Necrotizing Sialometaplasia and Bulimia: A Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
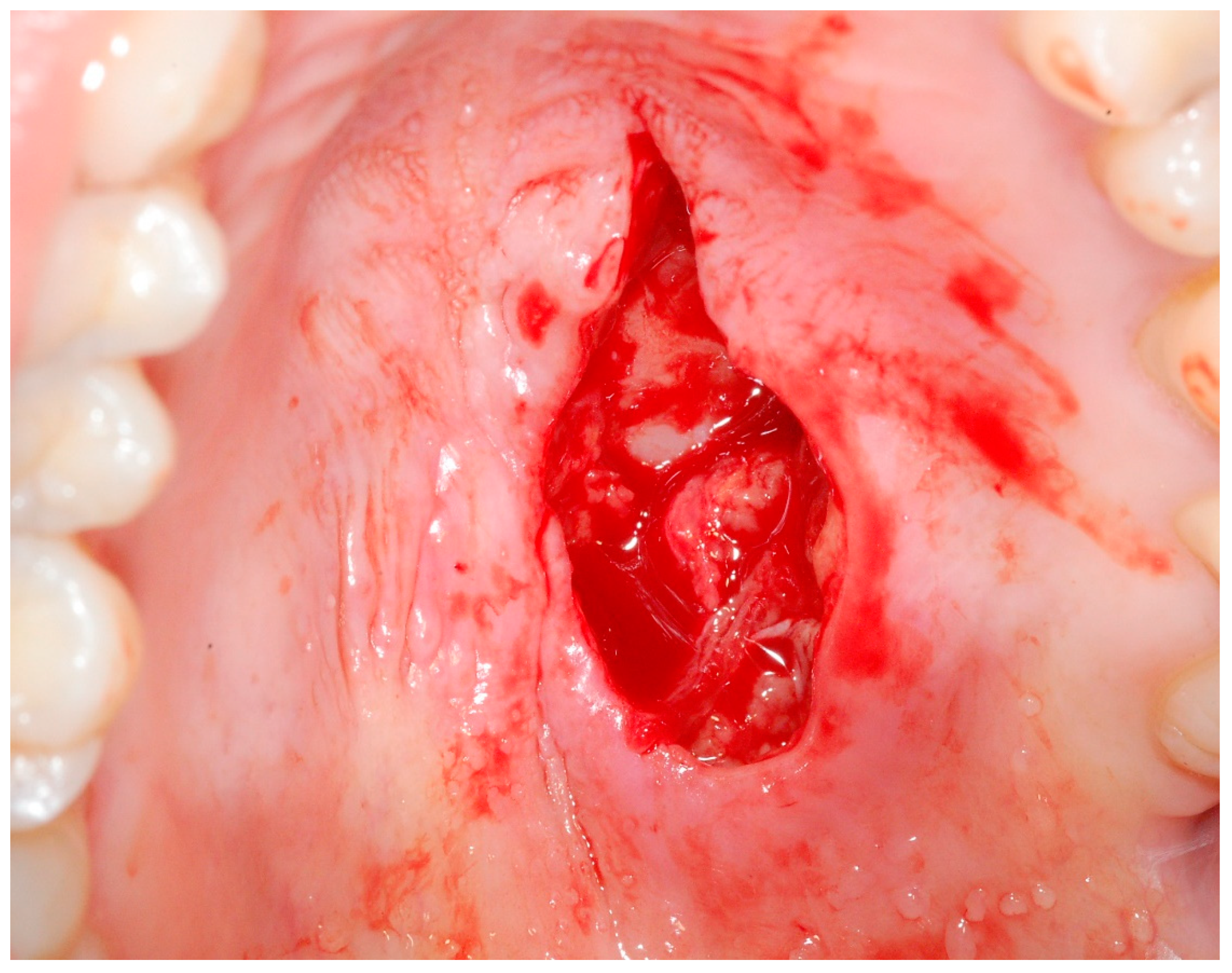
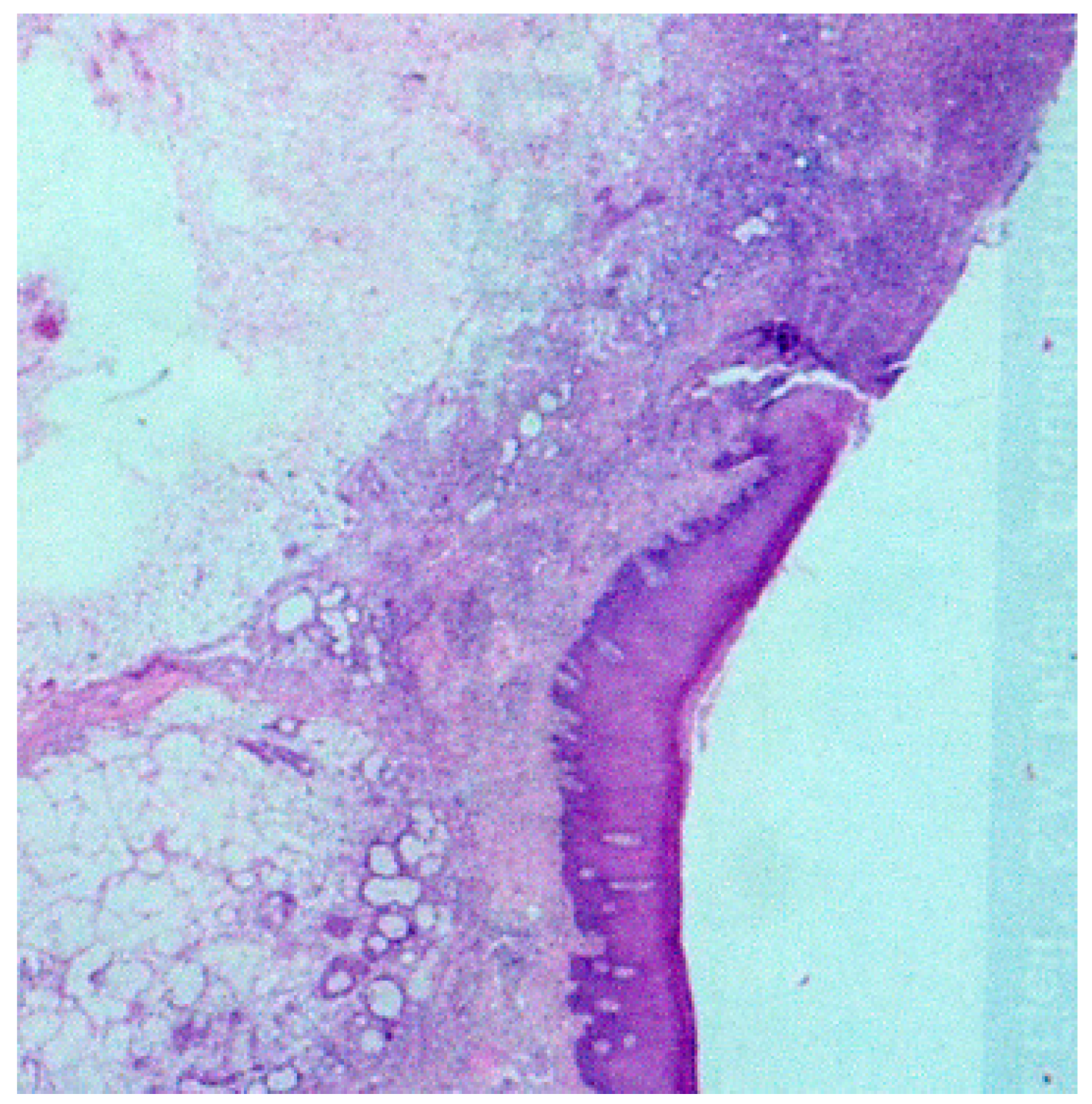
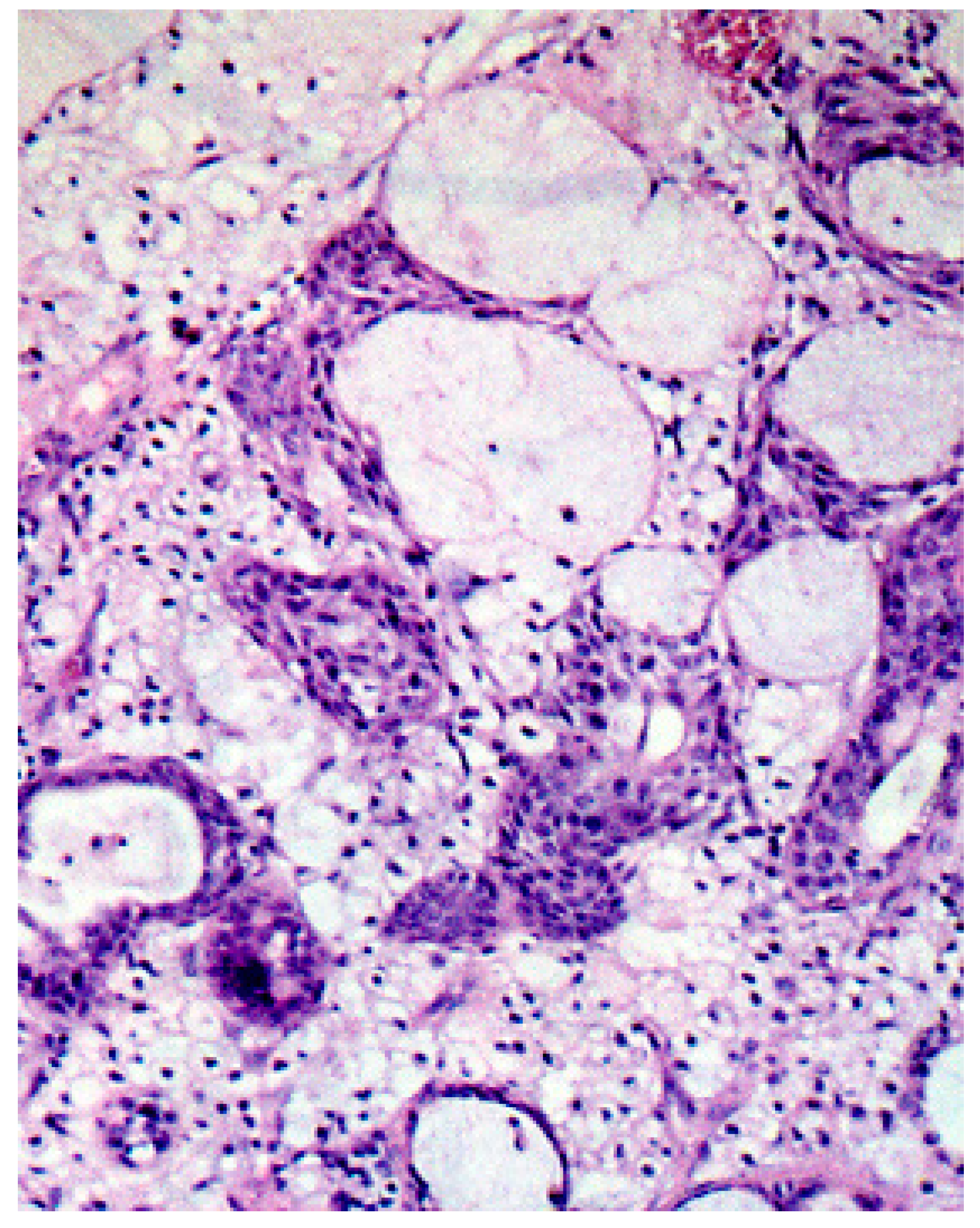
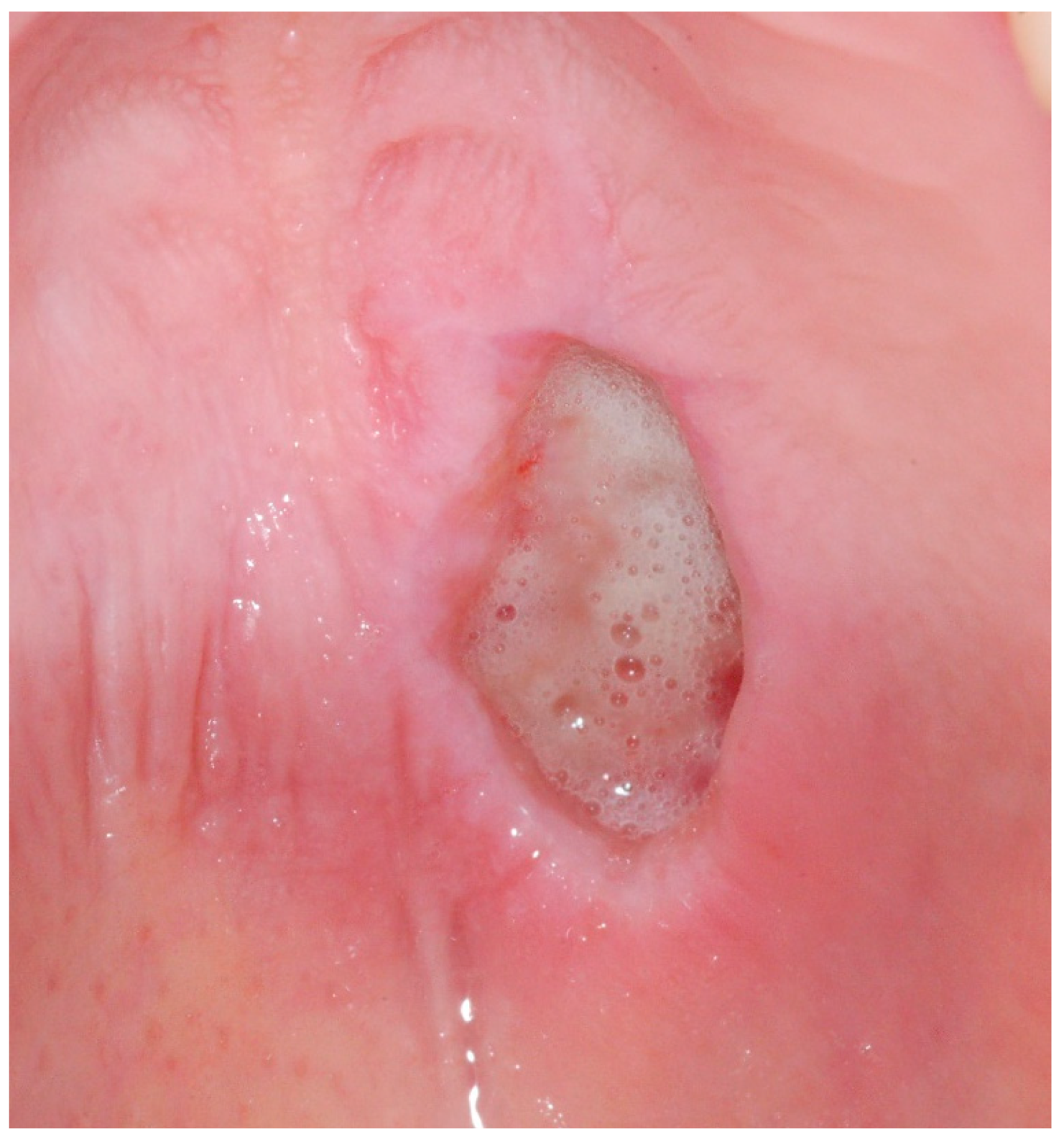
2. Case Report
3. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Penner, C.R.; Thompson, L.D. Necrotizing sialometaplasia. Ear Nose Throat J. 2003, 82, 493–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilowski, Ł.; Wiench, R.; Polakiewicz-Gilowska, A.; Dwornicka, K. Necrotizing sialometaplasia of the palatal mucosa in patient with history of anorexia: Review and case report. Am. J. Otolaryngol. 2014, 35, 400–401. [Google Scholar] [CrossRef] [PubMed]
- Abdalla-Aslan, R.; Frid, H.; Totri, A.; Akrish, S.; Merhav, G.; Rachmiel, A. Necrotizing sialometaplasia of the palate in a young bodybuilder with anabolic androgenic steroids abuse. Quintessence Int. 2020, 20, 2–7. [Google Scholar] [CrossRef]
