Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine in Rats

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals, Chemicals and Experimental Design
2.2. Plasma Lipid Profile Analysis
2.3. Liver Lipids Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sagoe, D.; Molde, H.; Andreassen, C.S.; Torsheim, T.; Pallesen, S. The global epidemiology of anabolic-androgenic steroid use: A meta-analysis and meta-regression analysis. Ann. Epidemiol. 2014, 24, 383–398. [Google Scholar] [CrossRef]
- van Amsterdam, J.; Opperhuizen, A.; Hartgens, F. Adverse health effects of anabolic-androgenic steroids. Regul. Toxicol. Pharmacol. 2010, 57, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H.; Parisis, C. Doping: A challenge to the endocrinologist. A reappraisal in view of the Olympic Games of 2004. Hormones 2003, 2, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.A.; Oliveira, C.V.; Silva, A.S. Adverse cardiovascular effects from the use of anabolic-androgenic steroids as ergogenic resources. Subst. Use Misuse 2014, 49, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Achar, S.; Rostamian, A.; Narayan, S.M. Cardiac and metabolic effects of anabolic-androgenic steroid abuse on lipids, blood pressure, left ventricular dimensions, and rhythm. Am. J. Cardiol. 2010, 106, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Roşca, A.; Badiu, C.; Uscatescu, V.; Stoian, I.; Mirica, R.; Braga, R.I.; Pavel, B.; Zagrean, L. Effect of chronic administration of anabolic androgenic steroids and taurine on platelet aggregation in rats. Acta Endocrinol. 2013, 9, 33–38. [Google Scholar]
- Roşca, A.; Badiu, C.; Uscatescu, V.; Stoian, I.; Mirica, R.; Braga, R.I.; Pavel, B.; Zagrean, L. Influence of chronic administration of anabolic androgenic steroids and taurine on haemostasis profile in rats: A thrombelastographic study. Blood Coagul. Fibrinolysis 2013, 24, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Vanberg, P.; Atar, D. Androgenic anabolic steroid abuse and the cardiovascular system. Handb. Exp. Pharmacol. 2010, 195, 411–457. [Google Scholar]
- Lambert, I.H.; Kristensen, D.M.; Holm, J.B.; Mortensen, O.H. Physiological role of taurine—From organism to organelle. Acta Physiol. 2015, 213, 191–212. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Guo, J.X.; Chang, P. The effect of taurine on cholesterol metabolism. Mol. Nutr. Food Res. 2012, 56, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S.; Ono, A.; Kawasaki, A.; Takenaga, T. Taurine attenuates the development of hepatic steatosis through the inhibition of oxidative stress in a model of nonalcoholic fatty liver disease in vivo and in vitro. Amino Acids 2018, 50, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Zulli, A. Taurine in cardiovascular disease. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Abebe, W.; Mozaffari, M. Role of taurine in the vasculature: An overview of experimental and human studies. Am. J. Cardiovasc. Dis. 2011, 1, 293–311. [Google Scholar] [PubMed]
