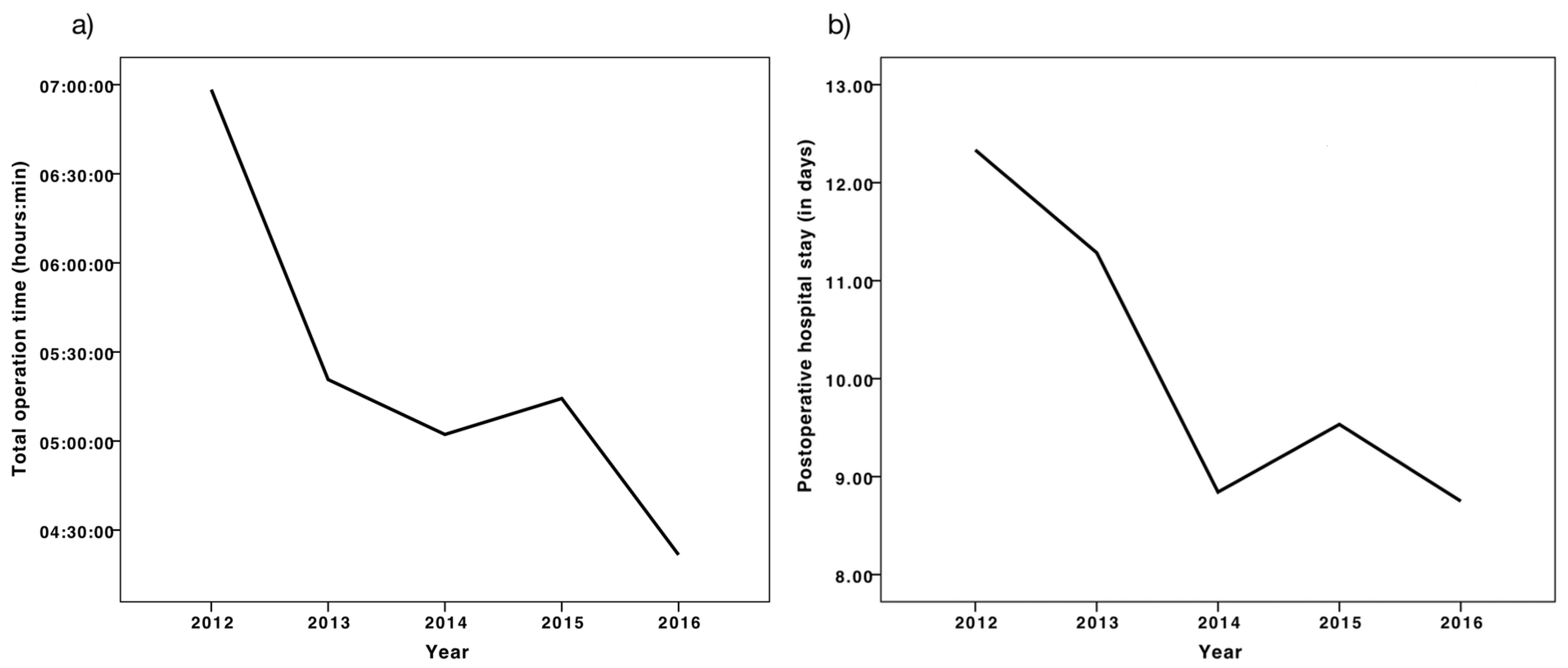
3.4. Hospital Stay, Early Postoperative Complications, Operation Time
3.5. Correlations and Regression Analysis
4. Discussion
4.1. Adolescent Idiopathic Scoliosis
4.2. Neuromuscular Scoliosis
4.3. Total Operation Time and Length of the Hospital Stay
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Variable | AAO | TOT | TVI | POHS | CAB | CAA | PC |
|---|---|---|---|---|---|---|---|
| Age at operation (AAO) | 1 | ||||||
| Total operation time (TOT) | −0.139 | 1 | |||||
| Total vertebral instrumentation (TVI) | 0.073 | 0.410 (**) | 1 | ||||
| Postoperative hospital stay (POHS) | −0.130 | 0.614 (**) | 0.526 (**) | 1 | |||
| Cobb angle before (CAB) | −0.198 | 0.478 (**) | 0.440 (**) | 0.489 (**) | 1 | ||
| Cobb angle afterwards (CAA) | −0.148 | 0.409 (**) | 0.243 (*) | 0.327 (**) | 0.530 (**) | 1 | |
| Percentage correction (%C) | 0.060 | −0.166 | −0.092 | −0.081 | −0.036 | 0.837 (**) | 1 |
References
- Huec, J.C.L.; Jouve, J.L.; Szpalski, M. Surgical techniques in pediatric spine surgery. Eur. Spine J. 2014, 23, 395–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasler, C.C. A brief overview of 100 years of history of surgical treatment for adolescent idiopathic scoliosis. J. Child. Orthop. 2013, 7, 57–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.C.; Castelein, R.M.; Chu, W.C.; Danielsson, A.J.; Dobbs, M.B.; Grivas, T.B.; Gurnett, C.A.; Luk, K.D.; Moreau, A.; Newton, P.O.; et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Primer 2015, 1, 15030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rüwald, J.M.; Eymael, R.L.; Upenieks, J.; Zhang, L.; Jacobs, C.; Pflugmacher, R.; Schildberg, F.A. An Overview of the Current State of Pediatric Scoliosis Management; Z. Georg Thieme Verlag KG Stuttgart: New York, NY, USA, 2019. [Google Scholar]
- Choudhry, M.N.; Ahmad, Z.; Verma, R. Adolescent idiopathic scoliosis. Open Orthop. J. 2016, 10, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DePaola, K.; Cuddihy, L.A. Pediatric spine disorders. Pediatr. Clin. North Am. 2020, 67, 185–204. [Google Scholar] [CrossRef]
- Cheung, Z.B.; Selverian, S.; Cho, B.H.; Ball, C.J.; Kang-Wook Cho, S. Idiopathic scoliosis in children and adolescents: Emerging techniques in surgical treatment. World Neurosurg. 2019, 130, e737–e742. [Google Scholar] [CrossRef]
- El-Hawary, R.; Chukwunyerenwa, C. Update on evaluation and treatment of scoliosis. Pediatr. Clin. North Am. 2014, 61, 1223–1241. [Google Scholar] [CrossRef]
- Haleem, S.; Nnadi, C. Scoliosis: A review. Paediatr. Child Health 2018, 28, 209–217. [Google Scholar] [CrossRef]
- Mackel, C.E.; Jada, A.; Samdani, A.F.; Stephen, J.H.; Bennett, J.T.; Baaj, A.A.; Hwang, S.W. A comprehensive review of the diagnosis and management of congenital scoliosis. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2018, 34, 2155–2171. [Google Scholar] [CrossRef]
- Janicki, J.A.; Alman, B. Scoliosis: Review of diagnosis and treatment. Paediatr. Child Health 2007, 12, 771–776. [Google Scholar] [CrossRef] [Green Version]
