The Role of Non-Selective β-Blockers in Compensated Cirrhotic Patients without Major Complications

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Compliance with Ethical Requirements
2.2. Data Sources
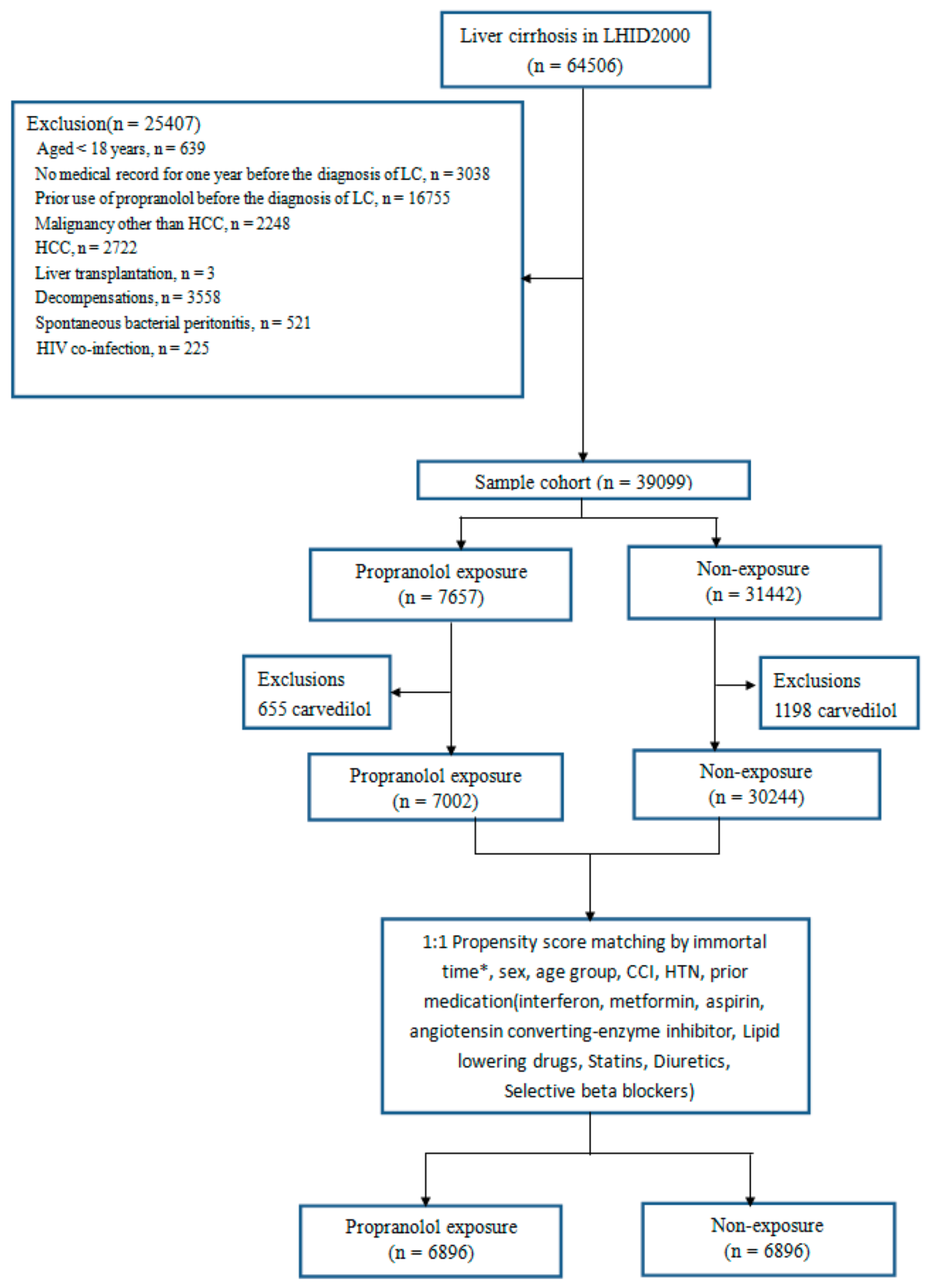
2.3. Study Cohort, and Inclusion and Exclusion Criteria
2.4. Definition of PPL Exposure
2.5. Study Outcomes
2.6. Confounder Assessment
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
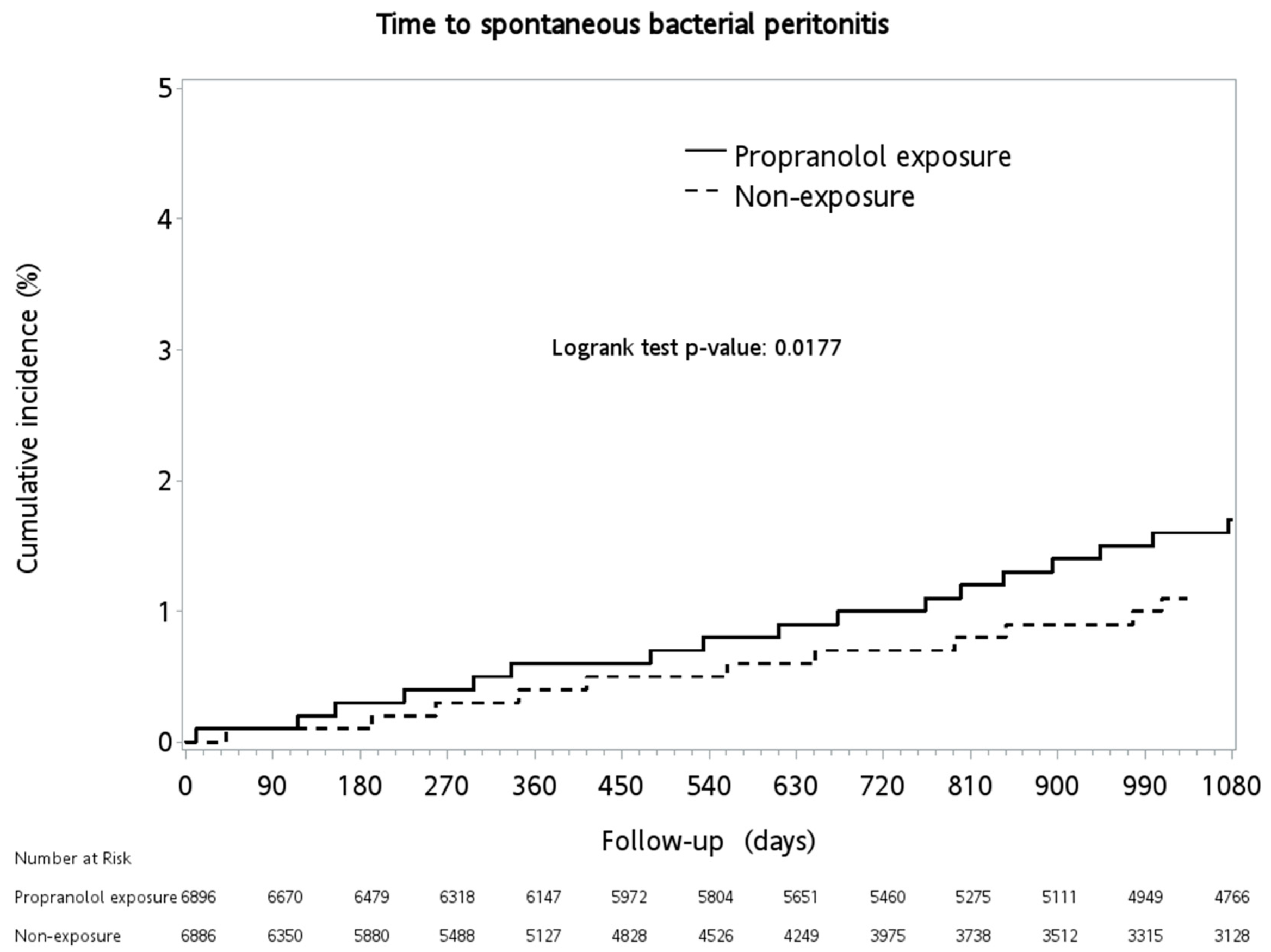
3.2. Outcomes of Spontaneous Bacterial Peritonitis and Assessments of Risk Factors
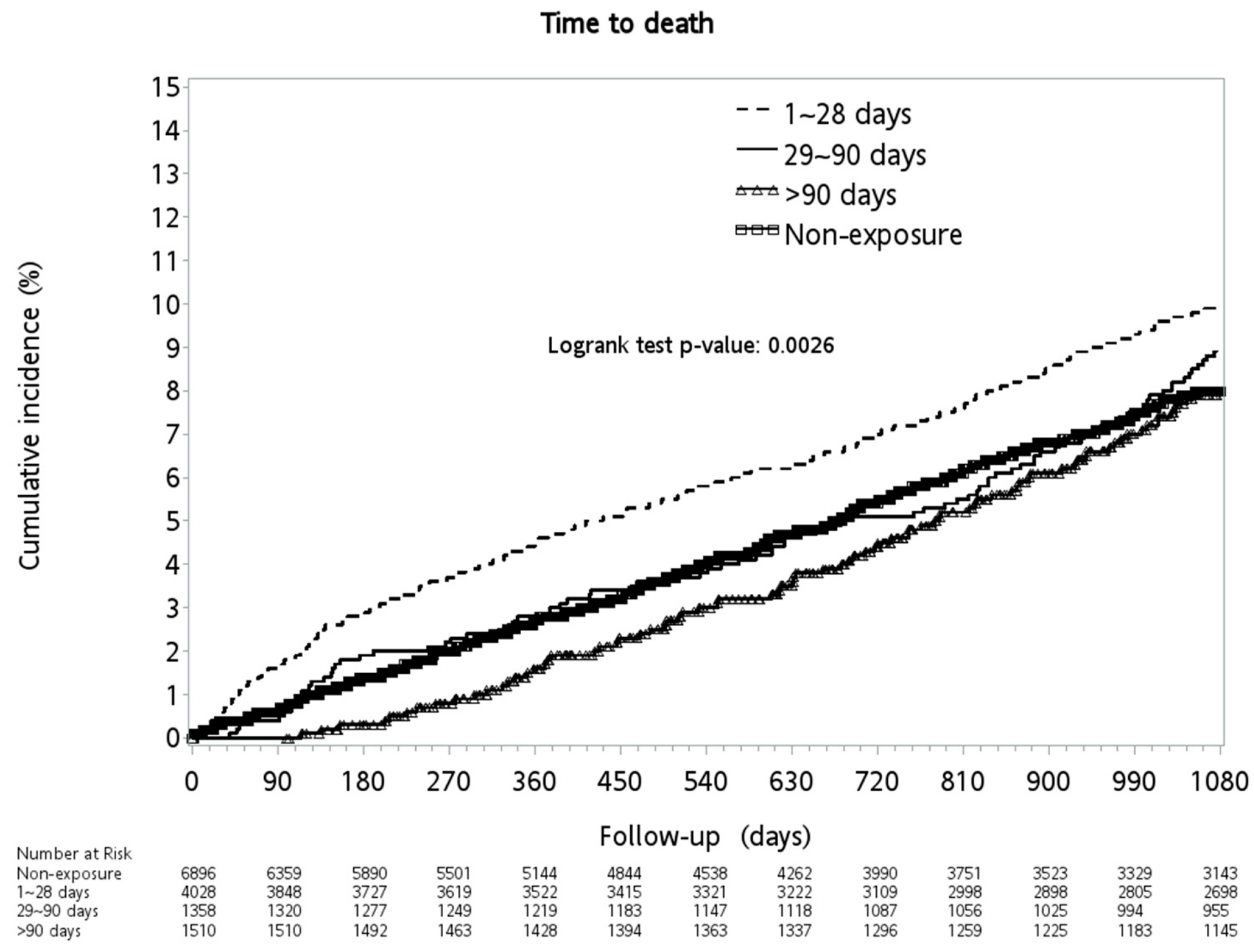
3.3. All-Cause Mortality
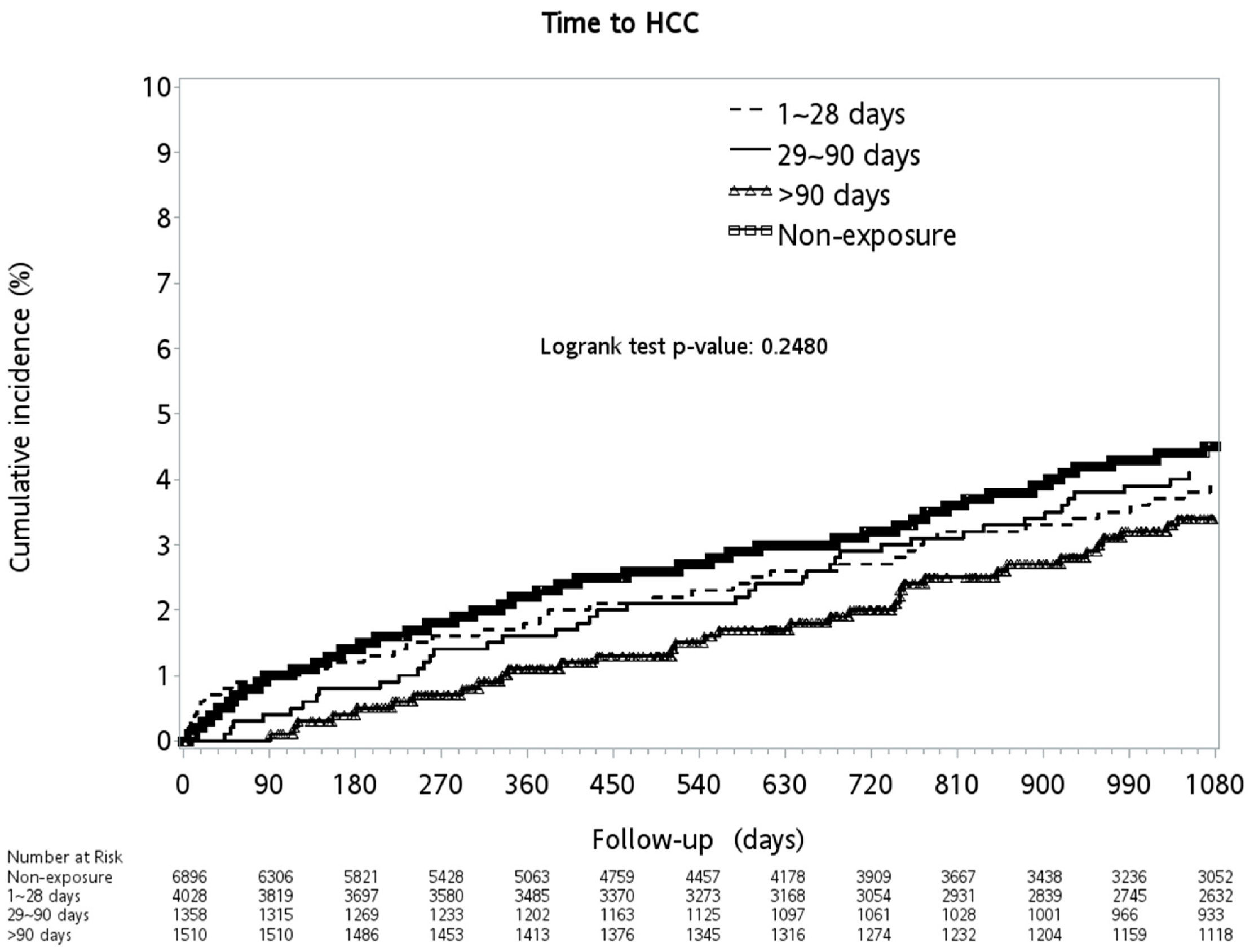
3.4. Outcomes of Hepatocellular Carcinoma and Assessments of Risk Factors
4. Discussions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lebrec, D.; Corbic, M.; Nouel, O.; Benhamou, J.P. PPL—A medical treatment for portal hypertension? Lancet 1980, 2, 180–182. [Google Scholar] [CrossRef]
- Garcia-Tsao, G.; Abraldes, J.G.; Berzigotti, A.; Bosch, J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017, 65, 310–335. [Google Scholar] [CrossRef] [Green Version]