- Brannon, R.B.; Fowler, C.B.; Hartman, K.S. Necrotizing sialometaplasia. A clinicopathologic study of sixty-nine cases and review of the literature. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 317–325. [Google Scholar] [CrossRef]
- Rye, L.A.; Calhoun, N.R.; Redman, R.S. Necrotizing sialometaplasia in a patient with Buerger’s disease and Raynaud’s phenomenon. Oral Surg. Oral Med. Oral Pathol. 1980, 49, 233–236. [Google Scholar] [CrossRef]
- Keogh, P.V.; O’Regan, E.; Toner, M.; Flint, S. Necrotizing sialometaplasia: An unusual bilateral presentation associated with antecedent anaesthesia and lack of response to intralesional steroids. Case report and review of the literature. Br. Dent. J. 2004, 196, 79–81. [Google Scholar] [CrossRef]
- Flint, S.R. Necrotizing sialometaplasia: An important diagnosis--review of the literature and spectrum of clinical presentation. J. Ir. Dent. Assoc. 2004, 51, 26–28. [Google Scholar]
- Arduino, P.G.; Carrozzo, M.; Pentenero, M.; Bertolusso, G.; Gandolfo, S. Non-neoplastic salivary gland diseases. Minerva Stomatol. 2006, 55, 249–270. [Google Scholar]
- Imai, T.; Michizawa, M. Necrotizing sialometaplasia in a patient with an eating disorder: Palatal ulcer accompanied by dental erosion due to binge-purging. J. Oral Maxillofac. Surg. 2013, 71, 879–885. [Google Scholar] [CrossRef]
- Solomon, L.W.; Merzianu, M.; Sullivan, M.; Rigual, N.R. Necrotizing sialometaplasia associated with bulimia: Case report and literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, e39–e42. [Google Scholar] [CrossRef]
- Daudia, A.; Murty, G.E. First case of full-thickness palatal necrotizing sialometaplasia. J. Laryngol. Otol. 2002, 116, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Imbery, T.A.; Edwards, P.A. Necrotizing sialometaplasia: Literature review and case reports. J. Am. Dent. Assoc. 1996, 127, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Garcia, N.G.; Oliveira, D.T.; Faustino, S.E.; Azevedo, A.L. Necrotizing sialometaplasia of palate: A case report. Case Rep. Pathol. 