Heat-Related Illnesses Transported by United States Emergency Medical Services


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Procedures
2.3. Variables of Interest
2.4. Census Region Temperature Patterns
2.5. Statistical Analysis
3. Results
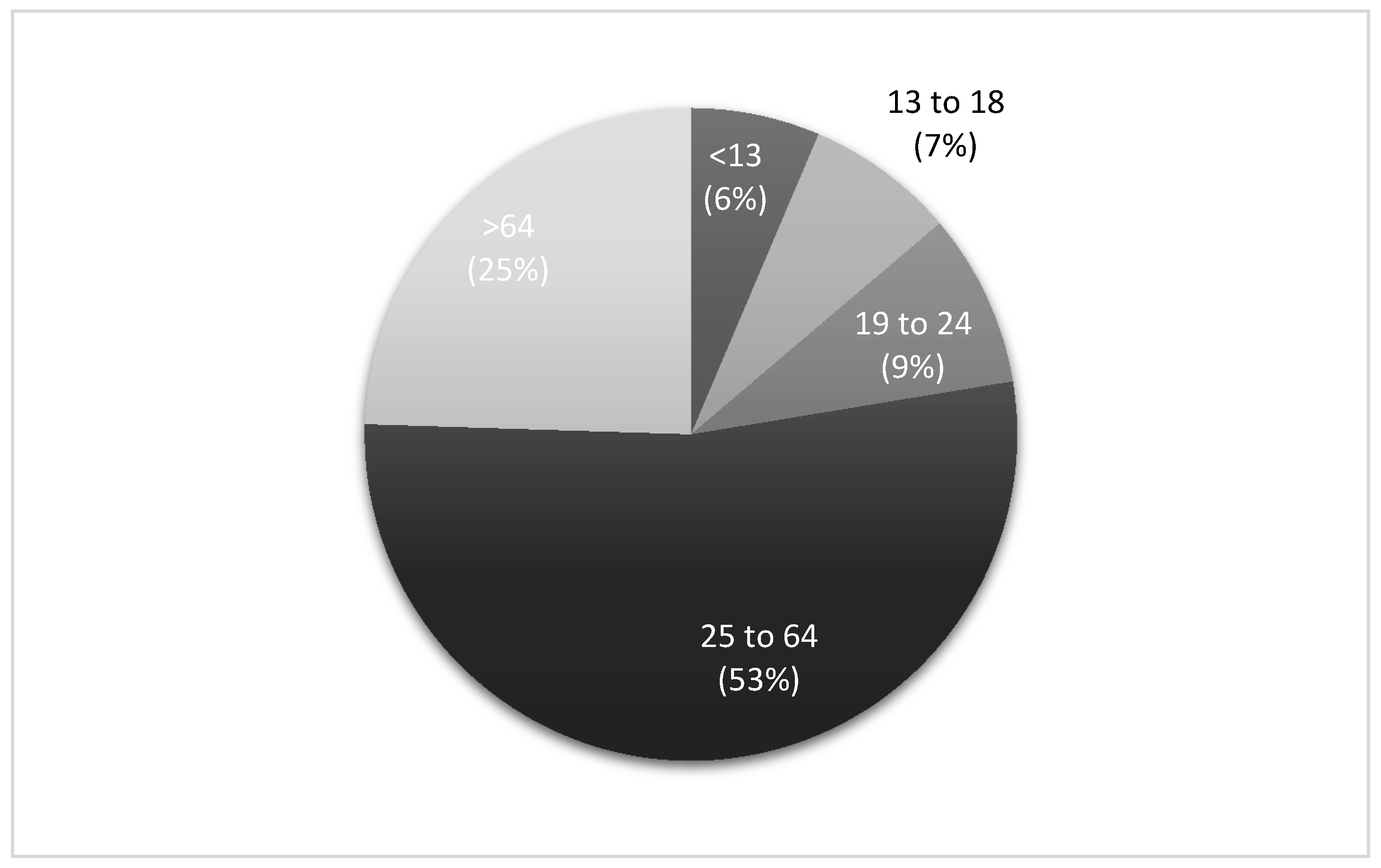
3.1. Patient Demographics
3.2. US Census Division and Urbanicity
3.3. Dispatch Date and Time
3.4. Census Division Temperature Patterns
3.5. Provider Impression and Incident Disposition
4. Discussion
4.1. Patient Demographics
4.2. US Census Division and Urbanicity
4.3. Dispatch Date and Time
4.4. Census Division Temperature Patterns
4.5. Provider Impression and Patient Disposition
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chirico, F. Comments on “Climate Change and Public Health: A Small Frame Obscures the Picture”. New Solut. J. Environ. Occup. Health Policy 2018, 28, 5–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, L.E. Exertional Heat Illnesses; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- Armstrong, L.E.; Casa, D.J.; Millard-Stafford, M.; Moran, D.S.; Pyne, S.W.; Roberts, W.O. American College of Sports Medicine position stand. Exertional heat illness during training and competition. Med. Sci. Sports Exerc. 2007, 39, 556–572. [Google Scholar] [CrossRef] [PubMed]
- Casa, D.J.; DeMartini, J.K.; Bergeron, M.F.; Csillan, D.; Eichner, E.R.; Lopez, R.M.; Ferrara, M.S.; Miller, K.C.; O’Connor, F.; Sawka, M.N.; et al. National Athletic Trainers’ Association position statement: Exertional heat illnesses. J. Athl. Train. 2015, 50, 986–1000. [Google Scholar] [CrossRef] [Green Version]
- Fechter-Leggett, E.D.; Vaidyanathan, A.; Choudhary, E. Heat Stress Illness Emergency Department Visits in National Environmental Public Health Tracking States, 2005–2010. J. Community Health 2016 41, 57–69. [CrossRef] [Green Version]
- Hess, J.J.; Saha, S.; Luber, G. Summertime Acute Heat Illness in U.S. Emergency Departments from 2006 through 2010: Analysis of a Nationally Representative Sample. Environ. Health Perspect. 2014, 122, 1209–1215. [Google Scholar] [CrossRef] [Green Version]
- Lippmann, S.J.; Fuhrmann, C.M.; Waller, A.E.; Richardson, D.B. Ambient temperature and emergency department visits for heat-related illness in North Carolina, 2007–2008. Environ. Res. 2013, 124, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.G.; Collins, C.L.; Comstock, R.D.; McKenzie, L.B. Exertional Heat-Related Injuries Treated in Emergency Departments in the U.S., 1997–2006. Am. J. Prev. Med. 2011, 40, 54–60. [Google Scholar] [CrossRef]
- Pillai, S.K.; Noe, R.S.; Murphy, M.W.; Vaidyanathan, A.; Young, R.; Kieszak, S.; Freymann, G.; Smith, W.; Drenzek, C.; Lewis, L.; et al. Heat Illness: Predictors of Hospital Admissions Among Emergency Department Visits—Georgia, 2002–2008. J. Community Health 2013, 39, 90–98. [Google Scholar] [CrossRef]
