Acute Coronary Syndromes in Chronic Kidney Disease: Clinical and Therapeutic Characteristics

 ,
,  , , , , and
, , , , and
Abstract
:
1. Introduction
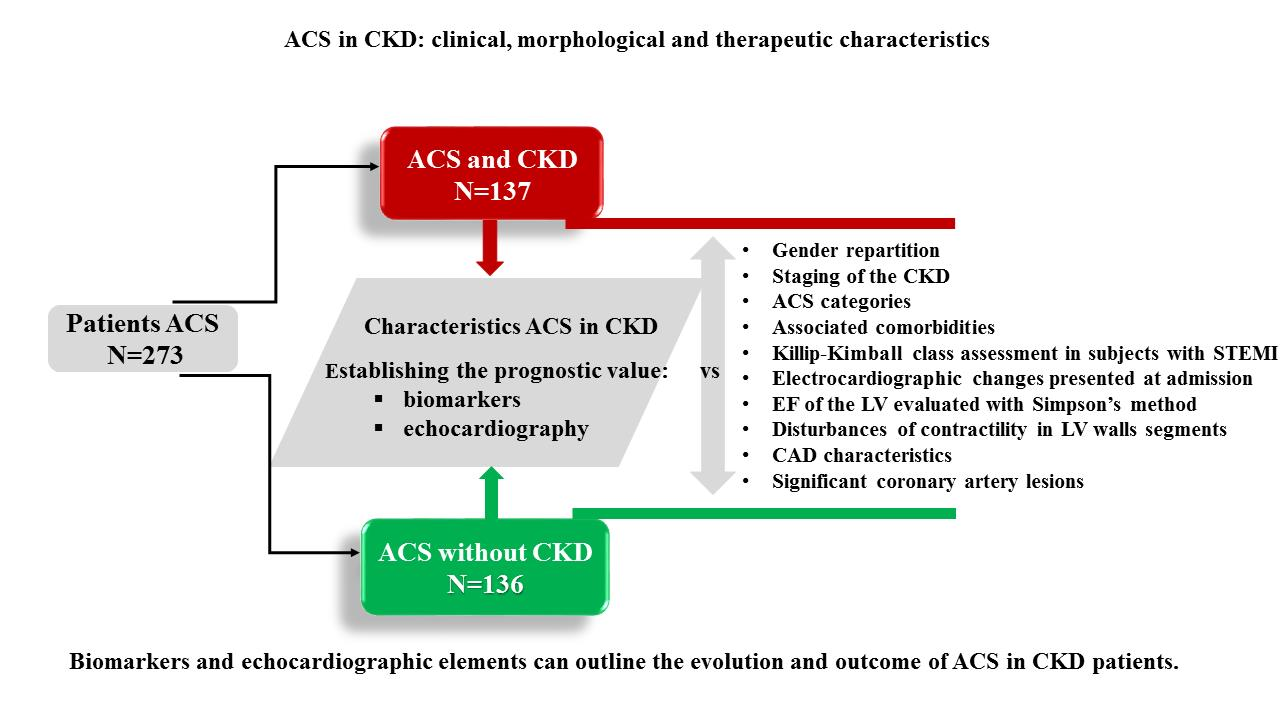
2. Materials and Methods
2.1. Study Design
2.2. Methodology
2.3. Statistical Analysis
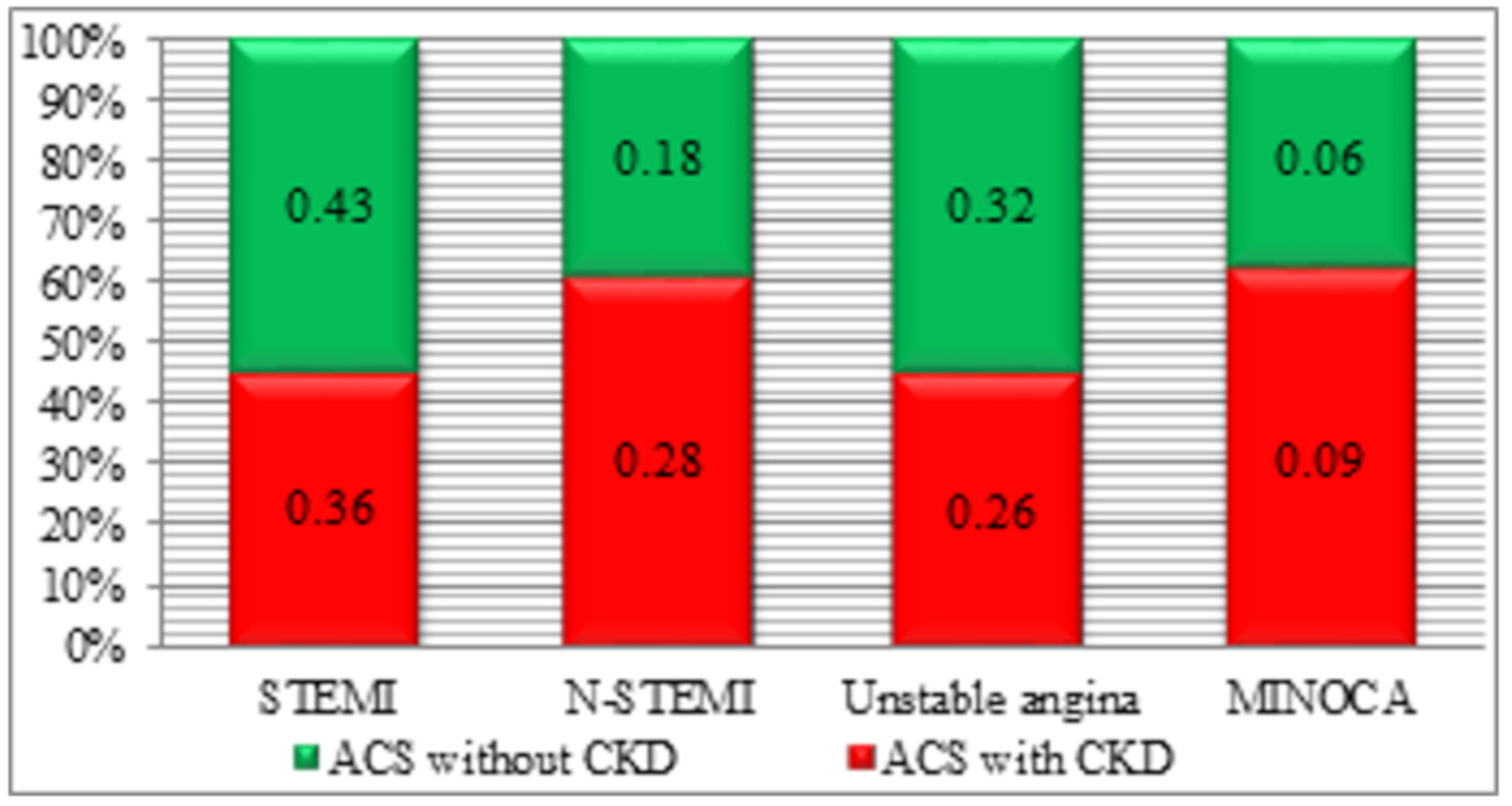
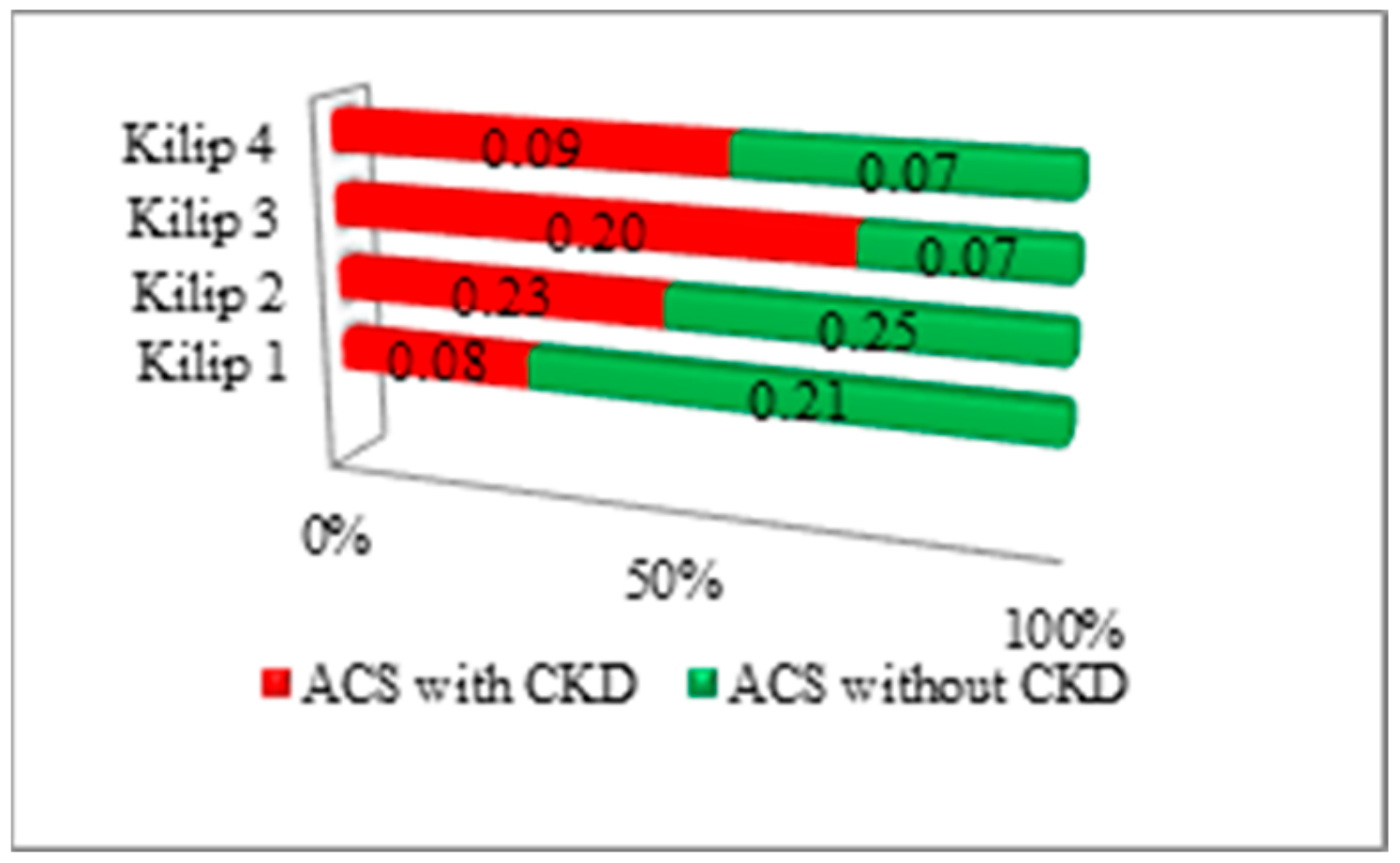
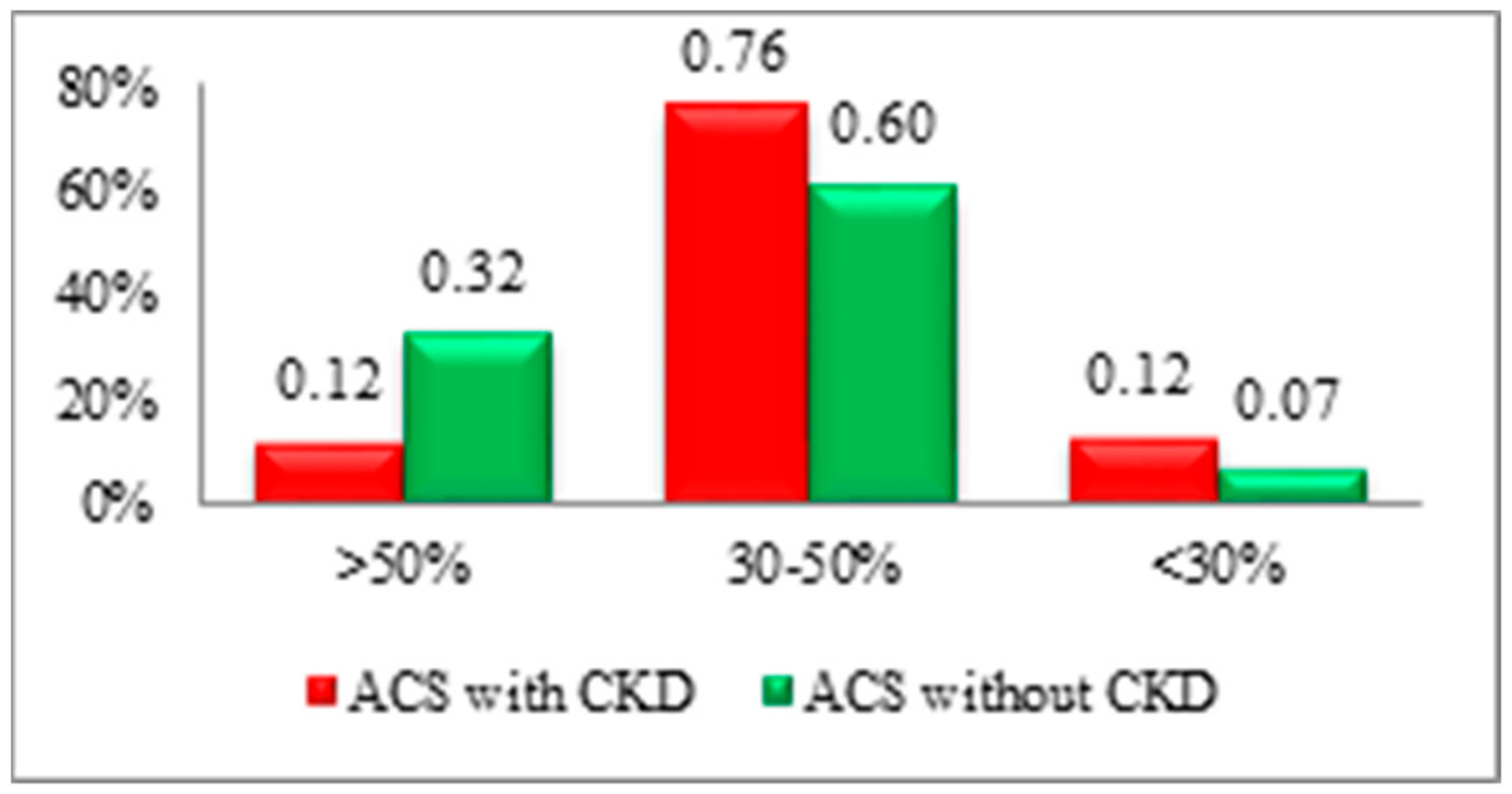
3. Results
- -
- for the association between the GFR, creatinine, urea, uric acid, cTnI, hs-cTnI, NT-proBNP, CRP, and the EF values, a positive significant medium correlation resulted (r = 0.651, R2 = 0.424, p < 0.001);
- -
- for the second case, where the association between GFR, creatinine, urea, uric acid, cTnI, hs-cTnI, NT-proBNP, CRP, and the number of coronary arteries affected in CAD were tested, a positive significant weak correlation was obtained (r = 0.377, R2 = 0.142, p = 0.011).
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yamamoto, S.; Kon, V. Mechanisms for increased cardiovascular disease in chronic kidney dysfunction. Curr. Opin. Nephrol. Hypertens. 2009, 18, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manea, M.; Marcu, D.; Pantea Stoian, A.; Gaman, M.A.; Gaman, A.M.; Socea, B.; Neagu, T.P.; Stanescu, A.M.A.; Bratu, O.G.B.; Diaconu, C.C. Heart failure with preserved ejection fraction and atrial fibrillation: A review. Rev. Chim. 2018, 69, 4180–4184. [Google Scholar] [CrossRef]
- Menon, V.; Gul, A.; Sarnak, M.J. Cardiovascular risk factors in chronic kidney disease. Kidney Int. 2005, 68, 1413–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fellström, B.; Holdaas, H.; Jardine, A.G.; Rose, H.; Schmieder, R.; Wilpshaar, W.; Zannad, F. Effect of rosuvastatin on outcomes in chronic haemodialysis patients: Baseline data from the AURORA study. Kidney Blood Press. Res. 2007, 30, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.C.; Kasiske, B.L. Statins for hemodialysis patients with diabetes? Long-term follow-up endorses the original conclusions of the 4D Study. Kidney Int. 2016, 89, 1189–1191. [Google Scholar] [CrossRef] [Green Version]