- Murakami, S. Taurine and atherosclerosis. Amino Acids 2014, 46, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Roşca, A.E.; Stoian, I.; Badiu, C.; Gaman, L.; Popescu, B.O.; Iosif, L.; Mirica, R.; Tivig, I.C.; Stancu, C.D.; Caruntu, C.; et al. Impact of chronic administration of anabolic androgenic steroids and taurine on blood pressure in rats. Braz. J. Med. Biol. Res. 2016, 49, 5116. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, S.W.; Ito, T. Clinical significance of taurine. Amino Acids 2014, 46, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Woodiwiss, A.J.; Trifunovic, B.; Philippides, M. Effects of an androgenic steroid on exercise-induced cardiac remodeling in rats. Appl. Physiol. 1985, 88, 409–415. [Google Scholar] [CrossRef]
- Ray, K.K.; Kastelein, J.J.; Boekholdt, S.M.; Nicholls, S.J.; Khaw, K.T.; Ballantyne, C.M.; Catapano, A.L.; Reiner, Ž.; Lüscher, T.F. The ACC/AHA 2013 guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular disease risk in adults: The good the bad and the uncertain: A comparison with ESC/EAS guidelines for the management of dyslipidaemias 2011. Eur. Heart J. 2014, 35, 960–968. [Google Scholar] [CrossRef]
- Becker, K.L. Principles and Practice of Endocrinology and Metabolism, 3rd ed.; Lippincot Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Wild, R.A.; Applebaum-Bowden, D.; Demers, L.M.; Bartholomew, M.; Landis, J.R.; Hazzard, W.R.; Santen, R.J. Lipoprotein lipids in women with androgen excess: Independent associations with increased insulin and androgen. Clin. Chem. 1990, 36, 283–289. [Google Scholar]
- Kousta, E.; Tolis, G.; Franks, S. Polycystic ovary syndrome. Revised diagnostic criteria and long-term health consequences. Hormones 2005, 4, 133–147. [Google Scholar] [CrossRef] [Green Version]
- Sattler, F.R.; Schroeder, E.T.; Dube, M.P.; Jaque, S.V.; Martinez, C.; Blanche, P.J.; Azen, S.; Krauss, R.M. Metabolic effects of nandrolone decanoate and resistance training in men with HIV. Am. J. Physiol. Endocrinol. Metab. 2002, 283, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Ghorbanihaghjo, A.; Argani, H.; Rohbaninoubar, M.; Rashtchizadeh, N. Effect of Nandrolone Decanoate on serum lipoprotein (a) and its isoforms in hemodialysis patients. Lipids Health Dis. 2004, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R., Jr.; Mebane, I.L.; Bangdiwala, S.I.; Criqui, M.H.; Tyroler, H.A. High density lipoprotein cholesterol as a predictor of cardiovascular disease mortality in men and women: The follow-up study of the Lipid Research Clinics Prevalence Study. Am. J. Epidemiol. 1990, 131, 32–47. [Google Scholar] [CrossRef] [PubMed]
- Oschry, Y.; Eisenberg, S. Rat plasma lipoproteins: Re-evaluation of a lipoprotein system in an animal devoid of cholesteryl ester transfer activity. J. Lipid Res. 1982, 23, 1099–1106. [Google Scholar] [PubMed]
- Glazer, G. Atherogenic effects of anabolic steroids on serum lipid levels. A literature review. Arch. Intern. Med. 1991, 151, 1925–1933. [Google Scholar] [CrossRef] [PubMed]
- Király, C.L. Androgenic-anabolic steroid effects on serum and skin surface lipids, on red cells, and on liver enzymes. Int. J. Sport Med. 1988, 9, 249–252. [Google Scholar] [CrossRef]