- Epstein, Y.; Yanovich, R. Heatstroke. N. Engl. J. Med. 2019, 380, 2449–2459. [Google Scholar] [CrossRef]
- Gaffin, S.; Hubbard, R. Pathophysiology of heatstroke. Med. Asp. Harsh Environ. 2001, 1, 161–208. [Google Scholar]
- Walter, E.J.; Carraretto, M. The neurological and cognitive consequences of hyperthermia. Crit. Care 2016, 20, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicario, S.J.; Okabajue, R.; Haltom, T. Rapid cooling in classic heatstroke: Effect on mortality rates. Am. J. Emerg. Med. 1986, 4, 394–398. [Google Scholar] [CrossRef]
- Centers for Disease Control. Heat-Related Deaths—United States, 1999–2003. In MMWR: Morbidity and Mortality Weekly Report; Centers for Disease Control: Atlanta, GA, USA, 2006; Volume 55, pp. 796–798. [Google Scholar]
- Santelli, J.; Sullivan, J.M.; Czarnik, A.; Bedolla, J. Heat illness in the emergency department: Keeping your cool. Emerg. Med. Pract. 2014, 16, 1–22. [Google Scholar] [PubMed]
- Armed Forces Health. Update: Heat Illness, Active Component, U.S. Armed Forces, 2018. MSMR 2018, 25, 6. [Google Scholar]
- Kerr, Z.Y.; Yeargin, S.W.; Hosokawa, Y.; Hirschhorn, R.M.; Pierpoint, L.A.; Casa, D.J. The Epidemiology and Management of Exertional Heat Illnesses in High School Sports during the 2012/2013–2016/2017 Academic Years. J. Sport Rehabil. 2020, 29, 332–338. [Google Scholar] [CrossRef]
- Yeargin, S.W.; Dompier, T.P.; Casa, D.J.; Hirschhorn, R.M.; Kerr, Z.Y. Epidemiology of exertional heat illnesses in National Collegiate Athletic Association athletes during the 2009–2010 through 2014–2015 academic years. J. Athl. Train. 2019, 54, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Argaud, L.; Ferry, T.; Le, Q.-H.; Marfisi, A.; Ciorba, D.; Achache, P.; Ducluzeau, R.; Robert, D. Short- and Long-term Outcomes of Heatstroke Following the 2003 Heat Wave in Lyon, France. Arch. Intern. Med. 2007, 167, 2177–2183. [Google Scholar] [CrossRef] [Green Version]
- Ilan, Y.; Hadad, E.; Heled, Y.; Moran, D.S.; Epstein, Y. Fatal Exertional Heat Stroke: A Case Series. Am. J. Med. Sci. 2004, 328, 84–87. [Google Scholar] [CrossRef]
- National Emergency Medical Services Information System Technical Assistance Center. National EMS Database NEMSIS Public Release Research Data Set V.3.4.0. 2018 User Manual; NEMSIS Technical Assistance Center: Salt Lake City, UT, USA, 2019. [Google Scholar]
- U.S. Census Bureau. Census Regions and Divisions of the United States; U.S. Census Bureau: Suitland, MD, USA, 2010.
- United States Department of Agriculture. Urban Influence Codes; Cromartie, J., Ed.; United States Department of Agriculture: Washington, DC, USA, 2013.