- Cai, Q.; Mukku, V.K.; Ahmad, M. Coronary Artery Disease in Patients with Chronic Kidney Disease: A Clinical Update. Curr. Cardiol. Rev. 2013, 9, 331–339. [Google Scholar] [CrossRef] [Green Version]
- Bartos, D.; Diaconu, C.; Badila, E.; Daraban, A.M. Old and new in lipid-lowering therapy: Focus on the emerging drugs. Farmacia 2014, 62, 811–823. [Google Scholar]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2017, 37, 267–315. [Google Scholar]
- Obialo, C.I.; Ofili, E.O.; Norris, K.C. Statins and Cardiovascular Disease Outcomes in Chronic Kidney Disease: Reaffirmation vs. Repudiation. Int. J. Environ. Res. Public Health 2018, 15, 2733. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; The Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Eur. Heart J. 2012, 33, 2551–2567. [Google Scholar] [CrossRef] [Green Version]
- Marenzi, G.; Cabiati, A.; Assanelli, E. Chronic kidney disease in acute coronary syndromes. World J. Nephrol. 2012, 1, 134–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet 1988, 2, 349–360. [Google Scholar]
- The GUSTO Investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N. Engl. J. Med. 1993, 329, 673–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobbach, H.P.; Gibson, C.M.; Giugliano, R.P.; Hundertmark, J.; Schaeffer, C.; Tscherleniak, W.; Schuster, P. The prognostic value of serum creatinine on admission in fibrinolytic-eligible patients with acute myocardial infarction. J. Thromb. Thrombolysis 2003, 16, 167–174. [Google Scholar] [CrossRef]
- Hachinohe, D.; Jeong, D.H.; Saito, S.; Ahmed, K.; Hwang, S.H.; Lee, M.G.; Sim, D.S.; Park, K.H.; Kim, J.H.; Hong, Y.J.; et al. Management of non-ST-segment elevation acute myocardial infarction in patients with chronic kidney disease (from the Korea Acute Myocardial Infarction Registry). Am. J. Cardiol. 2011, 108, 206–213. [Google Scholar] [CrossRef]