2012, 2012, 679325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, W.H. Necrotizing sialometaplasia involving the mucous glands of the nasal cavity. Hum. Pathol. 1977, 8, 589–592. [Google Scholar] [CrossRef]
- Merwin, G.E.; Duckert, L.G.; Pollak, K. Necrotizing sialometaplasia of the nasopharynx. Ann. Otol. Rhinol. Laryngol. 1979, 88, 348–351. [Google Scholar] [CrossRef]
- Toftegaard, F.A.; Steinicke, T.; Iversen, L. Necrotizing sialometaplasia: A case report. Acta Derm. Venereol. 2004, 84, 403–404. [Google Scholar]
- Fechner, R.E. Necrotizing sialometaplasia: A source of confusion with carcinoma of the palate. Am. J. Clin. Pathol. 1977, 67, 315–317. [Google Scholar] [CrossRef] [Green Version]
- Zhurakivska, K.; Maiorano, E.; Nocini, R.; Mignogna, M.D.; Favia, G.; Troiano, G.; Arena, C.; Caponio, V.C.A.; Lo Muzio, L. Necrotizing sialometaplasia can hide the presence of salivary gland tumors: A case series. Oral Dis. 2019, 25, 1084–1090. [Google Scholar] [CrossRef]
- Donath, K. Pathohistological findings in infarcted parotid glands (necrotizing sialometaplasia) (author’s transl). Arch. Otorhinolaryngol. 1978, 219, 392–393. [Google Scholar] [CrossRef]
- Suresh, L.; Aguirre, A. Subacute necrotizing sialadenitis: A clinicopathological study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 385–390. [Google Scholar] [CrossRef]
- Femopase, F.L.; Hernández, S.L.; Gendelman, H.; Criscuolo, M.I.; López-de-Blanc, S.A. Necrotizing sialometaplasia: Report of five cases. Med. Oral 2004, 9, 304–308. [Google Scholar]
- Couturier, J.; Lock, J. A review of medication use for children and adolescents with eating disorders. J. Can. Acad. Child Adolesc. Psychiatry 2007, 16, 173–176. [Google Scholar]
- World Health Organization (WHO). International Classification of Disease, Version 11; WHO, Geneva. Available online: https://icd.who.int/browse11/l-m/en (accessed on 25 March 2020).