- Vose, R.S.; Applequist, S.; Squires, M.; Durre, I.; Menne, M.J.; Williams, C.N.; Fenimore, C.; Gleason, K.; Arndt, D. Improved Historical Temperature and Precipitation Time Series for U.S. Climate Divisions. J. Appl. Meteorol. Clim. 2014, 53, 1232–1251. [Google Scholar] [CrossRef]
- McLaren, C.; Null, J.; Quinn, J. Heat Stress from Enclosed Vehicles: Moderate Ambient Temperatures Cause Significant Temperature Rise in Enclosed Vehicles. Pediatrics 2005, 116, e109–e112. [Google Scholar] [CrossRef] [Green Version]
- Chirico, F.; Magnavita, N. The significant role of health surveillance in the occupational heat stress assessment. Int. J. Biometeorol. 2018, 63, 193–194. [Google Scholar] [CrossRef] [PubMed]
- Dunn, R.J.; Kim, T.Y. Pediatric heat-related illness: Recommendations for prevention and management. Pediatr. Emerg. Med. Pract. 2017, 14, 1–20. [Google Scholar] [PubMed]
- Morano, L.H.; Watkins, S.; Kintziger, K. A Comprehensive Evaluation of the Burden of Heat-Related Illness and Death within the Florida Population. Int. J. Environ. Res. Public Health 2016, 13, 551. [Google Scholar] [CrossRef]
- Carter, R.; Cheuvront, S.N.; Williams, J.O.; Kolka, M.A.; Stephenson, L.A.; Sawka, M.N.; Amoroso, P.J. Epidemiology of Hospitalizations and Deaths from Heat Illness in Soldiers. Med. Sci. Sports Exerc. 2005, 37, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Gronlund, C.J. Racial and Socioeconomic Disparities in Heat-Related Health Effects and Their Mechanisms: A Review. Curr. Epidemiol. Rep. 2014, 1, 165–173. [Google Scholar] [CrossRef]
- Nalliah, R.P.; Anderson, I.M.; Lee, M.K.; Rampa, S.; Allareddy, V.; Allareddy, V. Epidemiology of Hospital-Based Emergency Department Visits Due to Sports Injuries. Pediatr. Emerg. Care 2014, 30, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Padegimas, E.M.; Stepan, J.G.; Stoker, G.E.; Polites, G.M.; Brophy, R.H. Epidemiology and Severity of Sports and Recreation Injuries Presenting to a Tertiary Adult Emergency Department. Physician Sportsmed. 2016, 44, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.M.; Brown, D.E.; Nelson, E.A. Epidemiology of Pediatric EMS Practice: A Multistate Analysis. Prehosp. Disaster Med. 1996, 11, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Gifford, R.M.; Todisco, T.; Stacey, M.; Fujisawa, T.; Allerhand, M.; Woods, D.; Reynolds, R.M. Risk of heat illness in men and women: A systematic review and meta-analysis. Environ. Res. 2019, 171, 24–35. [Google Scholar] [CrossRef]
- Chirico, F. Implications of climate change for thermal risk assessment in indoor workplaces. Environ. Dis. 2017, 2, 103. [Google Scholar] [CrossRef]
- Nelson, D.A.; Deuster, P.A.; O’Connor, F.G.; Kurina, L.M. Timing and Predictors of Mild and Severe Heat Illness among New Military Enlistees. Med. Sci. Sports Exerc. 2018, 50, 1603–1612. [Google Scholar] [CrossRef]