- Milojevic, M.; Head, S.J.; Mack, M.J. The impact of chronic kidney disease on outcomes following percutaneous coronary intervention versus coronary artery bypass grafting in patients with complex coronary artery disease: Five-year follow-up of the SYNTAX trial. EurInterv 2018, 14, 102–111. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Levey, A.S.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012. Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Mello, B.H.; Oliveira, G.B.; Ramos, R.F.; Lopes, B.B.; Barros, C.B.; Carvalho Ede, O.; Teixeira, F.B.; Arruda, G.D.; Revelo, M.S.; Piegas, L.S. Validation of the Killip-Kimball classification and late mortality after acute myocardial infarction. Arq. Bras. Cardiol. 2014, 103, 107–117. [Google Scholar] [CrossRef]
- Zhang, R.; Ma, S.; Shanahan, L.; Munroe, J.; Horn, S.; Speedie, S. Discovering and identifying New York heart association classification from electronic health records. BMC Med. Inform. Decis. Mak. 2018, 18, 48. [Google Scholar] [CrossRef] [Green Version]
- Kaul, P.; Naylor, C.D.; Armstrong, P.W.; Mark, D.B.; Theroux, P.; Dagenais, G.R. Assessment of activity status and survival according to the Canadian Cardiovascular Society angina classification. Can. J. Cardiol. 2009, 25, e225–e231. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Lancellotti, P.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaninotto, M.; Mion, M.; Di Serio, F.; Caputo, M.; Ottomano, C.; Plebani, M. PATHFAST™ NT-proBNP (N-terminal-pro B type natriuretic peptide): A multicenter evaluation of a new point-of-care assay. Clin. Chem. Lab. Med. 2010, 48, 1029–1034. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Wetmore, J.B.; Broce, M.; Malas, A.; Almehmi, A. Painless Myocardial Ischemia Is Associated with Mortality in Patients with Chronic Kidney Disease. Nephron Clin. Pract. 2012, 122, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Sosnov, J.; Lessard, D.; Goldberg, R.J.; Yarzebski, J.; Gore, J.M. Differential symptoms of acute myocardial infarction in patients with kidney disease: A community-wide perspective. Am. J. Kidney Dis. 2006, 47, 378–384. [Google Scholar] [CrossRef]
