Real-Time Remote Tele-Mentored Echocardiography: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
3. Results
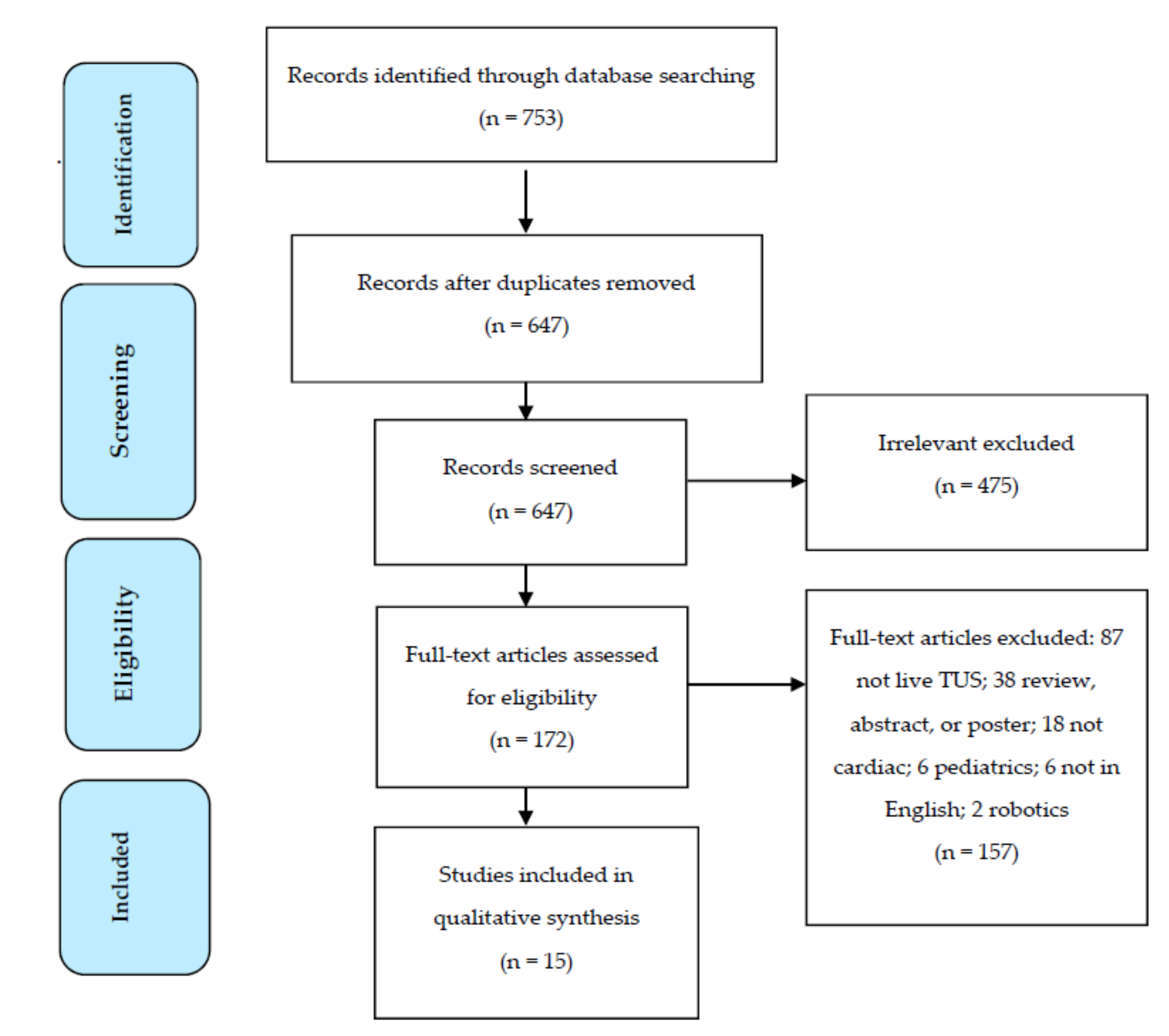
3.1. Studies Selected
3.2. Characteristics of Studies
4. Discussion
4.1. An RTMUS Echo Foundation
- An ultrasound operator at bedside who can perform images;
- An ultrasound;
- A technological platform that can provide active communication between the sonographer and ultrasound expert with simultaneous transmission of ultrasound images and probe location on the patient;
- An expert ultrasound consultant for interpretation.
4.2. RTMUS Echo Training of Novice Users
4.3. RTMUS Technology
4.4. RTMUS Interpretation of Images
4.5. RTMUS Technological Considerations
4.6. RTMUS Echo Use in SARS-CoV-2 and Other High Isolation Areas
4.7. Future Direction and Research of RTMUS Echo
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- ((((“Telemedicine/utilization”[MeSH]) OR “Remote Consultation”[MeSH]) OR “Teleradiology”[MeSH] OR telemedicine[tiab])) AND (“echocardiography/utilization”[MeSH] OR echocardiography[tiab])
- ((((“Telemedicine/utilization”[MeSH]) OR “Remote Consultation”[MeSH]) OR “Teleradiology”[MeSH] OR telemedicine[tiab])) AND (“Ultrasonography/utilization”[MeSH] OR ultrasound[tiab])
- (‘echocardiography’/exp AND ‘telemedicine’/exp).
References
- Cecconi, M.; De Backer, D. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef]
- Labovitz, A.J.; Noble, V.E. Focused Cardiac Ultrasound in the Emergent Setting: A Consensus Statement of the American Society of Echocardiography and American College of Emergency Physicians. J. Am. Soc. Echocardiogr. 2010, 23, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R.; Patel, A.R. Cardiac Ultrasound in the Intensive Care Unit: A Review. Cureus 2019, 11, e4612. [Google Scholar] [CrossRef] [Green Version]
- Britton, N.; Miller, M.A. Tele-Ultrasound in Resource-Limited Settings: A Systematic Review. Front. Public Health 2019, 7, 244. [Google Scholar] [CrossRef] [Green Version]
- Ferioli, M.; Cisternino, C. Protecting healthcare workers from SARS-CoV-2 infection: Practical indications. Eur. Respir. Rev. 2020, 29, 155. [Google Scholar] [CrossRef]
- Salerno, A.; Tupchong, K. Point-of-Care Teleultrasound: A Systematic Review. Telemed. J. E Health 2020, 26. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Boniface, K.S.; Shokoohi, H. Tele-ultrasound and paramedics: Real-time remote physician guidance of the Focused Assessment wWith Sonography for Trauma examination. Am. J. Emerg. Med. 2011, 29, 477–481. [Google Scholar] [CrossRef]
- Russell, P.M.; Mallin, M. First “glass” education: Telementored cardiac ultrasonography using Google Glass- a pilot study. Acad. Emerg. Med. 2014, 21, 1297–1299. [Google Scholar] [CrossRef] [Green Version]
- Robertson, T.E.; Levine, A.R. Remote tele-mentored ultrasound for non-physician learners using FaceTime: A feasibility study in a low-income country. J. Crit. Care 2017, 40, 145–148. [Google Scholar] [CrossRef]
- Ramsingh, D.; Ma, M. Feasibility Evaluation of Commercially Available Video Conferencing Devices to Technically Direct Untrained Nonmedical Personnel to Perform a Rapid Trauma Ultrasound Examination. Diagnostics 2019, 9, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivieri, P.P.; Verceles, A.C. A Pilot Study of Ultrasonography-Naïve Operators’ Ability to Use Tele-Ultrasonography to Assess the Heart and Lung. J. Intensive Care Med. 2020, 35, 672–678. [Google Scholar] [CrossRef]
- Afset, J.E.; Lunde, P. Accuracy of routine echocardiographic measurements made by an inexperienced examiner through tele-instruction. J. Telemed. Telecare 1996, 2, 148–154. [Google Scholar] [CrossRef]
- Becker, C.; Fusaro, M. Tele-Ultrasound to Guide Management of a Patient with Circulatory Shock. Am. J. Med. 2017, 130, e205–e206. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.A.; Shemenski, R. Real-time tele-echocardiography: Diagnosis and management of a pericardial effusion secondary to pericarditis at an Antarctic research station. Telemed J. E Health 2012, 18, 521–524. [Google Scholar] [CrossRef]
- Epstein, D.; Petersiel, N. Pocket-size point-of-care ultrasound in rural Uganda—A unique opportunity “to see”, where no imaging facilities are available. Travel Med. Infect. Dis. 2018, 23, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Douglas, T.M.; Levine, A.R. Brief training increases nurses’ comfort using tele-ultrasound: A feasibility study. Intensive Crit. Care Nurs. 2019, 51, 45–49. [Google Scholar] [CrossRef]
- Levine, A.R.; Buchner, J.A. Ultrasound images transmitted via FaceTime are non-inferior to images on the ultrasound machine. J. Crit. Care 2016, 33, 51–55. [Google Scholar] [CrossRef]
- Kim, C.; Hur, J. Can an Offsite Expert Remotely Evaluate the Visual Estimation of Ejection Fraction via a Social Network Video Call? J. Digit. Imaging 2017, 30, 718–725. [Google Scholar] [CrossRef]
- Miyashita, T.; Takizawa, M. Telemedicine of the heart: Real-time telescreening of echocardiography using satellite telecommunication. Circ. J. 2003, 67, 562–564. [Google Scholar] [CrossRef] [Green Version]
- Huffer, L.L.; Bauch, T.D. Feasibility of remote echocardiography with satellite transmission and real-time interpretation to support medical activities in the austere medical environment. J. Am. Soc. Echocardiogr. 2004, 17, 670–674. [Google Scholar] [CrossRef]
- Jensen, S.H.; Weile, J. Remote real-time supervision via tele-ultrasound in focused cardiac ultrasound: A single-blinded cluster randomized controlled trial. Acta Anaesthesiol. Scand. 2019, 63, 403–409. [Google Scholar] [CrossRef]
- Levine, A.R.; Robertson, T.E. Tele-Medicine and Point-of-Care Ultrasound: A New Paradigm for Resource-Constrained Settings. Chest 2016, 149, 1580–1581. [Google Scholar] [CrossRef]
- Paulus, Y.M.; Thompson, N.P. Inexpensive, realtime tele-ultrasound using a commercial, web-based video streaming device. J. Telemed. Telecare 2012, 18, 85–188. [Google Scholar] [CrossRef]
- Jajodia, A.; Ebner, L. Imaging in corona virus disease 2019 (COVID-19)-A Scoping review. Eur. J. Radiol. 2020, 7, 100237. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J. The Role of Chest Imaging in Patient Management During the COVID-19 Pandemic: A Multinational Consensus Statement fFrom the Fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef]
- American College of Radiology. Available online: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection (accessed on 1 August 2020).
- Szekely, Y.; Lichter, Y. Spectrum of Cardiac Manifestation in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID-19: A Simple, Quantitative, Reproducible Method. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Article | Study Design and Setting | Objective | Number and Experience Level of Learners/Sonographers | Number of Patients and Patient Population | Cardiac US Views and Measurements Obtained | Outcome Measures | Results |
|---|---|---|---|---|---|---|---|
| Afset et al. (1996) [13] | Feasibility study, community hospital, Norway | Evaluate reproducibility and accuracy of RTMUS echo measurements | One novice physician | 38 patients with known or suspected heart disease | PSL, A4C; EPSS, Doppler to estimate MR, AR, TR/pulmonic flow | Learner’s measurements compared to expert US examination | No difference between expert and RTMUS assessments of mean M-mode or Doppler variables |
| Miyashita et al. (2003) [20] | Feasibility study, mobile health vehicle, Japan | Evaluate ability to effectively transmit US images via satellite | Echocardiography specialist | 57 patients | Not specified | Image quality and acquisition time compared to US machine images | Average exam time 8.4 min (range, 6.1–10.1). Quality nearly identical to original |
| Huffer et al. (2004) [21] | Feasibility study, simulated mass casualty, USA | Determine feasibility and diagnostic accuracy of RTMUS during mass casualty | Trained sonographers | 10 individuals with known structural cardiac disease and 2 healthy controls | LVEF, RV Strain, RWM, LV size, AV/MV pathology | Technical quality and diagnostic accuracy | Overall average of 95% concordance between two sets of images |
| Boniface et al. (2011) [8] | Feasibility study, simulated pre-hospital setting, USA | Assess ability of paramedics to obtain adequate views using RTMUS | 51 novice paramedics | Healthy volunteer | Subx; PSL if inadequate subx | Adequacy of views (yes/no) | Success rate of 100% to obtain “adequate” views |
