Analysis of Sexual Disorders in Men with Infrarenal Abdominal Aortic Aneurysm Treated by Stent-Graft or Prosthesis Implantation—A Pilot Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
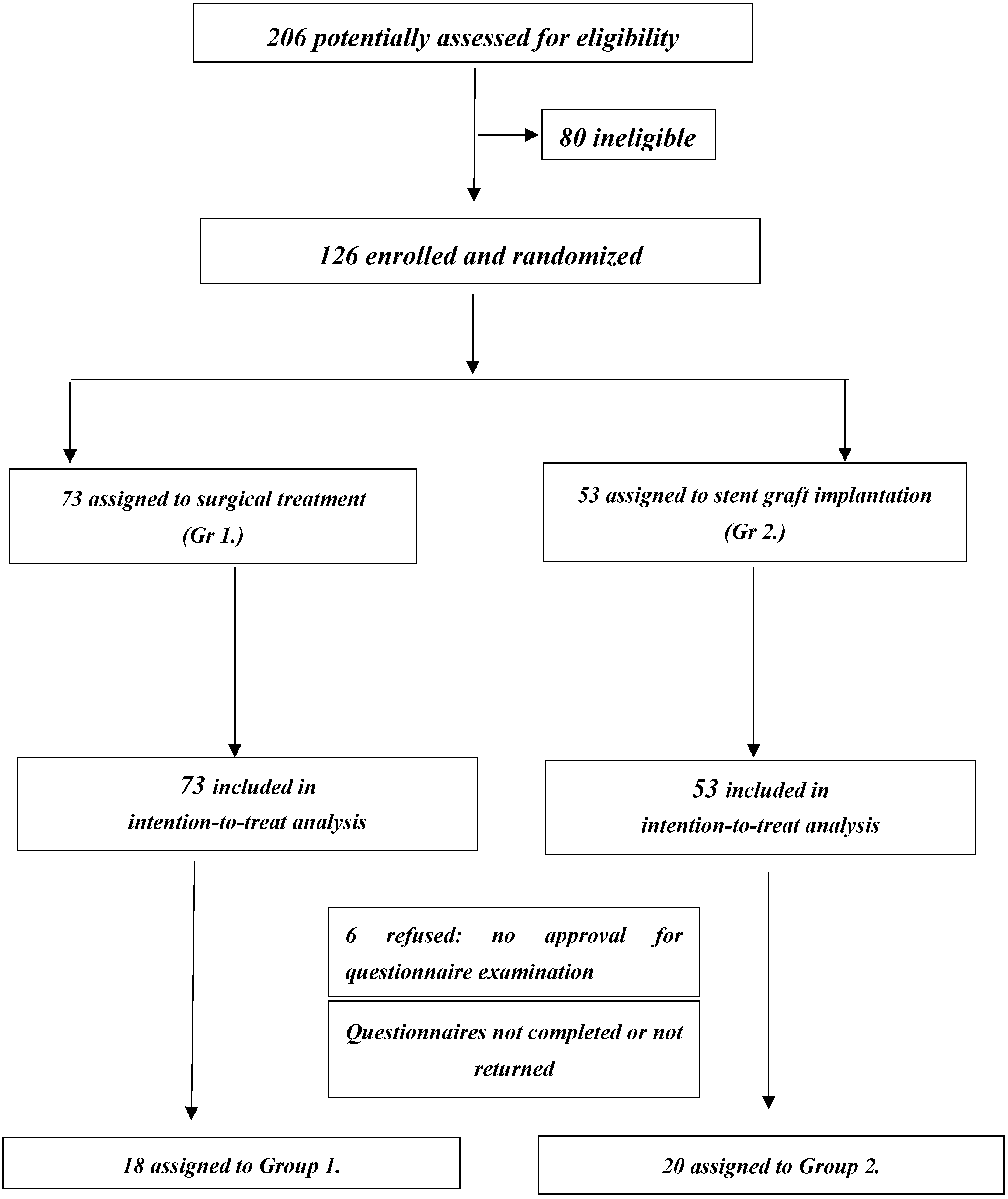
2.1. Studied Population
2.2. Methods
2.3. Statistical Analysis
2.4. Ethical Statement
3. Results
3.1. Analysis of the IIEF Survey
3.2. Assessment of Quality of Life and Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Karkos, C.D.; Wood, A.; Bruce, I.N.; Karkos, P.D.; Baguneid, M.S.; Lambert, M.E. Erectile Dysfunction After Open Versus Angioplasty Aortoiliac Procedures: A Questionnaire Survey. Vasc. Endovasc. Surg. 2004, 38, 157–165. [Google Scholar] [CrossRef]
- Lee, E.S.; Kor, D.J.; Kuskowski, M.A.; Santili, S.A. Incidence of erectile dysfunction after open abdominal aortic aneurysym repair. Ann. Vasc. Surg. 2000, 14, 13–19. [Google Scholar] [CrossRef]
- Miller, T.A. Diagnostic evaluation of erectile dysfunction. Am. Fam. Physician 2000, 61, 95–104. [Google Scholar]
- Pettersson, M.E.; Mattsson, E.; Bergbom, I. Prospective follow-up of sexual function after elective abdominal aortic aneurysms using open and endovascular techniques. J. Vasc. Surg. 2009, 50, 492–499. [Google Scholar] [CrossRef] [Green Version]
- Majd, P.; Ahmad, W.; Luebke, T.; Gawenda, M.; Brunkwall, J. Impairment of erectile function after elective repair of abdominal aortic aneurysm. Vascular 2016, 24, 37–43. [Google Scholar] [CrossRef]
- Michalak, A.; Michalak, K.; Bocian, R.; Okraszewski, J.; Wroński, K. How does change quality of life rating in patients post aneurysm surgery.? Piel Chir Ang. 2009, 3, 93–112. [Google Scholar]