- de Franchis, R.; Baveno, V.I. Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villanueva, C.; Albillos, A.; Genescà, J.; Abraldes, J.G.; Calleja, J.L.; Aracil, C.; Bañares, R.; Morillas, R.; Poca, M.; Peñas, B.; et al. Development of hyperdynamic circulation and response to β-blockers in compensated cirrhosis with portal hypertension. Hepatology 2016, 63, 197–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villanueva, C.; Albillos, A.; Genescà, J.; Garcia-Pagan, J.C.; Calleja, J.L.; Aracil, C.; Bañares, R.; Morillas, R.M.; Poca, M.; Peñas, B.; et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2019, 393, 1597–1608. [Google Scholar] [CrossRef]
- Chirapongsathorn, S.; Valentin, N.; Alahdab, F.; Krittanawong, C.; Erwin, P.J.; Murad, M.H.; Kamath, P.S. β-Blockers and Survival in Patients with Cirrhosis and Ascites: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 1096–1104. [Google Scholar] [CrossRef] [Green Version]
- Bang, U.C.; Benfield, T.; Hyldstrup, L.; Jensen, J.E.; Bendtsen, F. Effect of PPL on survival in patients with decompensated cirrhosis: A nationwide study based Danish patient registers. Liver Int. 2016, 36, 1304–1312. [Google Scholar] [CrossRef]