- Kuipers, H.; Wijnen, J.A.; Hartgens, F.; Willems, S.M. Influence of anabolic steroids on body composition, blood pressure, lipid profile and liver functions in body builders. Int. J. Sport Med. 1991, 12, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Glazer, G.; Suchman, A.L. Lack of demonstrated effect of nandrolone on serum lipids. Metabolism 1994, 43, 204–210. [Google Scholar] [CrossRef]
- Hartgens, F.; Rietjens, G.; Keizer, H.A.; Kuipers, H.; Wolffenbuttel, B.H. Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein. Br. J. Sport Med. 2004, 38, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Cunha, T.S.; Moura, M.J.; Bernardes, C.F.; Tanno, A.P.; Marcondes, F.K. Vascular sensitivity to phenylephrine in rats submitted to anaerobic training and nandrolone treatment. Hypertension 2005, 46, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Vieira, R.P.; França, R.F.; Damaceno-Rodrigues, N.R.; Dolhnikoff, M.; Caldini, E.G.; Carvalho, C.R.; Ribeiro, W. Dose-dependent hepatic response to subchronic administration of nandrolone decanoate. Med. Sci. Sport Exerc. 2008, 40, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, M.; Encabo, A.; Marín, J.; Balfagón, G. Chronic treatment with the anabolic steroid, nandrolone, inhibits vasodilator responses in rabbit aorta. Eur. J. Pharmacol. 1994, 252, 233–241. [Google Scholar] [CrossRef]
- Samieinasab, M.R.; Shahraki, M.R.; Samieinasab, F.; Najafi, S. Influence of nandrolone decanoate administration on serum lipids and liver enzymes in rats. ARYA Atheroscler. 2015, 11, 256–260. [Google Scholar] [PubMed]
- Aparicio, V.A.; Sánchez, C.; Ortega, F.B.; Nebot, E.; Kapravelou, G.; Porres, J.M.; Aranda, P. Effects of the dietary amount and source of protein, resistance training and anabolic-androgenic steroids on body weight and lipid profile of rats. Nutr. Hosp. 2013, 28, 127–136. [Google Scholar] [PubMed]
- Schwingel, P.A.; Cotrim, H.P.; Salles, B.R.; Almeida, C.E.; dos Santos, C.R., Jr.; Nachef, B.; Andrade, A.R.; Zoppi, C.C. Anabolic-androgenic steroids: A possible new risk factor of toxicant-associated fatty liver disease. Liver Int. 2011, 31, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Gentile, C.L.; Nivala, A.M.; Gonzales, J.C.; Pfaffenbach, K.T.; Wang, D.; Wei, Y.; Jiang, H.; Orlicky, D.J.; Petersen, D.R.; Pagliassotti, M.J.; et al. Experimental evidence for therapeutic potential of taurine in the treatment of nonalcoholic fatty liver disease. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 301, 1710–1722. [Google Scholar] [CrossRef] [PubMed]
- El Mesallamy, H.O.; El-Demerdash, E.; Hammad, L.N.; El Magdoub, H.M. Effect of taurine supplementation on hyperhomocysteinemia and markers of oxidative stress in high fructose diet induced insulin resistance. Diabetol. Metab. Syndr. 2010, 2, 46. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.J.; Kim, M.J.; Chang, K.J. The effect of dietary taurine supplementation on plasma and liver lipid concentrations and mineral metabolism in rats fed alcohol. Adv. Exp. Med. Biol. 2006, 583, 243–250. [Google Scholar] [PubMed]