- Veroux, P.; D’Arrigo, G.; Veroux, M.; Giaquinta, A.; Lomeo, A. Sexual Dysfunction after Elective Endovascular or Hand Assisted Laparoscopic Abdominal aortic Repair. Eur. J. Vasc. Endovasc. Surg. 2010, 40, 71–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leriche, R.; Morel, A. The synfrome of thrombotic blteration of the aortic bifurcation. ANN Surg. 1948, 127, 193–206. [Google Scholar] [CrossRef] [PubMed]
- The WHOQOL Group. What quality of life? World Health Organization Quality of Life Assessment. World Health Forum 1995, 41, 1403–1409. [Google Scholar]
- Turska, W.; Sjowron, A. Methodology of quality of life rating. Farm Pol. 2009, 65, 572–580. [Google Scholar]
- Kłak, A.; Mińko, M.; Siwczyńska, D. Questionaire methods of measurement the quality of life. Probl. Hig. Epidemiol. 2012, 93, 632–638. [Google Scholar]
- Rhoden, E.L.; Telöken, C.; Sogari, P.R.; Souto, C.A.V. The use of the simplified International Index of Erectile Function [IIEF–5] as a diagnostic tool study the prevalence of erectile dysfunction. Int. J. Impot. Res. 2002, 14, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. International index of erectile function [IIEF] a multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [Green Version]
- Sznapka, M. Compilation of the Nursing Procedures With Consideration of Quality of Life During Perioperative Period in Patients With Infrarenal Aortic Aneurysm Treated Intervascular and Surgically. Ph.D. Thesis, Medical University of Silesia, Katowice, Poland, 4 July 2017. Available online: https://sum.edu.pl/obrony-prac-doktorskich/6897-obrona-pracy-doktorskiej-wlk-4-07-2017r; (accessed on 27 June 2017).