| Otto et al. (2012) [15] | Case report, community hospital, Antarctica | Demonstrate ability of RTMUS to serve as important diagnostic tool in remote environments | One physician with “basic” CU skills | One patient | Subx, PSL, PSS, A4C | No formal analysis | Diagnosis of pericarditis; RTMUS prevented unnecessary transcontinental medical evacuation |
| Russell et al. (2014) [9] | Prospective, randomized, single-blinded, academic setting, USA | Compare ability to obtain PSLA US views for (1) no, (2) remote, and (3) in-person mentoring | 18 novice medical students | 75 kg live model | PSL; EPSS | Adequacy and quality of EPSS | No significant difference |
| Levine et al. (2016) [18] | Feasibility study, academic setting, USA | Determine ability of telemedicine ICU physicians to mentor remote sonographers to obtain US images | 11 novice non-physician health care providers | One healthy volunteer | Subx | Compare image quality and ability to make clinical decisions from US machine or RTMUS | Of RTMUS images, 69/77 (90%) were high quality and 74/77 (96%) permitted clinical decision making |
| Becker et al. (2017) [14] | Case report, tertiary hospital ICU, USA | Evaluate fluid responsiveness | One provider with CU training | One patient | PSL, A4C, IVC | RTMUS exam showed signs of distributive and hypovolemic shock | Patient given fluid with increase in MAP and vasopressors stopped |
| Kim et al. (2017) [19] | Feasibility study, tertiary hospital ICU, Korea | Determine ability of remote expert to evaluate EF with RTMUS using social network video call | 60 novice sonographers | 60 patients | PSL, PSS, A4C; EPSS, EF | Compare cardiologist-performed Simpson’s method vs. RTMUS EF and EPSS evaluation | Statistically excellent agreement between two measurements of EF |
| Robertson et al. (2017) [10] | Feasibility study, community hospital, Haiti | Determine ability of remote tele-intensivist to mentor providers to obtain US images | 9 novice non-physician healthcare workers | One healthy volunteer | Subx | Comfort of making clinical decisions based on images, image quality | Tele-intensivist could make clinical decisions with 56/63 (89%) images, of which 57/63 (90%) were high quality |
| Epstein et al. (2018) [16] | Rural hospital, Uganda | Evaluate ability of physician to detect major US findings after basic training | One physician underwent 5-day training | 7 echo studies, not specified # of real-time | Not specified | Assess image utility to make clinical decisions | RTMUS via smartphone for echo image feasible, reducing need for complete echo studies |
| Douglas et al. (2019) [17] | Feasibility study, pilot cohort and clinical cohort, community ICU, USA | Assess US training (1) effect on non-physician comfort performing TUS and (2) feasibility to improve participant comfort | Pilot cohort: 11 non-physician providersClinical cohort: 5 ICU nurses | Pilot cohort: 1 healthy volunteerClinical cohort: ICU inpatients over 6 weeks | Pilot cohort: SubxClinical cohort: PSL, PSS, Subx | Participant survey of experience and comfort of performing RTMUS | After training, all participants had positive experience and comfortable using RTMUS |
| Jensen et al. (2019) [22] | Single-blinded cluster randomized control trial, regional ED, Denmark | Investigate image quality of cine-loop recordings of RTMUS vs. non-supervised physician’s vs. experts | 10 physicians with prior CU training | 44 patients | Subx, PSL, PSS, A4C | Two blinded observers graded cine-loops recorded from all scans | RTMUS images had higher image quality than those by unsupervised physicians |
| Ramsingh et al. (2019) [11] | Feasibility study, academic setting, USA | Assess anesthesiologist ability to guide remote nonmedical learners to obtain US images | 21 novice non-medically trained students | One healthy volunteer | PSL, PSS | Image acquisition time, Quality of Image | Average exam time 8.5 min, 90% cardiac images had ≥3 out of 4 quality rating |
| Olivieri et al. (2020) [12] | Feasibility study, community ICU, USA | Evaluate ability of RTMUS to approximate CU exam performed by provider | 5 novice ICU nurses | 20 patients | PSL, PSS, Subxiphoid | Concordance between RTMUS and CU and clinical test | High specificity for all abnormalities |