- Huisman, T.A.G.M. Pediatric tumors of the spine. Cancer Imaging 2009, 9, S45–S48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubousset, J. Idiopathic scoliosis. Definition--pathology--classification--etiology. Bull. Acad. Natl. Med. 1999, 183, 699–704. [Google Scholar] [PubMed]
- Trobisch, P.; Suess, O.; Schwab, F. Idiopathic scoliosis. Dtsch. Ärztebl. Int. 2010, 107, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Thacker, M.; Hui, J.H.P.; Wong, H.K.; Chatterjee, A.; Lee, E.H. Spinal fusion and instrumentation for paediatric neuromuscular scoliosis: Retrospective review. J. Orthop. Surg. 2002, 10, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, F.; Hauser, D.; Espinosa, N.; Blumenthal, S.; Min, K. Scoliosis correction with pedicle screws in Duchenne muscular dystrophy. Eur. Spine J. 2008, 17, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Pesenti, S.; Blondel, B.; Peltier, E.; Launay, F.; Fuentes, S.; Bollini, G.; Viehweger, E.; Jouve, J.-L. Experience in perioperative management of patients undergoing posterior spine fusion for neuromuscular scoliosis. BioMed Res. Int. 2016, 2016, 3053056. [Google Scholar] [CrossRef]
- Kaspiris, A.; Grivas, T.B.; Weiss, H.-R.; Turnbull, D. Surgical and conservative treatment of patients with congenital scoliosis: α search for long-term results. Scoliosis 2011, 6, 12. [Google Scholar] [CrossRef] [Green Version]
- Levy, B.J.; Schulz, J.F.; Fornari, E.D.; Wollowick, A.L. Complications associated with surgical repair of syndromic scoliosis. Scoliosis 2015, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, N.D.; Shourbaji, N.; Mitchell, P.M.; Oswald, T.S.; Devito, D.P.; Bruce, R.W. Clinical and economic implications of early discharge following posterior spinal fusion for adolescent idiopathic scoliosis. J. Child. Orthop. 2014, 8, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Unnikrishnan, R.; Renjitkumar, J.; Menon, V.K. Adolescent idiopathic scoliosis: Retrospective analysis of 235 surgically treated cases. Indian J. Orthop. 2010, 44, 35–41. [Google Scholar]
- Lee, C.S.; Hwang, C.J.; Lim, E.J.; Lee, D.-H.; Cho, J.H. A retrospective study to reveal factors associated with postoperative shoulder imbalance in patients with adolescent idiopathic scoliosis with double thoracic curve. J. Neurosurg. Pediatr. 2016, 25, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Mendenhall, S.; Mobasser, D.; Relyea, K.; Jea, A. Spinal instrumentation in infants, children, and adolescents: A review. J. Neurosurg. Pediatr. 2019, 23, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Issac, E.; Menon, G.; Vasu, B.K.; George, M.; Vasudevan, A. Predictors of postoperative ventilation in scoliosis surgery: A retrospective analysis. Anesth. Essays Res. 2018, 12, 407–411. [Google Scholar]