- Ix, J.H.; Shlipak, M.G.; Liu, H.H.; Schiller, N.B.; Whooley, M.A. Association between Renal Insufficiency and Inducible Ischemia in Patients with Coronary Artery Disease: The Heart and Soul Study. J. Am. Soc. Nephrol. 2003, 14, 3233–3238. [Google Scholar] [CrossRef] [Green Version]
- Gaman, M.A.; Dobrica, E.C.; Pascu, E.G.; Cozma, M.A.; Epingeac, M.E.; Gaman, A.M.; Pantea Stoian, A.; Bratu, O.G.; Diaconu, C.C. Cardiometabolic risk factors for atrial fibrillation in type 2 diabetes mellitus: Focus on hypertension, metabolic syndrome and obesity. J. Mind Med. Sci. 2019, 6, 157–161. [Google Scholar] [CrossRef]
- Laslo, C.; Pantea Stoian, A.; Socea, B.; Paduraru, D.; Bodean, O.; Socea, L.; Neagu, T.P.; Stanescu, A.M.A.; Marcu, D.; Diaconu, C. New oral anticoagulants and their reversal agents. J. Mind Med. Sci. 2018, 5, 195–201. [Google Scholar] [CrossRef]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Santopinto, J.J.; Fox, K.A.; Goldberg, R.J.; Budaj, A.; Piñero, G.; Avezum, A.; Gulba, D.; Esteban, J.; Gore, J.M.; Johnson, J.; et al. GRACE Investigators. Creatinine clearance and adverse hospital outcomes in patients with acute coronary syndromes: Findings from the global registry of acute coronary events (GRACE). Heart 2003, 89, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Shroff, G.R.; Frederick, P.D.; Herzog, C.A. Renal failure and acute myocardial infarction: Clinical characteristics in patients with advanced chronic kidney disease, on dialysis, and without chronic kidney disease. A collaborative project of the United States Renal Data System/National Institutes of Health and the National Registry of Myocardial Infarction. Am. Heart J. 2012, 163, 399–406. [Google Scholar] [PubMed] [Green Version]
- Naito, K.; Anzai, T.; Yoshikawa, T.; Anzai, A.; Kaneko, H.; Kohno, T.; Takahashi, T.; Kawamura, A.; Ogawa, S. Impact of Chronic Kidney Disease on Postinfarction Inflammation, Oxidative Stress, and Left Ventricular Remodeling. J. Card. Fail. 2008, 14, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Herzog, C.A.; Littrell, K.; Arko, C.; Blaney, M. Clinical characteristics of dialysis patients with acute myocardial infarction in the United States: A collaborative project of the United States Renal Data System and the National Registry of Myocardial Infarction. Circulation 2007, 116, 1465–1472. [Google Scholar] [CrossRef] [Green Version]
- Dubin, R.F.; Li, Y.; He, J.; Jaar, B.G.; Kallem, R.; Lash, J.P.; Makos, G.; Rosas, S.E.; Soliman, E.Z.; Townsend, R.R.; et al. CRIC Study Investigators. Predictors of high sensitivity cardiac troponin T in chronic kidney disease patients: A cross-sectional study in the chronic renal insufficiency cohort (CRIC). BMC Nephrol. 2013, 14, 229. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.J.; Yao, F.J.; Liu, L.J.; Tang, K.; Lin, X.X.; Li, W.J.; Zhang, J.; Wu, S.H. B-type natriuretic peptide and prognosis of end-stage renal disease: A meta-analysis. PLoS ONE 2013, 8, e79302. [Google Scholar] [CrossRef] [Green Version]
- Stoicescu, M.; Csepento, C.; Mutiu, G.; Bungau, S. The role of increased plasmatic renin level in the pathogenesis of arterial hypertension in young adults. Rom. J. Morphol. Embriol. 2011, 52, 419–423. [Google Scholar]
- Popa, A.R.; Mihai Vesa, C.; Uivarosan, D.; Jurca, C.M.; Isvoranu, G.; Socea, B.; Maria, A.; Stanescu, A.; Iancu, A.; Scarneciu, I.; et al. Cross sectional study regarding the association between sweetened beverages intake, fast-food products, body mass index, fasting blood glucose and blood pressure in the young adults from North-western Romania. Rev. Chim. 2019, 70, 156–160. [Google Scholar] [CrossRef]
- Popa, A.R.; Bungau, S.; Vesa, C.M.; Bondar, A.C.; Pantis, C.; Maghiar, O.; Dimulescu (Nica), I.A.; Nistor-Cseppento, D.C.; Rus, M. Evaluating the efficacy of the treatment with benfotiamine and alpha-lipoic acid in distal symmetric painful diabetic polyneuropathy. Rev. Chim. 2019, 70, 3108–3114. [Google Scholar] [CrossRef]