- Ziaja, D.; Biolik, K.; Sznapka, M.; Domalik, J.; Tkocz, M.; Urbanek, T.; Kuczmik, W.; Ziaja, K. Venous thrombosis. In Guidlines for Diagnostic and Treatment Procedures as Well as Nursing Care; Via Medica: Gdańsk, Poland, 2010; ISBN 978-83-7555-206-5. [Google Scholar]
- Tkocz, M.; Kupajski, M.; Duda, M. The contenporary diagnostics of erectile disfunction. Ann. Acad. Med. Siles. 2007, 61, 71–76. [Google Scholar]
- Daveci, S.; O’Brien, K.; Parker, M.; Guhring, P.; Mulhall, J.P. Can the Internatiolan Index of Erectile Function distinguish between organic and psychogenic erectile function? BIU Int. 2008, 102, 354–356. [Google Scholar]
- Andersson, K.E.; Wagner, G. Physiology of penile erection. Physiol. Rev. 1995, 75, 191–236. [Google Scholar] [CrossRef]
- Shiri, R.; Koskimaki, J.; Hakama, M.; Häkkinen, J.; Tammela, T.L.; Huhtala, H.; Auvinen, A. Prevalence and Severity of Erectile Dysfunction in 50 to 75 Year Old Finnish Men. J. Urol. 2003, 170, 2342–2344. [Google Scholar] [CrossRef]
- Eardley, I.; Gentile, V.; Austoni, E.; Hackett, G.; Lembo, D.; Wang, C.; Beardsworth, A. Efficacy and safety of tadalafil in a Western European population of men with erectile dysfunction. BJU Int. 2004, 93, 563–567. [Google Scholar] [CrossRef]
- Rosen, R.C. Reproductive health problems in ageing men. Lancet 2005, 366, 183–185. [Google Scholar] [CrossRef]
- Lepor, H.; Gregerman, M.; Mostofi, R.; Walsh, C. Precise localization of the anatomic nerves from the pelvic plexusmto the corpoca cavernosa: A detailed anatomical study of the adult male pelvis. J. Urol. 1985, 133, 207–212. [Google Scholar] [CrossRef]
- Strasser, H.; Bartsh, G. Anatomic basis for the interventions of the male pelvis. Urol. A. 2004, 43, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Carmelit, P. Bllod vessels and nerves: Common signals. pathways and diseases. Nat. Rev. Gennet. 2003, 4, 710–720. [Google Scholar] [CrossRef]
- Mulvany, M.L. Small artery remodelling in hypertensions: Causes, consequences and therapeutic implicationsn. Med. Biol. Eng. Comput. 2008, 46, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Popel, A.S.; Johnson, P.C. Microcirculation and hemorheology. Annu. Rev. Fluid Mech. 2005, 37, 43–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McVary, K.T.; Carrier, S.; Wessells, H. Smoking and erectile dysfunction: Evidence based analysis. J. Urol. 2001, 166, 1623–1632. [Google Scholar] [CrossRef]
- Solomon, H.; Man, J.W.; Wierzbicki, A.S.; Jackson, G. Relation to erectile dysfunction to angiographic coronary artery disease. Am. J. Cardiol. 2003, 15, 230–231. [Google Scholar] [CrossRef]
- Nehra, A.; Jolly, N.; Rybak, J. Reviev of erectile dysfunction and cardiovascular risk. Minerva Urol. Nephrol. 2013, 65, 109–115. [Google Scholar]
- Rosen, R.C.; Allen, K.R.; Ni, X.; Arujo, A.B. Minimally clinically important defferences in the erectile function of the International Index of Erectile Function scale. Eur. Urol. 2011, 60, 1010–1016. [Google Scholar] [CrossRef]
- Kloner, R.A.; Henderson, L. Sexual Function in Patients with Chronic Angina Pectoris. Am. J. Cardiol. 2013, 111, 1671–1676. [Google Scholar] [CrossRef]
- Ziaja, D. The Patency of Inferior Mesenteric Artery, Detachment of Thrombus, Extensiveness of Aneursme, Expression of Cytokines and Proteins Compared to Content of Metals and Non–Metals as a Marker of Inflamation of the Infrarental Aortic Aneutysme. Habilitation Thesis, Medical University of Silesia, Katowice, Poland, 2013. [Google Scholar]