- Onali, S.; Kalafateli, M.; Majumdar, A.; Westbrook, R.; O’Beirne, J.; Leandro, G.; Patch, D.; Tsochatzis, E.A. Non-selective beta-blockers are not associated with increased mortality in cirrhotic patients with ascites. Liver Int. 2017, 37, 1334–1344. [Google Scholar] [CrossRef] [Green Version]
- Bossen, L.; Krag, A.; Vilstrup, H.; Watson, H.; Jepsen, P. Nonselective β-blockers do not affect mortality in cirrhosis patients with ascites: Post Hoc analysis of three randomized controlled trials with 1198 patients. Hepatology 2016, 63, 1968–1976. [Google Scholar] [CrossRef]
- Kalambokis, G.N.; Christodoulou, D.; Baltayiannis, G.; Christou, L. PPL use beyond 6 months increases mortality in patients with Child-Pugh C cirrhosis and ascites. Hepatology 2016, 64, 1806–1808. [Google Scholar] [CrossRef]
- Chang, P.Y.; Huang, W.Y.; Lin, C.L.; Huang, T.C.; Wu, Y.Y.; Chen, J.H.; Kao, C.H. PPL Reduces Cancer Risk: A Population-Based Cohort Study. Medicine 2015, 94, 1097. [Google Scholar] [CrossRef]
- Monami, M.; Filippi, L.; Ungar, A.; Sgrilli, F.; Antenore, A.; Dicembrini, I.; Bagnoli, P.; Marchionni, N.; Rotella, C.M.; Mannucci, E. Further data on beta-blockers and cancer risk: Observational study and meta-analysis of randomized clinical trials. Curr. Med. Res. Opin. 2013, 29, 369–378. [Google Scholar] [CrossRef]
- Herrera, I.; Pascual, S.; Zapater, P.; Carnicer, F.; Bellot, P.; María Palazón, J. The use of β-blockers is associated with a lower risk of developing hepatocellular carcinoma in patients with cirrhosis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1194–1197. [Google Scholar] [CrossRef]
- Thiele, M.; Albillos, A.; Abazi, R.; Wiest, R.; Gluud, L.L.; Krag, A. Non-selective beta-blockers may reduce risk of hepatocellular carcinoma: A meta-analysis of randomized trials. Liver Int. Off. J. Int. Assoc. Study Liver 2015, 35, 2009–2016. [Google Scholar] [CrossRef]
- Longitudinal Health Insurance Database 2000 (LHID 2000), National Health Insurance Research Database. Taiwan at. Available online: https://nhird.nhri.org.tw/en/Data_Subsets.html (accessed on 1 May 2019).
- WHO Collaborating Center for Drugs Statistics Methodology: ATC/DDD Index 2013. Available online: http://www.whocc.no/atc_ddd_index/ (accessed on 1 May 2019).