- Heller, A.; Melvani, R.; Thome, A.; Leamon, J.; Schwend, R.M. Predictors of variability in the length of surgery of posterior instrumented arthrodesis in patients with adolescent idiopathic scoliosis. J. Pediatr. Orthop. B 2016, 25, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Bao, H.; Yan, P.; Liu, S.; Zhu, Z.; Liu, Z.; Bao, M.; Qiu, Y. Comparison of surgical outcome of adolescent idiopathic scoliosis and young adult idiopathic scoliosis: A match-pair analysis of 160 patients. Spine 2017, 42, E1133–E1139. [Google Scholar] [CrossRef] [PubMed]
- Rumalla, K.; Yarbrough, C.K.; Pugely, A.J.; Koester, L.; Dorward, I.G. Spinal fusion for pediatric neuromuscular scoliosis: National trends, complications, and in-hospital outcomes. J. Neurosurg. Spine 2016, 25, 500–508. [Google Scholar] [CrossRef]
- Nordon, D.G.; Lugão, A.F.; Machado, L.C.C.; Marcon, R.M.; Cristante, A.F.; de Barros Filho, T.E.P.; Letaif, O.B. Correlation between the degree of correction of neuromuscular scoliosis and patient quality of life. Clinics 2017, 72, 71–80. [Google Scholar] [CrossRef]
- Ryu, K.J.; Suh, S.W.; Kim, H.W.; Lee, D.H.; Yoon, Y.; Hwang, J.H. Quantitative analysis of a spinal surgeon’s learning curve for scoliosis surgery. Bone Jt. J. 2016, 98, 679–685. [Google Scholar] [CrossRef]
- Procter, L.D.; Davenport, D.L.; Bernard, A.C.; Zwischenberger, J.B. General surgical operative duration is associated with increased risk-adjusted infectious complication rates and length of hospital stay. J. Am. Coll. Surg. 2010, 210, 60–65.e1–2. [Google Scholar] [CrossRef]
- Kudo, D.; Miyakoshi, N.; Hongo, M.; Kasukawa, Y.; Ishikawa, Y.; Mizutani, T.; Shimada, Y. Relationship between preoperative serum rapid turnover proteins and early-stage surgical wound infection after spine surgery. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2017, 26, 3156–3161. [Google Scholar] [CrossRef]
- Garbarino, L.J.; Gold, P.A.; Sodhi, N.; Anis, H.K.; Ehiorobo, J.O.; Boraiah, S.; Danoff, J.R.; Rasquinha, V.J.; Higuera-Rueda, C.A.; Mont, M.A. The effect of operative time on in-hospital length of stay in revision total knee arthroplasty. Ann. Transl. Med. 2019, 7, 66. [Google Scholar] [CrossRef] [PubMed]

| Congenital: Failure of formation, Failure of segmentation | Idiopathic: Infantile (0–3 years) Juvenile (3–10 years) Adolescent (10+ years until skeletal maturity) |
| Neuromuscular: (1) Myopathic: Arthrogryposis, Muscular dystrophy (2) Neuropathic: Upper Motor Neuron, Lower Motor Neuron, Dysautonomia | Others: Neurofibromatosis, Mesenchymal (Marfan’s, Ehler-Danlos), Traumatic, Tumors, Osteochondrodystrophies |
| Category | Specific Cause | N |
|---|---|---|
| General | Lung related complications (infection, embolism) | 0 |
| Prolonged ICU stay (>2 days for posterior, >3 days for anterior-posterior approach) | 2 | |
| Development of pressure ulcer | 1 | |
| Anemia requiring blood transfusion | 3 | |
| Wound related | Surgical wound complications (skin closure defects, infection) | 1 |
| Neurologic | Neurologic complications (neurological deficits) | 1 |
| Urinary retention (requiring catheterization) and postoperative ileus | 1 | |