- Chan, W.; Ivanov, J.; Ko, D.; Fremes, S.; Rao, V.; Jolly, S.; Cantor, W.J.; Lavi, S.; Overgaard, C.B.; Ruel, M.; et al. Clinical outcomes of treatment by percutaneous coronary intervention versus coronary artery bypass graft surgery in patients with chronic kidney disease undergoing index revascularization in Ontario. Circ. Cardiovasc. Interv. 2015, 8, e001973. [Google Scholar] [CrossRef] [Green Version]
- Bangalore, S.; Guo, Y.; Samadashvili, Z.; Blecker, S.; Xu, J.; Hannan, E.L. Revascularization in patients with multivessel coronary artery disease and chronic kidney disease: Everolimus-eluting stents versus coronary artery bypass graft surgery. J. Am. Coll. Cardiol. 2015, 66, 1209–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonelli, M.; Isles, C.; Craven, T.; Tonkin, A.; Pfeffer, M.A.; Shepherd, J.; Sacks, F.M.; Furberg, C.; Cobbe, S.M.; Simes, J.; et al. Effect of pravastatin on rate of kidney function loss in people with or at risk for coronary disease. Circulation 2005, 112, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szummer, K.; Lundman, P.; Jacobson, S.H.; Schön, S.; Lindbäck, J.; Stenestrand, U.; Wallentin, L.; Jernberg, T.; SWEDEHEART. Influence of renal function on the effects of early revascularization in non-ST-segment elevation myocardial infarction: Data from the Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART). Circulation 2009, 120, 851–858. [Google Scholar] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | CKD | GFR (mL/min/1.73 m2) |
|---|---|---|
| 1 | Normal kidney function | ≥90 |
| 2 | Mild loss of kidney function | 60–89 |
| 3 | Moderate loss of kidney function | 30–59 |
| 4 | Severe loss of kidney function | 15–29 |
| 5 | Chronic dialysis treatment | ≤15 |
| Class | The Severity of Shortness of Breath |
|---|---|
| I | No shortness of breath when performing ordinary activities |
| II | Slight limitations of activities due to the shortness of breath occurrence |
| III | Dyspnoea in most of the ordinary activities with marked limitation of the physical activities |