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Villanueva, C.; Aracil, C.; Turnes, J.; Hernandez-Guerra, M.; Genesca, J.; García-Pagán, J.C.; Torres, F.; Calleja, J.L.; Albillos, A. Addition of Simvastatin to Standard Therapy for the Prevention of Variceal Rebleeding Does Not Reduce Rebleeding but Increases Survival in Patients with Cirrhosis. Gastroenterology 2016, 150, 1160–1170. [Google Scholar] [CrossRef] [Green Version]
- Kim, R.G.; Loomba, R.; Prokop, L.J.; Singh, S. Statin Use and Risk of Cirrhosis and Related Complications in Patients with Chronic Liver Diseases: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2017, 15, 1521–1530. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Tsao, G.; Friedman, S.; Iredale, J.; Pinzani, M. Now there are many (stages) where before there was one: In search of pathophysiological classification of cirrhosis. Hepatology 2010, 51, 1445–1449. [Google Scholar] [CrossRef] [Green Version]
- Ripoll, C.; Groszmann, R.; Garcia-Tsao, G.; Grace, N.; Burroughs, A.; Planas, R.; Escorsell, A.; García-Pagán, J.C.; Makuch, R.; Patch, D. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology 2007, 133, 481–488. [Google Scholar] [CrossRef]
- Poynard, T.; Cale’s, P.; Pasta, L.; Ideo, G.; Pascal, J.P.; Pagliaro, L.; Lebrec, D. Franco—Italian Multicenter Study Group. Betaadrenergic-antagonist drugs in the prevention of gastrointestinal bleeding in patients with cirrhosis and esophageal varices: An analysis of data and prognostic factors in 589 patients from four randomized clinical trials. N. Engl. J. Med. 1991, 324, 1532–1538. [Google Scholar]
- Mandorfer, M.; Bota, S.; Schwabl, P.; Bucsics, T.; Pfisterer, N.; Kruzik, M.; Hagmann, M.; Blacky, A.; Ferlitsch, A.; Sieghart, W.; et al. Nonselective β blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology 2014, 146, 1680–9160. [Google Scholar] [CrossRef] [Green Version]
- Groszmann, R.J.; Garcia-Tsao, G.; Bosch, J.; Grace, N.D.; Burroughs, A.K.; Planas, R.; Escorsell, A.; Garcia-Pagan, J.C.; Patch, D.; Matloff, D.S.; et al. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N. Engl. J. Med. 2005, 353, 2254–2261. [Google Scholar] [CrossRef] [Green Version]
- Abraldes, J.G.; Iwakiri, Y.; Loureiro-Silva, M.; Haq, O.; Sessa, W.C.; Groszmann, R.J. Mild increases in portal pressure up-regulate VEGF and eNOS in the intestinal microcirculation leading to hyperdynamic state. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 290, 980–987. [Google Scholar] [CrossRef] [Green Version]
- Brito-Azevedo, A.; de Mello Perez, R.; Coelho, H.S.M.; Fernandes, E.D.S.M.; Castiglione, R.C.; Villela-Nogueira, C.A.; Bouskela, E. PPL improves endothelial dysfunction in advanced cirrhosis: The ‘endothelial exhaustion’ hypothesis. Gut 2016, 65, 1391–1392. [Google Scholar] [CrossRef]
- Reiberger, T.; Ferlitsch, A.; Payer, B.A.; Mandorfer, M.; Heinisch, B.B.; Hayden, H.; Lammert, F.; Trauner, M.; Peck-Radosavljevic, M.; Vogelsang, H.; et al. Non-selective betablocker therapy decreases intestinal permeability and serum levels of LBP and IL-6 in patients with cirrhosis. J. Hepatol. 2013, 58, 911–921. [Google Scholar] [CrossRef]
- Brito-Azevedo, A.; de Mello Perez, R.; Coelho, H.S.M.; Fernandes, E.D.S.M.; Castiglione, R.C.; Villela-Nogueira, C.A.; Bouskela, E. The anti-inflammatory role of PPL in cirrhosis: Preventing the inflammatory exhaustion? J. Hepatol. 2017, 66, 240–241. [Google Scholar] [CrossRef] [Green Version]
- Ripoll, C.; Groszmann, R.J.; Garcia-Tsao, G.; Bosch, J.; Grace, N.; Burroughs, A.; Planas, R.; Escorsell, A.; Garcia-Pagan, J.C.; Makuch, R.; et al. Hepatic venous pressure gradient predicts development of hepatocellular carcinoma independently of severy of cirrhosis. J. Hepatol. 2009, 50, 923–928. [Google Scholar] [CrossRef] [Green Version]
- Kassahun, W.T.; Guenl, B.; Ungemach, F.R.; Jonas, S.; Abraham, G. Expression and functional coupling of liver beta2—Adrenoceptors in the human hepatocellular carcinoma. Pharmacology 2012, 89, 313–320. [Google Scholar] [CrossRef]