- Grundstein, A.J.; Hosokawa, Y.; Casa, D.J. Fatal Exertional Heat Stroke and American Football Players: The Need for Regional Heat-Safety Guidelines. J. Athl. Train. 2018, 53, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundstein, A.J.; Duzinski, S.; Null, J. Impact of dangerous microclimate conditions within an enclosed vehicle on pediatric thermoregulation. Theor. Appl. Clim. 2015, 127, 103–110. [Google Scholar] [CrossRef]
- Grundstein, A.J.; Duzinski, S.V.; Dolinak, D.; Null, J.; Iyer, S.S. Evaluating infant core temperature response in a hot car using a heat balance model. Forensic Sci. Med. Pathol. 2014, 11, 13–19. [Google Scholar] [CrossRef]
- Kark, J.A.; Burr, P.Q.; Wenger, C.B.; Gastaldo, E.; Gardner, J.W. Exertional heat illness in Marine Corps recruit training. Aviat. Space Environ. Med. 1996, 67, 354–360. [Google Scholar]
- Sugg, M.M.; Konrad, C.E.; Fuhrmann, C.M. Relationships between maximum temperature and heat-related illness across North Carolina, USA. Int. J. Biometeorol. 2015, 60, 663–675. [Google Scholar] [CrossRef]
- Yow, D.M. Urban Heat Islands: Observations, Impacts, and Adaptation. Geogr. Compass 2007, 1, 1227–1251. [Google Scholar] [CrossRef]
- Mann, N.C.; Kane, L.; Dai, M.; Jacobson, K. Description of the 2012 NEMSIS Public-Release Research Dataset. Prehosp. Emerg. Care 2015, 19, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Grundstein, A.; Elguindi, N.; Cooper, E.; Ferrara, M. Exceedance of wet bulb globe temperature safety thresholds in sports under a warming climate. Clim. Res. 2013, 58, 183–191. [Google Scholar] [CrossRef]
- Zeller, L.; Novack, V.; Barski, L.; Jotkowitz, A.; Almog, Y. Exertional heatstroke: Clinical characteristics, diagnostic and therapeutic considerations. Eur. J. Intern. Med. 2011, 22, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Morano, L.H.; Watkins, S. Evaluation of Diagnostic Codes in Morbidity and Mortality Data Sources for Heat-Related Illness Surveillance. Public Health Rep. 2017, 132, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryor, R.R.; Roth, R.N.; Suyama, J.; Hostler, D. Exertional Heat Illness: Emerging Concepts and Advances in Prehospital Care. Prehosp. Disaster Med. 2015, 30, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Rowland, T. Thermoregulation during exercise in the heat in children: Old concepts revisited. J. Appl. Physiol. 2008, 105, 718–724. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Frequency (n) | Percent (%) | |
|---|---|---|
| American Indian or Alaska Native | 196 | 1.0 |
| Asian | 173 | 0.9 |
| Black or African-American | 3889 | 19.9 |
| Hispanic or Latino | 1380 | 7.1 |
| Native Hawaiian or Other Pacific Islander | 66 | 0.3 |
| White | 10,878 | 55.6 |
| Not Documented | 2996 | 15.3 |
