Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection and Testing
2.2. CMR Measurements
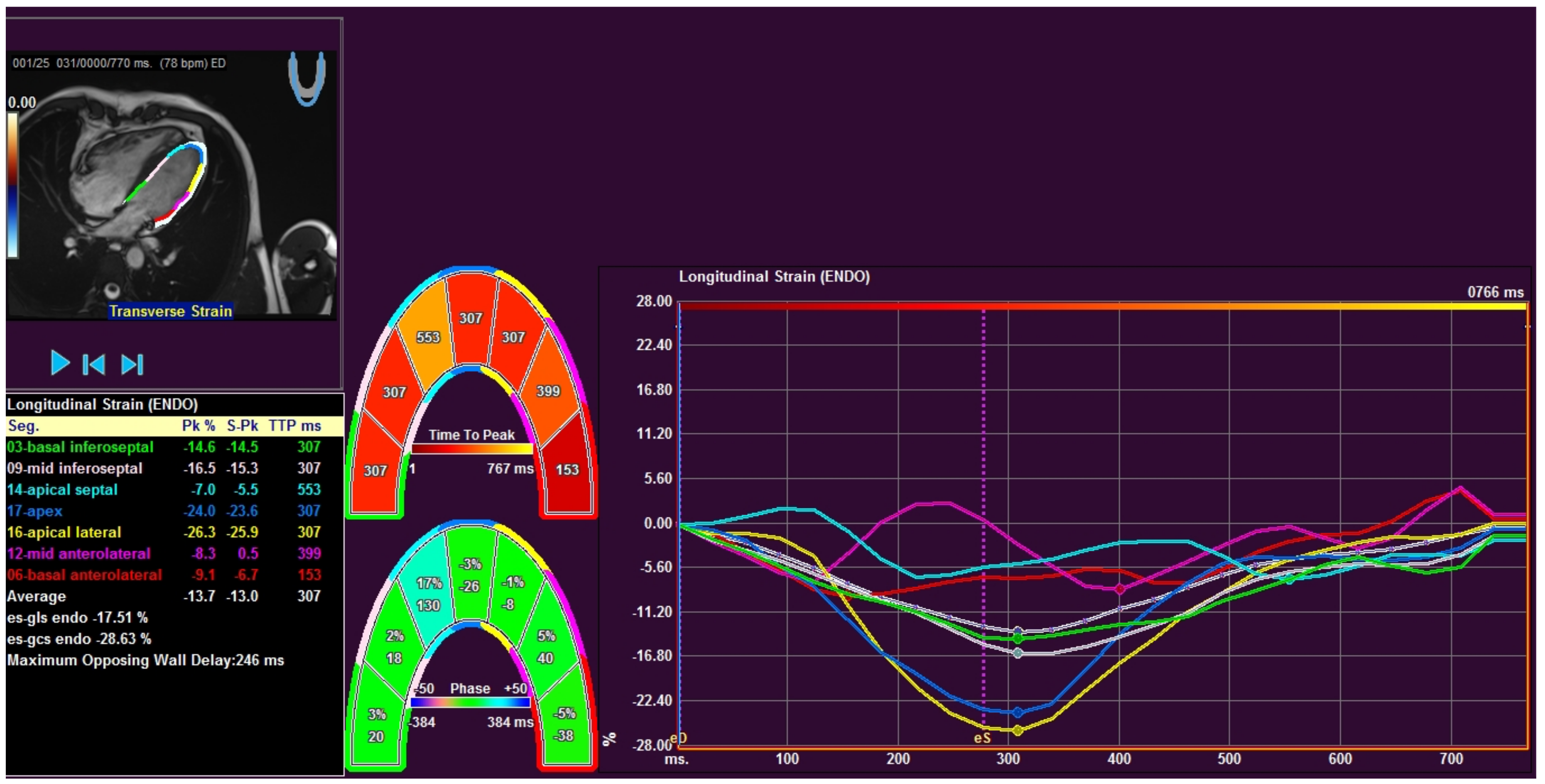
2.3. FT Analysis
2.4. Data Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Galié, N.; Humbert, M.; Vachiéry, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef]
- Swift, A.J.; Rajaram, S.; Campbell, M.J.; