Pharmacotherapy Literacy of Parents in the Rural and Urban Areas of Serbia—Are There Any Differences?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
3.1. Socio-Demographic and Health-Related Characteristics of Respondents
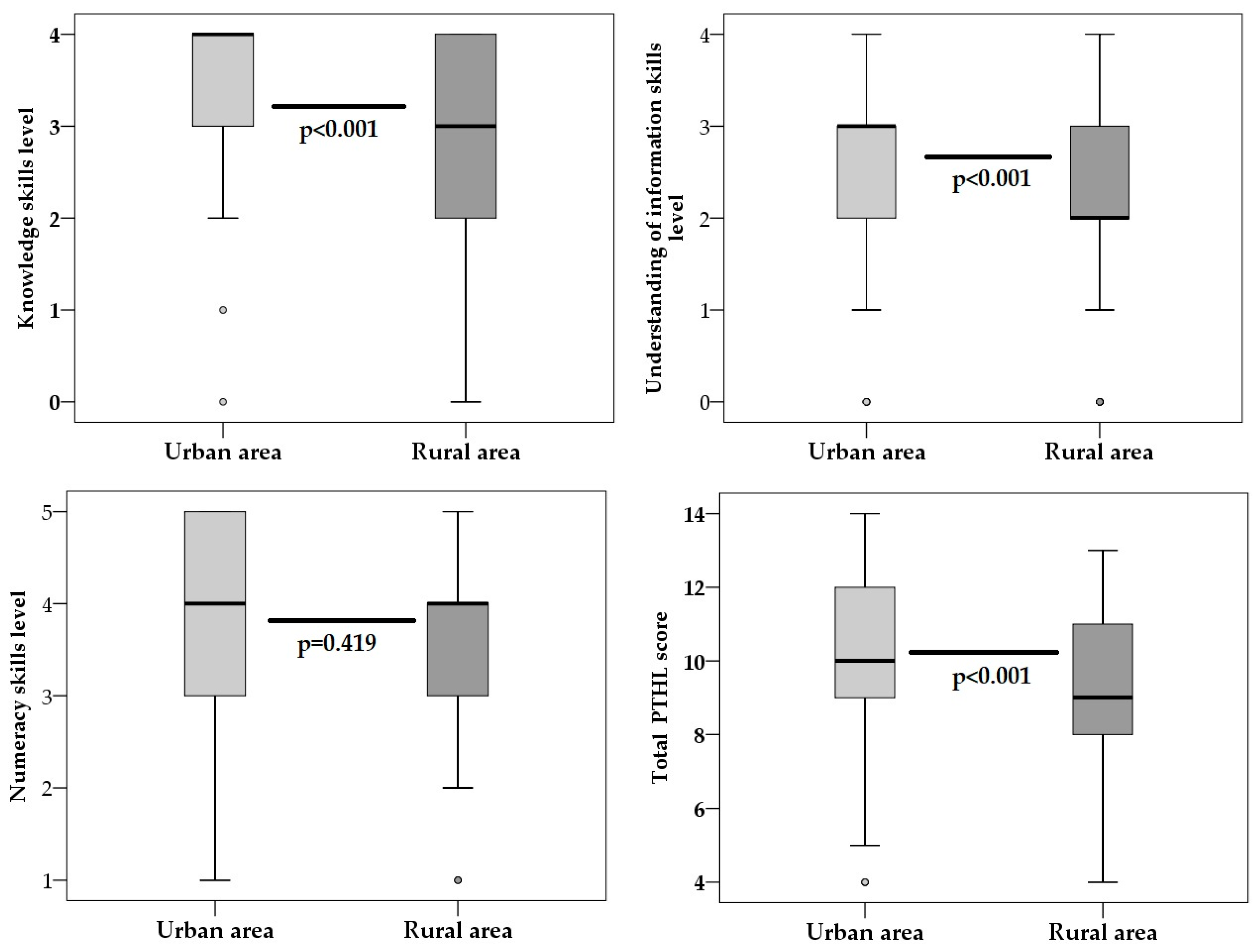
3.2. Pharmacotherapy Literacy of Respondents
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Haun, J.N.; Valerio, M.A.; McCormack, L.A.; Sørensen, K.; Paasche-Orlow, M.K. Health literacy measurement: An inventory and descriptive summary of 51 instruments. J. Health Commun. 2014, 19, 302–330. [Google Scholar] [CrossRef] [PubMed]
- Parker, R. Health literacy: A challenge for American patients and their health care providers. Health Promot. Int. 2000, 15, 277–283. [Google Scholar] [CrossRef]
- World Health Organization. Shanghai declaration on promoting health in the 2030 Agenda for Sustainable Development. Health Promot. Int. 2017, 32, 7. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Todorovic, N.; Jovic-Vranes, A.; Djikanovic, B.; Pilipovic-Broceta, N.; Vasiljevic, N.; Lucic-Samardzija, V.; Peric, A. Assessment of health literacy in the adult population registered to family medicine physicians in the Republic of Srpska, Bosnia and Herzegovina. Eur. J. Gen. Pract. 2019, 25, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.S.; Johnson, M.; Mendelsohn, A.L.; Abrams, M.A.; Sanders, L.M.; Dreyer, B.P. The health literacy of parents in the United States: A nationally representative study. Pediatrics 2009, 124 (Suppl. 3), 289–298. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.W.; Miller, M.J.; Schmitt, M.R.; Wen, F.K. Assessing readability formula differences with written health information materials: Application, results, and recommendations. Res. Soc. Adm. Pharm. 2013, 9, 503–516. [Google Scholar] [CrossRef] [PubMed]
- Krajnović, D.; Ubavić, S.; Bogavac-Stanojević, N. Pharmacotherapy literacy and parental practice in use of over-the-counter pediatric medicines. Medicina 2019, 55, 80. [Google Scholar] [CrossRef]
- Raynor, D.K. Addressing medication literacy: A pharmacy practice priority. Int. J. Pharm. Pract. 2009, 17, 257–259. [Google Scholar] [CrossRef]
- Pouliot, A.; Vaillancourt, R.; Stacey, D.; Suter, P. Defining and identifying concepts of medication literacy: An international perspective. Res. Soc. Adm. Pharm. 2018, 14, 797–804. [Google Scholar] [CrossRef]
- Pouliot, A.; Vaillancourt, R. Medication Literacy: Why Pharmacists Should Pay Attention. Can. J. Hosp. Pharm. 2016, 69, 335–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, S.R.; Mccaffrey, D.J., III; Bouldin, A.S. Health literacy in the pharmacy setting: Defining pharmacotherapy literacy. Pharm. Pract. 2011, 9, 213–220. [Google Scholar] [CrossRef]
- Ubavić, S.; Bogavac-Stanojević, N.; Jović-Vraneš, A.; Krajnović, D. Understanding of information about medicines use among parents of pre-school children in Serbia: Parental pharmacotherapy literacy questionnaire (PTHL-SR). Int. J. Environ. Res. Public Health 2018, 15, 977. [Google Scholar] [CrossRef] [PubMed]
- Dewalt, D.A.; Hink, A. Health literacy and child health outcomes: A systematic review of the literature. Pediatrics 2009, 124 (Suppl. 3), S265–S274. [Google Scholar] [CrossRef] [PubMed]
- Zahnd, W.E.; Scaife, S.L.; Francis, M.L. Health literacy skills in rural and urban populations. Am. J. Health Behav. 2009, 33, 550–557. [Google Scholar] [CrossRef]
- Levin, K.A.; Leyland, A.H. A comparison of health inequalities in urban and rural Scotland. Soc. Sci. Med. 2006, 62, 1457–1464. [Google Scholar] [CrossRef]
- Ogunbodede, E.O.; Kida, I.A.; Madjapa, H.S.; Amedari, M.; Ehizele, A.; Mutave, R.; Sodipo, B.; Temilola, S.; Okoye, L. Oral Health Inequalities between Rural and Urban Populations of the African and Middle East Region. Adv. Dent. Res. 2015, 27, 18–25. [Google Scholar] [CrossRef]
- Nutbeam, D.; Mcgill, B.; Premkumar, P. Improving health literacy in community populations: A review of progress. Health Promot. Int. 2017, 33, 901–911. Available online: https://academic.oup.com/heapro/article-lookup/doi/10.1093/heapro/dax015 (accessed on 17 June 2019). [CrossRef]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31 (Suppl. 1), S19–S26. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17931132 (accessed on 17 June 2019). [CrossRef]
- Mancuso, J.M. Health literacy: A concept/dimensional analysis. Nur. Health Sci. 2008, 10, 248–255. [Google Scholar] [CrossRef]
- Caldwell, B.K.; Caldwell, J.C.; Barkat-e-Khuda; Pieris, I. Why do the children of the poor die in Dhaka, Bangladesh? Popul. Res. Policy Rev. 2002, 21, 159. [Google Scholar] [CrossRef]
- Lee, S.S.; Choi, Y.S.; Lee, D.S.; Nam, S.H. A study on the health literacy of the elderly in rural area. Biomed. Res. 2017, 28, 7567–7573. [Google Scholar]
- Rushworth, G.F.; Diack, L.; Macrobbie, A.; Munoz, S.A.; Pfleger, S.; Stewart, D. Access to medicines in remote and rural areas: A survey of residents in the Scottish Highlands & Western Isles. Public Health 2015, 129, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Pop, O.M.; Brînzaniuc, A.; Şirlincan, E.O.; Baba, C.O.; Cherecheş, R.M. Assessing health literacy in rural settings: A pilot study in rural areas of Cluj County, Romania. Glob. Health Promot. 2013, 20, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Opare-Addo, M.N.; Buabeng, K.O.; Marfo, A.F.; Osei, F.A.; Owusu-Dabo, E.; Ansong, D.; Anto, B.P.; Boaheng, J.M.; Nyanor, I. Source of medicines and medicine information by self-reported persons living with hypertension and diabetes in rural and Urban Ghana. Pharm. Pract. 2018, 16, 1151. [Google Scholar] [CrossRef] [PubMed]
- Ortega, L.Y.; Arribas, M.J.; Jódar, A.R. Diseño, construcción y evaluación de una escala para medir la actitud hacia la automedicación en adolescentes. Rev. Española De Salud Pública 2018, 92, e201807042. [Google Scholar]
- Gavrilovic, D. Statistical Yearbook of The Republic of Serbia; Statistical Office of the Republic of Serbia: Belgrade, Serbia, 2018; p. 53.
- World Data Bank, United Nations Population Division. World Urbanization Prospects: 2018 Revision. Available online: https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS?name_desc=false (accessed on 28 July 2019).
- Ubavic, S.; Krajnovic, D. Pharmacotherapy literacy (PTHL-SR) questionnaire for parents of pre-school children in Serbia: Construction and psychometric characteristics. Vojnosanit Pregl. 2018, in press. [Google Scholar] [CrossRef]
- Cox, K.; Giglia, R.; Binns, C.W. Breastfeeding beyond the big smoke: Who provides support for mothers in rural Western Australia? Aust. J. Rural. Health 2017, 25, 369–375. [Google Scholar] [CrossRef]
- Adewuyi, E.O.; Auta, A.; Khanal, V.; Bamidele, O.D.; Akuoko, C.P.; Adefemi, K.; Tapshak, S.J.; Zhao, Y. Prevalence and factors associated with underutilization of antenatal care services in Nigeria: A comparative study of rural and urban residences based on the 2013 Nigeria demographic and health survey. PLoS ONE 2018, 13, e0197324. [Google Scholar] [CrossRef]
- Li, X.; Ning, N.; Hao, Y.; Sun, H.; Gao, L.; Jiao, M.; Wu, Q.; Quan, H. Health literacy in rural areas of China: Hypertension knowledge survey. Int. J. Environ. Res. Public Health 2013, 10, 1125–1138. [Google Scholar] [CrossRef]
- Bogdanovic, R.; Lozanovic, D.; Pejovic Milovancevic, M.; Sokal Jovanovic, L. The Child Health Care System of Serbia. J. Pediatrics 2016, 177S, S156–S172. [Google Scholar] [CrossRef]
- Ministry of Health of the Republic of Serbia. Results of the National Health Survey of the Republic of Serbia 2013. Ministry of Health of the Republic of Serbia: Belgrade, Serbia, 2014. Available online: http://www.batut.org.rs/download/publikacije/2013SerbiaHealthSurvey.pdf (accessed on 17 June 2019).



{kind=link}
{kind=link}
| Socio-Demographic Characteristics | Urban n = 250 n (%) | Rural n = 182 n (%) | Statistics n = 432 | |
|---|---|---|---|---|
| Gender | Female | 207 (82.8) | 145 (79.7) | X2(1, n = 432) = 0.68 p = 0.408 |
| Male | 43 (17.2) | 37 (20.3) | ||
| Age (years) | 18–29 | 13 (5.2) | 45 (24.7) | X2(2, n = 432) = 38.4 p < 0.001 |
| 30–40 | 184 (73.6) | 118 (64.8) | ||
| 41–50 | 53 (21.2) | 19 (10.4) | ||
| Number of children | One child | 64 (25.6) | 56 (30.8) | X2(2, n = 432) = 1.87 p = 0.392 |
| Two children | 154 (61.6) | 108 (59.8) | ||
| Three children and more | 32 (12.8) | 18 (9.9) | ||
| Marital status | Living with a partner | 232 (92.8) | 173 (95.1) | X2(1, n = 432) = 0.92 p = 0.339 |
| Living without a partner | 18 (7.2) | 9 (4.9) | ||
| Education | University degree and higher | 167 (66.8) | 55 (30.2) | X2(1, n = 432) = 56.4 p < 0.001 |
| No university degree | 83 (33.2) | 127 (69.8) | ||
| Employment | Employed | 230 (92.0) | 138 (75.8) | X2(1, n = 432) = 21.8 p < 0.001 |
| Not employed | 20 (8.0) | 44 (24.2) | ||
| Smoking | Yes | 65 (26.0) | 61 (33.5) | X2(1, n = 432) = 2.88 p = 0.090 |
| No | 185 (74.0) | 121 (66.5) | ||
| Health-Related Characteristics | Urban n = 250 n (%) | Rural n = 182 n (%) | Statistics n = 432 | |
|---|---|---|---|---|
| Chronic disease of a child | Yes | 32 (12.8) | 26 (14.3) | X2(1, n = 432) = 0.20; p = 0.655 |
| No | 218 (87.2) | 156 (85.7) | ||
| Breastfeeding of a first child | Yes | 225 (90.0) | 143 (78.6) | X2(1, n = 432) = 10.9; p < 0.001 |
| No | 25 (10.0) | 39 (21.4) | ||
| Annual visits to pediatrician | 1–2 times | 83 (33.2) | 72 (39.6) | X2(3, n = 432) = 8.09; p = 0.044 |
| 3–4 times | 75 (30.0) | 63 (34.6) | ||
| 5–6 times 7 times and more | 52 (20.8) | 33 (18.1) | ||
| 40 (16.0) | 14 (7.7) | |||
| Parental estimation of health status | Average | 36 (14.4) | 39 (21.4) | X2(2, n = 432) = 4.42; p = 0.116 |
| Good | 154 (61.6) | 109 (59.9) | ||
| Excellent | 60 (24.0) | 34 (18.7) | ||
| Predictor | β | SE β | Wald X2-Square | Df | p Value | OR | 95% CI |
|---|---|---|---|---|---|---|---|
| Rural area | 1.049 | 0.206 | 25.975 | 1 | < 0.001 | 2.854 | 1.907–4.273 |
| p value | ORa | 95% CI | |||||
| Rural area * | 0.709 | 0.241 | 8.635 | 1 | 0.003 | 2.033 | 1.266–3.262 |
| Goodness of fit test (Hosmer Lemeshow) chi-square = 6.924; df = 8; p = 0.545 | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajnović, D.; Ubavić, S.; Bogavac-Stanojević, N. Pharmacotherapy Literacy of Parents in the Rural and Urban Areas of Serbia—Are There Any Differences? Medicina 2019, 55, 590. https://doi.org/10.3390/medicina55090590
Krajnović D, Ubavić S, Bogavac-Stanojević N. Pharmacotherapy Literacy of Parents in the Rural and Urban Areas of Serbia—Are There Any Differences? Medicina. 2019; 55(9):590. https://doi.org/10.3390/medicina55090590
Chicago/Turabian StyleKrajnović, Dušanka, Stana Ubavić, and Nataša Bogavac-Stanojević. 2019. "Pharmacotherapy Literacy of Parents in the Rural and Urban Areas of Serbia—Are There Any Differences?" Medicina 55, no. 9: 590. https://doi.org/10.3390/medicina55090590