| Total | 19,578 | 100.0 |
| Frequency (n) | Percent (%) | |
|---|---|---|
| East North Central | 3330 | 9.6 |
| East South Central | 2130 | 6.1 |
| Middle Atlantic | 1418 | 4.1 |
| Mountain | 4861 | 14.0 |
| New England | 891 | 2.6 |
| Pacific | 4046 | 11.6 |
| South Atlantic | 11,732 | 33.7 |
| Territories | 16 | 0.1 |
| West North Central | 2598 | 7.5 |
| West South Central | 3792 | 10.9 |
| Total | 34,814 | 100.0 |
| DIVISION | Winter | Spring | Summer | Fall | Diff_Win | Diff_Spr | Diff_Sum | Diff_Fall |
|---|---|---|---|---|---|---|---|---|
| East North Central | 2.1 | 14.2 | 27.1 | 15.6 | 1.6 | −0.2 | 0.1 | −0.2 |
| East South Central | 13.5 | 23.0 | 31.0 | 23.0 | 1.9 | 0.6 | −0.3 | 0.0 |
| Middle Atlantic | 3.1 | 13.3 | 26.1 | 15.8 | 1.5 | −0.5 | 0.1 | 0.2 |
| Mountain | 5.7 | 16.9 | 29.5 | 17.3 | 0.7 | 1.1 | 1.2 | 0.5 |
| New England | 0.1 | 10.8 | 25.0 | 14.1 | 1.0 | −0.5 | 0.5 | 0.5 |
| Pacific | 8.6 | 17.1 | 29.5 | 19.2 | 0.3 | 0.4 | 1.6 | 0.6 |
| South Atlantic | 15.4 | 23.1 | 30.8 | 23.9 | 1.9 | 0.3 | −0.1 | 0.5 |
| West North Central | 1.4 | 15.3 | 28.8 | 15.6 | 0.8 | 0.0 | 0.4 | −0.5 |
| West South Central | 15.8 | 25.9 | 33.8 | 24.7 | 1.4 | 1.4 | 0.4 | −0.2 |
| Age Group | Heat Stroke | Heat Syncope | Heat Cramps | Heat Exhaustion | Other | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| <13 | 530 | 1.5 | 14 | 0.0 | 16 | 0.1 | 1590 | 4.6 | 84 | 0.2 |
| 13 to 18 | 301 | 0.9 | 19 | 0.1 | 13 | 0.0 | 2186 | 6.3 | 47 | 0.1 |
| 19 to 24 | 425 | 1.2 | 31 | 0.1 | 37 | 0.1 | 2455 | 7.1 | 53 | 0.2 |
| 25 to 64 | 2890 | 8.3 | 109 | 0.3 | 186 | 0.5 | 14,987 | 43.0 | 317 | 0.9 |
| >64 | 1809 | 5.2 | 125 | 0.4 | 52 | 0.2 | 6383 | 18.3 | 155 | 0.4 |
| Total | 5955 | 17.1 | 298 | 0.9 | 304 | 0.9 | 27,601 | 79.3 | 656 | 1.9 |
| Frequency (n) | Percent (%) | |
|---|---|---|
| Assist | 245 | 0.7 |
| Canceled | 75 | 0.2 |
| Patient Dead at Scene | 5 | 0.0 |
| No Transport * | 4244 | 12.2 |
| Patient Treated, Released | 5598 | 16.1 |
| Patient Treated, Transported | 24,539 | 70.5 |
| Patient Treated, Transported by Private Vehicle | 108 | 0.3 |
| Total | 34,814 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeargin, S.; Hirschhorn, R.; Grundstein, A. Heat-Related Illnesses Transported by United States Emergency Medical Services. Medicina 2020, 56, 543. https://doi.org/10.3390/medicina56100543
Yeargin S, Hirschhorn R, Grundstein A. Heat-Related Illnesses Transported by United States Emergency Medical Services. Medicina. 2020; 56(10):543. https://doi.org/10.3390/medicina56100543
Chicago/Turabian StyleYeargin, Susan, Rebecca Hirschhorn, and Andrew Grundstein. 2020. "Heat-Related Illnesses Transported by United States Emergency Medical Services" Medicina 56, no. 10: 543. https://doi.org/10.3390/medicina56100543