| IV | Shortness of breath at rest and inability to carry physical activities without symptoms occurrence |
| Characteristics | ACS with CKD (n = 137) | ACS without CKD (n = 136) | p * | ||
|---|---|---|---|---|---|
| Gender | No. | % | No. | % | 0.76 |
| Men | 93 | 67.88 | 90 | 66.18 | |
| Women | 44 | 32.12 | 46 | 33.82 | |
| Age | |||||
| Mean age | 68.62 ± 9.94 | 64.19 ± 10.68 | <0.01 | ||
| 95% confidence level | (48.74; 88.5) | (42.83; 85.55) | |||
| GFR | Patients | |
|---|---|---|
| No. | % | |
| Stage 3 | 89 | 64.96 |
| Stage 4 | 32 | 23.36 |
| Stage 5 | 16 | 11.68 |
| Comorbidities/Symptoms at Presentation | ACS with CKD | ACS without CKD | p * | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Chronic coronary syndrome | 62 | 45.26 | 35 | 25.74 | <0.01 |
| Stable angina | 54 | 39.42 | 35 | 25.74 | <0.01 |
| Canadian Cardiovascular Society grading of angina pectoris | |||||
| Degree I | 8 | 5.84 | 6 | 4.41 | 0.59 |
| Degree II | 29 | 21.17 | 23 | 16.91 | 0.37 |
| Degree III | 17 | 12.41 | 6 | 4.41 | 0.01 |
| Previous heart failure | 57 | 41.61 | 27 | 19.85 | <0.01 |
| NYHA II | 32 | 23.36 | 15 | 11.03 | <0.01 |
| NYHA III | 25 | 18.25 | 12 | 8.82 | 0.02 |
| Sequelae of myocardial infarction | 30 | 21.90 | 15 | 11.03 | 0.01 |
| Anterior territory | 15 | 10.95 | 11 | 8.09 | 0.42 |
| Inferior territory | 14 | 10.22 | 3 | 2.21 | <0.01 |
| Lateral territory | 0 | 0.00 | 1 | 0.74 | 0.31 |
| Anterior and inferior territories | 1 | 0.73 | 0 | 0.00 | 0.31 |
| Peripheral artery disease | 24 | 17.52 | 16 | 11.76 | 0.17 |
| Previous ischemic stroke | 25 | 18.25 | 2 | 1.47 | <0.01 |
| Diabetes mellitus | 78 | 56.93 | 48 | 35.29 | <0.01 |
| Thoracic pain at admission | 78 | 56.93 | 118 | 86.76 | <0.01 |
| Dyspnoea at admission | 57 | 41.61 | 18 | 13.24 | <0.01 |
| Syncope at admission | 2 | 1.46 | 0 | 0.00 | 0.16 |
| Cardiogenic shock (%) | 18 | 13.14 | 9 | 6.62 | 0.07 |
| ECG at Admission | ACS with CKD | ACS without CKD | p * | ||
|---|---|---|---|---|---|