| Instrumentation | Early revision surgery (problems with drainage, closure, infection, screw malposition) | 2 |
| Death | 0 |
| Diagnostic Groups | % (n) | Mean Age at Surgery | SD |
|---|---|---|---|
| All | 100 (69) | 14.6 | 2.9 |
| Idiopathic scoliosis | 62.3 (43) | 15.4 | 2.1 |
| 52.2 (36) | 16.0 | 1.5 |
| 10.1 (7) | 11.9 | 1.1 |
| 0 | - | - |
| Non-idiopathic scoliosis | 37.7 (26) | 13.4 | 3.7 |
| 24.6 (17) | 13.8 | 3.8 |
| 7.2 (5) | 12.6 | 3.5 |
| 5.8 (4) | 12.8 | 4.1 |
| Variable | Idiopathic | (AIS) | Non-Idiopathic | (NEU) | p |
|---|---|---|---|---|---|
| Age at operation (in years) | 15.4 ± 2.1 | (16.0 ± 1.5) | 13.4 ± 3.7 | (13.8 ± 3.8) | ** (**) |
| Total operation time (h:mm) | 4:46 ± 1:05 | (4:50 ± 1:07) | 6:05 ± 1:45 | (6:12 ± 1:39) | ** (**) |
| N° of vertebrae instrumented | 9.1 ± 1.8 | (9.7 ± 1.9) | 10.7 ± 3.7 | (12.5 ± 2.7) | 0.062 (***) |
| Postoperative hospital stay (in days) | 9.2 ± 1.9 | (9.2 ± 2.0) | 11.2 ± 3.1 | (11.8 ± 2.6) | ** (**) |
| Cobb angle before (Cobb°) | 55.8 ± 14.7 | (56.3 ± 15.3) | 75.1 ± 23.6 | (78.7 ± 20.0) | ** (***) |
| Cobb angle afterwards (Cobb°) | 21.1 ± 9.0 | (20.9 ± 9.2) | 37.0 ± 18.4 | (39.2 ± 19.4) | *** (***) |
| Percentage decrease (%) | 62.0 ± 13.7 | (62.6 ± 13.9) | 49.7 ± 20.1 | (49.7 ± 21.1) | * (*) |
| Associations with PCs | Without PC | MC with PC | p-Value |
|---|---|---|---|
| Age at operation (in years) | 14.5 ± 2.9 | +0.9 | 0.818 |
| Total operation time (hh:mm) | 5:01 ± 1:09 | +1:33 | 0.056 |
| N° of vertebrae instrumented | 9.7 ± 2.6 | +2.4 | * |
| Postoperative hospital stay (in days) | 9.4 ± 2.3 | +3.1 | ** |
| Cobb angle before (Cobb°) | 59.7 ± 17.6 | +21.5 | ** |
| Cobb angle afterwards (Cobb°) | 25.0 ± 12.0 | +13.2 | 0.158 |
| Percentage decrease (%) | 57.6 ± 17.4 | −1.5 | 0.737 |
| Variables | Regression Coefficient | Standardized Coefficient | p-Value | 95% CI |
|---|---|---|---|---|
| Total operation time (hours) | 1.01 | 0.586 | <0.001 | 0.683–1.337 |
| Presence of PC | 1.56 | 0.220 | 0.024 | 0.213–2.898 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rüwald, J.M.; Upenieks, J.; Ositis, J.; Pycha, A.; Avidan, Y.; Rüwald, A.L.; Eymael, R.L.; Schildberg, F.A. Pediatric Scoliosis Surgery—A Comprehensive Analysis of Treatment-Specific Variables and Trends in Latvia. Medicina 2020, 56, 201. https://doi.org/10.3390/medicina56040201
Rüwald JM, Upenieks J, Ositis J, Pycha A, Avidan Y, Rüwald AL, Eymael RL, Schildberg FA. Pediatric Scoliosis Surgery—A Comprehensive Analysis of Treatment-Specific Variables and Trends in Latvia. Medicina. 2020; 56(4):201. https://doi.org/10.3390/medicina56040201
Chicago/Turabian StyleRüwald, Julian M., Janis Upenieks, Janis Ositis, Alexander Pycha, Yuval Avidan, Anna L. Rüwald, Robin L. Eymael, and Frank A. Schildberg. 2020. "Pediatric Scoliosis Surgery—A Comprehensive Analysis of Treatment-Specific Variables and Trends in Latvia" Medicina 56, no. 4: 201. https://doi.org/10.3390/medicina56040201