| Article Title | US Machine | Recording and Transmission Technology | Capture, Resolution, and Data Transfer Rate | Delay, Distortions, and Cost |
|---|---|---|---|---|
| Afset et al. (1996) [13] | 270 SSA (Toshiba) | Videoconference signals digitized by computer before transmission through digital telecommunication channels using a system called MEGA-NET | Video codec (Philips VCD 2M-G) compressed video signals by 97%. MEGA-NET capacity of 2 Mbps. | Cost of equipment ~USD 34,500 per site. Cost of video conference ~(USD 28/h) |
| Miyashita et al. (2003) [20] | Dyna View-II SSD 1700 (Aloka) | Remote-controlled camera at exam site, images transmitted using satellite links (JCSAT-1B) as videoconferencing and DICOM images | Meeting system could transmit images of 640 × 480 pixels at an upload rate of 30 fps at best. | RTMUS system cost USD 30,000 and the communication cost~ USD 4 per min. |
| Huffer et al. (2004) [21] | VISICU, Inc. | MPEG-2 compression technology | Capture rate of 32 fps, needed higher gain than usual. | |
| Boniface et al. (2011) [8] | Sonosite Micromaxx, M-Turbo (Fujifilm) | Physician communicating with paramedic via two-way radio | ||
| Otto et al. (2012) [15] | Acuson US and TeleRad workstation | Transmitted via McMurdo Station’s T-1 satellite communications link | Data link of 384 Kbps to McMurdo Station’s LAN | |
| Russell et al. (2014) [9] | Vscan(GE Healthcare) | Mentoring via Google Glass and Google Hangouts | Google Glass estimated at USD 1500 | |
| Levine et al. (2016) [18] | SonoSite S-ICU (Fujifilm) | Tele-ICU camera: images captured using Sony camera | Camera had 340° pan, 120° tilt, 18× optical, 12× digital, and 380k pixels | |
| Becker et al. (2017) [14] | Not provided | No information provided | No information provided | No information provided |
| Kim et al. (2017) [19] | Logiq S8 (GE Healthcare) | Video call (Kakao face talk) with 4G network using a Galaxy S7 (Samsung) | US machine with 1920 × 1080-pixel LED | |
| Robertson et al. (2017) [10] | SonoSite M-Turbo (FujiFilm) | Apple MacBook laptop, connected to sonographer in Haiti via an Apple iPhone 5S, both operating Apple’s FaceTime app | Apple iPhone running FaceTime using 4G cellular data network | |
| Epstein et al. (2018) [16] | Vscan (GE Healthcare) | Cellular phones, commercially available video-chat software, and 3G cellular data network | ||
| Douglas et al. (2019) [17] | SonoSite X-Porte (Fujifilm) | Two-way camera to visualize both US machine and sonographer; remote tele-intensivist used Philips monitoring software | ||
| Jensen et al. (2019) [22] | Vivid S6 (GE Healthcare) | Video grabber (DVI2USB 3.0; Epiphan Video), two web cameras, headset, two laptop computers (on-site and remote) | ||
| Ramsingh et al. (2019) [11] | SonoSite Edge (Fujifilm) | Apple FaceTime and Google Glass, with one-way visual communication and two-way audio communication | ||
| Olivieri et al. (2020) [12] | SonoSite X-Porte (Fujifilm) | Philips audiovisual communication link, Philips monitoring software, and videoconference with camera (Sony EVI-D70) | Camera had 18x lens with horizontal resolution of 470 television lines (TVL) | Facilities and equipment from preexisting tele-ICU |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salerno, A.; Kuhn, D.; El Sibai, R.; Levine, A.R.; McCurdy, M.T. Real-Time Remote Tele-Mentored Echocardiography: A Systematic Review. Medicina 2020, 56, 668. https://doi.org/10.3390/medicina56120668
Salerno A, Kuhn D, El Sibai R, Levine AR, McCurdy MT. Real-Time Remote Tele-Mentored Echocardiography: A Systematic Review. Medicina. 2020; 56(12):668. https://doi.org/10.3390/medicina56120668
Chicago/Turabian StyleSalerno, Alexis, Diane Kuhn, Rayan El Sibai, Andrea R. Levine, and Michael T. McCurdy. 2020. "Real-Time Remote Tele-Mentored Echocardiography: A Systematic Review" Medicina 56, no. 12: 668. https://doi.org/10.3390/medicina56120668