- Das, J.; Roy, A.; Sil, P.C. Mechanism of the protective action of taurine in toxin and drug induced organ pathophysiology and diabetic complications: A review. Food Funct. 2012, 3, 1251–1264. [Google Scholar] [CrossRef]
- Park, T.; Lee, K. Dietary taurine supplementation reduces plasma and liver cholesterol and triglyceride levels in rats fed a high-cholesterol or a cholesterol-free diet. Adv. Exp. Med. Biol. 1998, 442, 319–325. [Google Scholar] [PubMed]
- Zhang, M.; Bi, L.F.; Fang, J.H.; Su, X.L.; Da, G.L.; Kuwamori, T.; Kagamimori, S. Beneficial effects of taurine on serum lipids in overweight or obese non-diabetic subjects. Amino Acids 2004, 26, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.W.; Chen, Y.X.; Shi, J.; Lin, Y.; Xie, W.F. The restorative effect of taurine on experimental nonalcoholic steatohepatitis. Dig. Dis. Sci. 2006, 51, 2225–2234. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S.; Kondo-Ohta, Y.; Tomisawa, K. Improvement in cholesterol metabolism in mice given chronic treatment of taurine and fed a high-fat diet. Life Sci. 1999, 64, 83–91. [Google Scholar] [CrossRef]
- Sessa, F.; Salerno, M.; Di Mizio, G.; Bertozzi, G.; Messina, G.; Tomaiuolo, B.; Pisanelli, D.; Maglietta, F.; Ricci, P.; Pomara, C. Anabolic Androgenic Steroids: Searching New Molecular Biomarkers. Front. Pharmacol. 2018, 9, 1321. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | C group | A Group | T Group | AT Group | p ANOVA |
|---|---|---|---|---|---|
| TG (mg/dL) | 56.33 ± 10.74 | 85.15 ± 21.44 | 63.22 ± 12.0 | 60.24 ± 23.26 | 0.01 |
| TC (mg/dL) | 58.83 ± 5.50 | 57.54 ± 8.46 | 60.44 ± 8.23 | 58.33 ± 10.51 | 0.91 |
| LDL-C (mg/dL) | 20.04 ± 3.49 | 20.67 ± 2.90 | 23.53 ± 3.06 | 21.10 ± 2.11 | 0.11 |
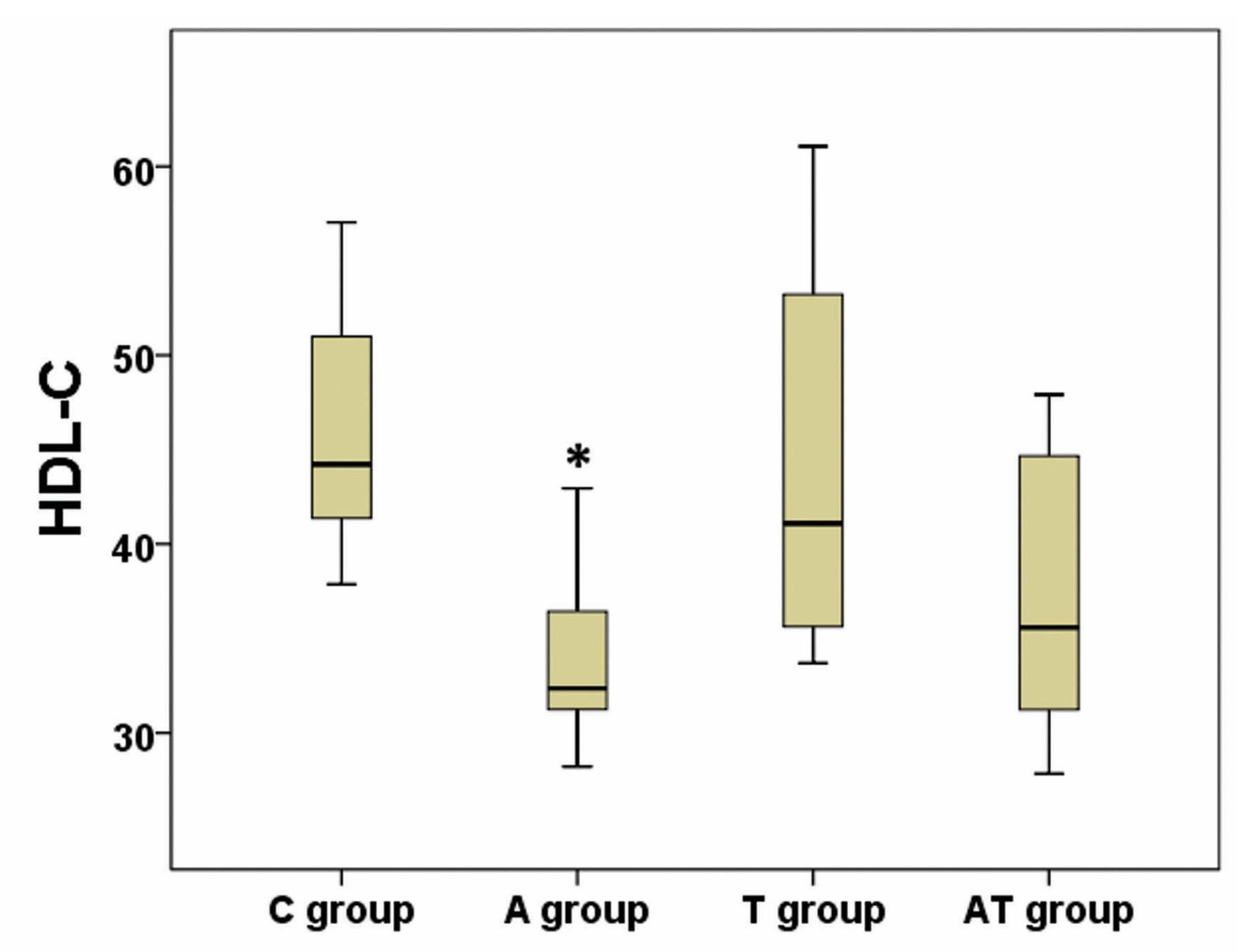
| HDL-C (mg/dL) | 46.00 ± 6.64 | 33.90 ± 4.67 | 44.33 ± 10.69 | 37.33 ± 7.68 | 0.01 |
| TGh (µg/mg protein) | 657.022 ± 102.45 | 536.61 ± 23.33 | 506.50 ± 111.09 | 470.04 ± 43.48 | p < 0.001 |
| NEFA (µmol/mg protein) | 11.05 ± 2.35 | 15.66 ± 7.27 | 13.78 ± 4.01 | 10.19 ± 1.17 | 0.06 |
| LW/BW (g/g) | 0.036 ± 0.003 | 0.038 ± 0.002 | 0.037 ± 0.002 | 0.036 ± 0.002 | 0.21 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosca, A.E.; Stancu, C.S.; Badiu, C.; Popescu, B.O.; Mirica, R.; Căruntu, C.; Gologan, S.; Voiculescu, S.E.; Zagrean, A.-M. Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine in Rats. Medicina 2019, 55, 540. https://doi.org/10.3390/medicina55090540
Rosca AE, Stancu CS, Badiu C, Popescu BO, Mirica R, Căruntu C, Gologan S, Voiculescu SE, Zagrean A-M. Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine in Rats. Medicina. 2019; 55(9):540. https://doi.org/10.3390/medicina55090540
Chicago/Turabian StyleRosca, A.E., Camelia Sorina Stancu, Corin Badiu, Bogdan Ovidiu Popescu, Radu Mirica, Constantin Căruntu, Serban Gologan, Suzana Elena Voiculescu, and Ana-Maria Zagrean. 2019. "Lipid Profile Changes Induced by Chronic Administration of Anabolic Androgenic Steroids and Taurine in Rats" Medicina 55, no. 9: 540. https://doi.org/10.3390/medicina55090540