- Sinagra, E.; Perricone, G.; D’Amico, M.; Tinè, F.; D’Amico, G. Systematic review with meta-analysis: The haemodynamic effects of carvedilol compared with propranolol for portal hypertension in cirrhosis. Aliment. Pharmacol. Ther. 2014, 39, 557–568. [Google Scholar] [CrossRef]
- Gupta, V.; Rawat, R.; Shalimar Saraya, A. Carvedilol versus propranolol effect on hepatic venous pressure gradient at 1 month in patients with index variceal bleed: RCT. Hepatol. Int. 2017, 11, 181–187. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Bureau, C.; Stefanescu, H.; Augustin, S.; Ney, M.; Blasco, H.; Procopet, B.; Bosch, J.; Genesca, J.; Berzigotti, A. Noninvasive tools and risk of clinically significant portal hypertension and varices in compensated cirrhosis: The “Anticipate” study. Hepatology 2016, 64, 2173–2184. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Exposure | Non-Exposure | ||||||
|---|---|---|---|---|---|---|---|---|
| N | n | (%) | n | (%) | SMD | p-Value | ||
| Total | 13,792 | 6896 | (50.00) | 6896 | (50.00) | |||
| Sex | 0.8196 | |||||||
| Female | 5237 | 2625 | (38.07) | 2612 | (37.88) | 0.00 | ||
| Male | 8555 | 4271 | (61.93) | 4284 | (62.12) | 0.00 | ||
| Age group | 0.01 | 0.7577 | ||||||
| 18–34 | 3254 | 1609 | (23.33) | 1645 | (23.85) | |||
| 35–49 | 5463 | 2722 | (39.47) | 2741 | (39.75) | |||
| 50–64 | 3461 | 1755 | (25.45) | 1706 | (24.74) | |||
| 65+ | 1614 | 810 | (11.75) | 804 | (11.66) | |||
| Covariate | ||||||||
| Acute myocardial infarction | 12 | 9 | (0.13) | 3 | (0.04) | 0.03 | 0.0831 | |
| Congestive heart failure | 111 | 67 | (0.97) | 44 | (0.64) | 0.04 | 0.0284 | |
| Peripheral vascular disease | 32 | 18 | (0.26) | 14 | (0.20) | 0.01 | 0.4790 | |
| Cerebral vascular accident | 369 | 184 | (2.67) | 185 | (2.68) | 0.00 | 0.9579 | |
| Dementia | 37 | 20 | (0.29) | 17 | (0.25) | 0.01 | 0.6214 | |
| Pulmonary disease | 876 | 449 | (6.51) | 427 | (6.19) | 0.01 | 0.4424 | |
| Connective tissue disorder | 99 | 52 | (0.75) | 47 | (0.68) | 0.01 | 0.6140 | |
| Peptic ulcer | 2194 | 1113 | (16.14) | 1081 | (15.68) | 0.01 | 0.4563 | |
| Liver cirrhosis | 3447 | 1964 | (28.48) | 1483 | (21.51) | <0.0001 | ||
| Hepatitis B Virus | 7885 | 3605 | (52.28) | 4280 | (62.06) | <0.0001 | ||
| Hepatitis C Virus | 3079 | 1653 | (23.97) | 1426 | (20.68) | <0.0001 | ||
| Alcohol | 3544 | 2159 | (31.31) | 1385 | (20.08) | <0.0001 | ||
| Diabetes | 920 | 485 | (7.03) | 435 | (6.31) | 0.03 | 0.0879 | |
| Diabetes complications | 189 | 115 | (1.67) | 74 | (1.07) | 0.05 | 0.0027 | |
| Paraplegia | 36 | 18 | (0.26) | 18 | (0.26) | 0.00 | 1.0000 | |
| Renal disease | 250 | 139 | (2.02) | 111 | (1.61) | 0.03 | 0.0739 | |
| Severe liver disease | 3 | 2 | (0.03) | 1 | (0.01) | 0.01 | 0.5637 | |
| Hypertension | 1969 | 1032 | (14.97) | 937 | (13.59) | 0.04 | 0.0208 | |
| Prior medications | ||||||||
| Interferon-based therapy | ||||||||
| interferon | 43 | 23 | (0.33) | 20 | (0.29) | 0.01 | 0.6468 | |
| Metformin | 605 | 328 | (4.76) | 277 | (4.02) | 0.04 | 0.0340 | |
| Aspirin | 520 | 286 | (4.15) | 234 | (3.39) | 0.04 | 0.0201 | |
| Angiotensin converting-enzyme inhibitor | 376 | 200 | (2.90) | 176 | (2.55) | 0.02 | 0.2095 | |
| Captopril | 136 | 70 | (1.02) | 66 | (0.96) | 0.7303 | ||
| Lisinopril | 63 | 35 | (0.51) | 28 | (0.41) | 0.3767 | ||
| Perindopril | 51 | 25 | (0.36) | 26 | (0.38) | 0.8884 | ||
| Ramipril | 42 | 23 | (0.33) | 19 | (0.28) | 0.5365 | ||
| Quinapril | 26 | 13 | (0.19) | 13 | (0.19) | 1.0000 | ||
| Benazepril | 3 | 2 | (0.03) | 1 | (0.01) | 0.5637 | ||
| Cilazapril | 17 | 8 | (0.12) | 9 | (0.13) | 0.8082 | ||
| Fosinopril | 62 | 36 | (0.52) | 26 | (0.38) | 0.2031 | ||
| Lipid lowering drugs | 222 | 129 | (1.87) | 93 | (1.35) | 0.04 | 0.0149 | |
| Clofibrate | 0.0149 | |||||||
| Bezafibrate | 30 | 13 | (0.19) | 17 | (0.25) | 0.4647 | ||
| Gemfibrozil | 129 | 78 | (1.13) | 51 | (0.74) | 0.0169 | ||
| Fenofibrate | 74 | 44 | (0.64) | 30 | (0.44) | 0.1027 | ||