- Ledda, A. Cigarette Smoking, Hypertension and Erectile Dysfunction. Curr. Med. Res. Opin. 2000, 16, s13–s16. [Google Scholar] [CrossRef]
- Haete, C.B.; Meston, C.M. Assosiation berween smoking cessation and sexual health in men. BJU Int. 2012, 109, 888–896. [Google Scholar]
- Philip, F.; Shishehbor, M.H. Current State of Endovascular Treatment of Vasculogenic Erectile Dysfunction. Curr. Cardiol. Rep. 2013, 16, 360–363. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Variable | Group 1; N = 18 Mean (SD) | Group 2; N = 20 Mean (SD) | V (X) W % |
|---|---|---|---|
| IIEF 5” = 25 p | (n = 4) 14.5 (3.81) | (n = 3) 14.1 (3.75) | Gr. 1 = 26 Gr. 2 = 26 |
| IIEF ≤ 21 | (n = 14) 19.42 (4.40) | (n = 17) 15.22 (3.88) | Gr. 1 = 22 Gr. 2 = 25 |
| Q 1 | 2.35 (1.38) | 2.85 (0.72) | Gr. 1 = 58 Gr. 2 = 25 |
| Q 2 | 2.6 (1.3) | 2.6 (1.21) | Gr. 1 = 50 Gr. 2 = 48 |
| Q 3 | 2.3 (1.2) | 2.5 (1.12) | Gr. 1 = 50 Gr. 2 = 44 |
| Q 4 | 2.8 (1.4) | 2.8 (1.37) | Gr. 1 = 50 Gr. 2 = 48 |
| Q 5 | 2.95 (1.2) | 3.4 (1.0) | Gr. 1 = 40 Gr.2 = 29 |
| Variable | Group 1; N = 73 | Group 2; N = 53 |
|---|---|---|
| Smoking, n (%) (20–30 daily, 30–40 years) | 72/73 (98.63%) | 50/51 (94.33%) |
| Coffee (per day) | 2–4 | 2–4 |
| Alcohol | Occasionally | Occasionally |
| Claudicatio intermittens < 200 m | 27.4 % | 30.18 % |
| Varices veins | 42.46 % | 64.15 % |
| Pulmonary obturator diseases | 15.06 % | 39.62% |
| Variable | Group 1A; N = 49 * (%) | Group 1B; N = 36 ** (%) | Gr 2; N = 61 *** (%) |
|---|---|---|---|
| Hypertension, (%) | 95.9 | 94.4 | 96.7 |
| CABG | 12.2 | 19.4 | 22.9 |
| MI, n (%) | 12.2 | 5.5 | 24.5 |
| CAD | 18.3 | 33.3 | 52.4 |
| Diabetes, (%) | 18.3 | 11.1 | 16.3 |
| Variable | Surgery | Stent Graft Implantation | p |
|---|---|---|---|
| Patient age, years | 68.5 (Range 53–85) | 68.7 (Range 52–83) | NS |
| Cigarettes, % | 94.4% | 95.0% | NS |
| Coffee, Range | 2–4 | 2–4 | |
| Alcohol | Occasionally | Occasionally | |
| Hypertension, % | 94.4% | 95.0% | NS |
| Diabetes, % | 11.1% | 10.0% | NS |
| CAD, % | 16.6% | 45.0% | p < 0.05 |
| MI, % | 11.1% | 15.0% | NS |
| CABG, % | 11.1% | 20.0% | p < 0.05 |
| Claudicatio intermittens <200 m | 22.2% | 25.0% | NS |
| Varices and pulmonary embolization | 44.4% | 45.0% | NS |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sznapka, M.; Brzęk, A.; Ziaja, D.; Tkocz, M.; Pawlicki, K.; Ziaja, K.; Skrzypulec-Plinta, V.; Chudek, J.; Kuczmik, W. Analysis of Sexual Disorders in Men with Infrarenal Abdominal Aortic Aneurysm Treated by Stent-Graft or Prosthesis Implantation—A Pilot Study. Medicina 2020, 56, 191. https://doi.org/10.3390/medicina56040191
Sznapka M, Brzęk A, Ziaja D, Tkocz M, Pawlicki K, Ziaja K, Skrzypulec-Plinta V, Chudek J, Kuczmik W. Analysis of Sexual Disorders in Men with Infrarenal Abdominal Aortic Aneurysm Treated by Stent-Graft or Prosthesis Implantation—A Pilot Study. Medicina. 2020; 56(4):191. https://doi.org/10.3390/medicina56040191
Chicago/Turabian StyleSznapka, Mariola, Anna Brzęk, Damian Ziaja, Michał Tkocz, Krzysztof Pawlicki, Krzysztof Ziaja, Violetta Skrzypulec-Plinta, Jerzy Chudek, and Wacław Kuczmik. 2020. "Analysis of Sexual Disorders in Men with Infrarenal Abdominal Aortic Aneurysm Treated by Stent-Graft or Prosthesis Implantation—A Pilot Study" Medicina 56, no. 4: 191. https://doi.org/10.3390/medicina56040191