| Patients | |||||
| No. | % | No. | % | ||
| ST-segment elevation | 51 | 37.23 | 55 | 40.44 | 0.58 |
| ST-segment depression | 25 | 18.25 | 23 | 16.91 | 0.77 |
| QS waves | 2 | 1.46 | 13 | 9.56 | <0.01 |
| T negative waves | 23 | 16.79 | 20 | 14.71 | 0.63 |
| Left bundle branch block | 18 | 13.14 | 8 | 5.88 | 0.04 |
| Right bundle brunch block | 7 | 5.11 | 5 | 3.68 | 0.56 |
| Left ventricle hypertrophy | 5 | 3.65 | 1 | 0.74 | 0.1 |
| Ventricular paced rhythm | 1 | 0.73 | 1 | 0.74 | 0.99 |
| Complete atrioventricular block | 1 | 0.73 | 0 | 0.00 | 0.31 |
| No ECG changes | 4 | 2.92 | 10 | 7.35 | 0.09 |
| Characteristics | ACS/CKD | ACS | p * | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Single-vessel CAD | 15 | 10.95 | 40 | 29.41 | <0.01 |
| Double-vessel CAD | 37 | 27.01 | 44 | 32.35 | 0.33 |
| Three-vessel CAD | 37 | 27.01 | 31 | 22.79 | 0.42 |
| LMCA | 20 | 14.60 | 12 | 8.82 | 0.13 |
| MINOCA | 12 | 8.76 | 8 | 5.88 | 0.36 |
| Patients without coronary angioplasty | 16 | 11.68 | 1 | 0.74 | <0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moisi, M.I.; Rus, M.; Bungau, S.; Zaha, D.C.; Uivarosan, D.; Fratila, O.; Tit, D.M.; Endres, L.; Nistor-Cseppento, D.C.; Popescu, M.I. Acute Coronary Syndromes in Chronic Kidney Disease: Clinical and Therapeutic Characteristics. Medicina 2020, 56, 118. https://doi.org/10.3390/medicina56030118
Moisi MI, Rus M, Bungau S, Zaha DC, Uivarosan D, Fratila O, Tit DM, Endres L, Nistor-Cseppento DC, Popescu MI. Acute Coronary Syndromes in Chronic Kidney Disease: Clinical and Therapeutic Characteristics. Medicina. 2020; 56(3):118. https://doi.org/10.3390/medicina56030118
Chicago/Turabian StyleMoisi, Mădălina Ioana, Marius Rus, Simona Bungau, Dana Carmen Zaha, Diana Uivarosan, Ovidiu Fratila, Delia Mirela Tit, Laura Endres, Delia Carmen Nistor-Cseppento, and Mircea Ioachim Popescu. 2020. "Acute Coronary Syndromes in Chronic Kidney Disease: Clinical and Therapeutic Characteristics" Medicina 56, no. 3: 118. https://doi.org/10.3390/medicina56030118