| Nicotinic acid | 4 | 2 | (0.03) | 2 | (0.03) | 1.0000 | ||
| Acipimox | 7 | 6 | (0.09) | 1 | (0.01) | 0.0587 | ||
| Statins | 81 | 48 | (0.70) | 33 | (0.48) | 0.03 | 0.0946 | |
| Atorvastatin | 0.0946 | |||||||
| Fluvastatin | 47 | 26 | (0.38) | 21 | (0.30) | 0.4650 | ||
| Pitavastatin | 0.4650 | |||||||
| Rosuvastatin | 30 | 19 | (0.28) | 11 | (0.16) | 0.1437 | ||
| Simvastatin | 7 | 5 | (0.07) | 2 | (0.03) | 0.2567 | ||
| Diuretics | 272 | 145 | (2.10) | 127 | (1.84) | 0.02 | 0.2703 | |
| Furosemide | 233 | 125 | (1.81) | 108 | (1.57) | 0.2613 | ||
| Spironolactone | 75 | 36 | (0.52) | 39 | (0.57) | 0.7283 | ||
| Selective beta blockers | 577 | 293 | (4.25) | 284 | (4.12) | 0.01 | 0.7019 | |
| Variable | N | Exposure | Non-Exposure | p-Value | ||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | |||
| Total | 13,792 | 6896 | (50.00) | 6896 | (50.00) | |
| Spontaneous bacterial peritonitis | 150 | 98 | (1.42) | 52 | (0.75) | 0.0002 |
| Decompensation | 546 | 396 | (5.74) | 150 | (2.18) | <0.0001 |
| Hepatorenal syndrome | 28 | 18 | (0.26) | 10 | (0.15) | 0.1302 |
| Other sequelae of chronic liver disease | 41 | 29 | (0.42) | 12 | (0.17) | 0.0078 |
| Ascites | 342 | 298 | (4.32) | 44 | (0.64) | <0.0001 |
| Jaundice | 75 | 54 | (0.78) | 21 | (0.30) | 0.0001 |
| Hepatic coma | 294 | 191 | (2.77) | 103 | (1.49) | <0.0001 |
| Variceal bleeding | 260 | 197 | (2.86) | 63 | (0.91) | <0.0001 |
| All-cause mortality | 966 | 577 | (8.37) | 389 | (5.64) | <0.0001 |
| Liver transplantation | 21 | 6 | (0.09) | 15 | (0.22) | 0.0494 |
| HCC | 462 | 232 | (3.36) | 230 | (3.34) | 0.9246 |
| Variable | Adjusted HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Propranolol Exposure vs. Non-Exposure | 1.24 | (0.88) | (1.75) | 0.2111 |
| Sex | ||||
| Male vs. female | 1.90 | (1.30) | (2.76) | 0.0008 |
| Age Group | ||||
| 18–34 | ||||
| 35–49 | 1.15 | (0.66) | (2.00) | 0.6204 |
| 50–64 | 1.34 | (0.74) | (2.40) | 0.3307 |
| 65+ | 2.02 | (1.08) | (3.75) | 0.0270 |
| Covariate | ||||
| CCI | ||||
| Congestive heart failure | 1.98 | (0.76) | (5.11) | 0.1603 |
| Peripheral vascular disease | 2.98 | (0.41) | (21.83) | 0.2819 |
| Cerebral vascular accident | 0.53 | (0.18) | (1.61) | 0.2657 |
| Pulmonary disease | 0.92 | (0.52) | (1.63) | 0.7716 |
| Peptic ulcer | 1.27 | (0.86) | (1.88) | 0.2279 |
| Liver cirrhosis | 1.02 | (0.69) | (1.49) | 0.9260 |
| Diabetes | 1.17 | (0.61) | (2.24) | 0.6318 |
| Diabetes complications | 0.57 | (0.17) | (1.90) | 0.3612 |
| Paraplegia | 4.72 | (0.55) | (40.53) | 0.1570 |
| Renal disease | 1.63 | (0.70) | (3.80) | 0.2605 |
| Hypertension | 0.71 | (0.43) | (1.18) | 0.1845 |
| Baseline Medications | ||||
| Metformin | 1.41 | (0.67) | (2.95) | 0.3676 |
| Aspirin | 0.45 | (0.17) | (1.15) | 0.0949 |
| Angiotensin converting-enzyme inhibitor | 0.82 | (0.34) | (2.01) | 0.6670 |
| Lipid lowering drugs | 1.10 | (0.35) | (3.52) | 0.8688 |
| Diuretics | 1.83 | (0.96) | (3.47) | 0.0652 |
| Selective beta blockers | 0.83 | (0.34) | (2.04) | 0.6904 |
| Concomitant Medications | ||||
| Selective beta blockers | 0.35 | (0.19) | (0.67) | 0.0014 |
| Diuretics | 8.56 | (5.93) | (12.37) | <0.0001 |
| Variable | Adjusted HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Propranolol Exposure | ||||
| 1~28 Days vs. non-exposure | 1.33 | (1.15) | (1.53) | 0.0001 |
| 29~90 Days vs. non-exposure | 1.12 | (0.91) | (1.40) | 0.2888 |
| >90 Days vs. non-exposure | 0.79 | (0.64) | (0.98) | 0.0340 |
| Sex | ||||
| Male vs. female | 1.59 | (1.38) | (1.83) | <0.0001 |
| Age Group | ||||
| 18–34 | ||||
| 35–49 | 1.73 | (1.34) | (2.21) | <0.0001 |
| 50–64 | 2.63 | (2.04) | (3.40) | <0.0001 |
| 65+ | 5.07 | (3.89) | (6.61) | <0.0001 |
| Covariate | ||||
| CCI | ||||
| Acute myocardial infarction | 2.27 | (0.89) | (5.82) | 0.0870 |
| Congestive heart failure | 1.37 | (0.95) | (1.97) | 0.0914 |
| Peripheral vascular disease | 3.15 | (1.67) | (5.93) | 0.0004 |
| Cerebral vascular accident | 1.56 | (1.20) | (2.01) | 0.0008 |
| Dementia | 1.86 | (1.04) | (3.32) | 0.0350 |