- Crowther, J.H.; Armey, M.; Luce, K.H.; Dalton, G.R.; Leahey, T. The point prevalence of bulimic disorders from 1990 to 2004. Int. J. Eat. Disord. 2008, 41, 491–497. [Google Scholar] [CrossRef]
- Rikani, A.A.; Choudhry, Z.; Choudhry, A.M.; Ikram, H.; Asghar, M.W.; Kajal, D.; Waheed, A.; Mobassarah, N.J. A critique of the literature on etiology of eating disorders. Ann. Neurosci. 2013, 20, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Lilenfeld, L.R.; Ringham, R.; Kalarchian, M.A.; Marcus, M.D. A family history study of binge-eating disorder. Compr. Psychiatry 2008, 49, 247–254. [Google Scholar] [CrossRef]
- Fenichel, R.M.; Warren, M.P. Anorexia, bulimia, and the athletic triad: Evaluation and management. Curr. Osteoporos. Rep. 2007, 5, 160–164. [Google Scholar] [CrossRef]
- Mehler, P.S.; O’Melia, A.; Brown, C.; Gibson, D.; Hollis, J.; Westmoreland, P. Medical complications of bulimia nervosa. Br. J. Hosp. Med. 2017, 78, 672–677. [Google Scholar] [CrossRef]
- Lourenço, M.; Azevedo, Á.; Brandão, I.; Gomes, P.S. Orofacial manifestations in outpatients with anorexia nervosa and bulimia nervosa focusing on the vomiting behavior. Clin. Oral Investig. 2018, 22, 1915–1922. [Google Scholar] [CrossRef] [Green Version]
- Mandel, L.; Kaynar, A.; DeChiara, S. Necrotizing sialometaplasia in a patient with sickle-cell anemia. J. Oral Maxillofac. Surg. 1991, 49, 757–759. [Google Scholar] [CrossRef]
- Scully, C.; Eveson, J. Sialosis and necrotising sialometaplasia in bulimia; a case report. Int. J. Oral Maxillofac. Surg. 2004, 33, 808–810. [Google Scholar] [CrossRef]
- Boyd, L.D.; Dwyer, J.T.; Papas, A. Nutritional implications of xerostomia and rampant caries caused by serotonin reuptake inhibitors: A case study. Nutr. Rev. 1997, 55, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Deslée, G.; Brichet, A.; Lebuffe, G.; Copin, M.C.; Ramon, P.; Marquette, C.H. Obstructive fibrinous tracheal pseudomembrane. A potentially fatal complication of tracheal intubation. Am. J. Respir. Crit. Care Med. 2000, 162, 1169–1171. [Google Scholar] [CrossRef] [PubMed]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvado, F.; de Araújo Nobre, M.; Gomes, J.; Maia, P. Necrotizing Sialometaplasia and Bulimia: A Case Report. Medicina 2020, 56, 188. https://doi.org/10.3390/medicina56040188
Salvado F, de Araújo Nobre M, Gomes J, Maia P. Necrotizing Sialometaplasia and Bulimia: A Case Report. Medicina. 2020; 56(4):188. https://doi.org/10.3390/medicina56040188
Chicago/Turabian StyleSalvado, Francisco, Miguel de Araújo Nobre, João Gomes, and Paulo Maia. 2020. "Necrotizing Sialometaplasia and Bulimia: A Case Report" Medicina 56, no. 4: 188. https://doi.org/10.3390/medicina56040188