| Pulmonary disease | 1.25 | (1.03) | (1.52) | 0.0218 |
| Connective tissue disorder | 0.49 | (0.16) | (1.51) | 0.2133 |
| Peptic ulcer | 1.29 | (1.11) | (1.50) | 0.0009 |
| Liver cirrhosis | 0.78 | (0.67) | (0.92) | 0.0025 |
| Diabetes | 1.17 | (0.92) | (1.50) | 0.2098 |
| Diabetes complications | 1.21 | (0.85) | (1.72) | 0.2872 |
| Paraplegia | 0.75 | (0.31) | (1.79) | 0.5116 |
| Renal disease | 1.87 | (1.42) | (2.48) | <0.0001 |
| Severe liver disease | 1.61 | (0.22) | (11.63) | 0.6392 |
| Hypertension | 1.06 | (0.89) | (1.27) | 0.5056 |
| Baseline Medications | ||||
| Metformin | 1.16 | (0.87) | (1.55) | 0.3157 |
| Aspirin | 0.84 | (0.65) | (1.09) | 0.1964 |
| Angiotensin converting-enzyme inhibitor | 0.71 | (0.52) | (0.97) | 0.0307 |
| Lipid lowering drugs | 0.80 | (0.48) | (1.32) | 0.3820 |
| Statins | 0.91 | (0.40) | (2.04) | 0.8147 |
| Diuretics | 1.88 | (1.45) | (2.44) | <0.0001 |
| Selective beta blockers | 0.94 | (0.70) | (1.26) | 0.6631 |
| Concomitant Medications | ||||
| Selective beta blockers | 0.44 | (0.35) | (0.56) | <0.0001 |
| Diuretics | 2.69 | (2.33) | (3.11) | <0.0001 |
| Variable | Adjusted HR | 95% CI | p-Value | ||
|---|---|---|---|---|---|
| Propranolol Exposure | |||||
| 1~28 Days vs. non-exposure | 0.81 | (0.65) | (1.01) | 0.0580 | |
| 29~90 Days vs. non-exposure | 0.80 | (0.58) | (1.09) | 0.1588 | |
| >90 Days vs. non-exposure | 0.49 | (0.36) | (0.67) | <0.0001 | |
| Sex | |||||
| Male vs. female | 1.47 | (1.20) | (1.79) | 0.0002 | |
| Age Group | |||||
| 18–34 | |||||
| 35–49 | 3.33 | (2.02) | (5.49) | <0.0001 | |
| 50–64 | 7.67 | (4.68) | (12.55) | <0.0001 | |
| 65+ | 10.72 | (6.43) | (17.88) | <0.0001 | |
| Covariate | |||||
| CCI | |||||
| 1 | Acute myocardial infarction | 1.82 | (0.25) | (13.18) | 0.5552 |
| 2 | Congestive heart failure | 0.98 | (0.45) | (2.10) | 0.9489 |
| 3 | Peripheral vascular disease | 0.74 | (0.10) | (5.26) | 0.7597 |
| 4 | Cerebral vascular accident | 0.78 | (0.46) | (1.33) | 0.3695 |
| 6 | Pulmonary disease | 0.79 | (0.57) | (1.10) | 0.1584 |
| 7 | Connective tissue disorder | 0.64 | (0.16) | (2.58) | 0.5294 |
| 8 | Peptic ulcer | 1.03 | (0.82) | (1.30) | 0.7978 |
| 9 | Liver cirrhosis | 1.46 | (1.19) | (1.78) | 0.0002 |
| 10 | Diabetes | 0.75 | (0.51) | (1.10) | 0.1362 |
| 11 | Diabetes complications | 1.10 | (0.62) | (1.96) | 0.7375 |
| 12 | Renal disease | 0.90 | (0.47) | (1.71) | 0.7458 |
| 13 | Hypertension | 0.49 | (0.37) | (0.66) | <0.0001 |
| Baseline Medications | |||||
| Metformin | 2.08 | (1.40) | (3.08) | 0.0003 | |
| Aspirin | 0.71 | (0.46) | (1.11) | 0.1355 | |
| Angiotensin converting-enzyme inhibitor | 1.23 | (0.80) | (1.90) | 0.3513 | |
| Lipid lowering drugs | 0.50 | (0.20) | (1.21) | 0.1248 | |
| Statins | 1.30 | (0.41) | (4.09) | 0.6527 | |
| Diuretics | 0.74 | (0.44) | (1.24) | 0.2547 | |
| Selective beta blockers | 1.21 | (0.78) | (1.87) | 0.3858 | |
| Concomitant Medications | |||||
| Selective beta blockers | 0.54 | (0.39) | (0.74) | 0.0001 | |
| Diuretics | 5.65 | (4.61) | (6.92) | <0.0001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, W.-S.; Yang, S.-C.; Liang, C.-M.; Li, Y.-C.; Tai, W.-C.; Lee, C.-H.; Yang, Y.-H.; Hsu, C.-N.; Tsai, T.-H.; Chuah, S.-K.; et al. The Role of Non-Selective β-Blockers in Compensated Cirrhotic Patients without Major Complications. Medicina 2020, 56, 14. https://doi.org/10.3390/medicina56010014
Yeh W-S, Yang S-C, Liang C-M, Li Y-C, Tai W-C, Lee C-H, Yang Y-H, Hsu C-N, Tsai T-H, Chuah S-K, et al. The Role of Non-Selective β-Blockers in Compensated Cirrhotic Patients without Major Complications. Medicina. 2020; 56(1):14. https://doi.org/10.3390/medicina56010014
Chicago/Turabian StyleYeh, Wen-Shuo, Shih-Cheng Yang, Chih-Ming Liang, Yu-Chi Li, Wei-Chen Tai, Chen-Hsiang Lee, Yao-Hsu Yang, Chien-Ning Hsu, Tzu-Hsien Tsai, Seng-Kee Chuah, and et al. 2020. "The Role of Non-Selective β-Blockers in Compensated Cirrhotic Patients without Major Complications" Medicina 56, no. 1: 14. https://doi.org/10.3390/medicina56010014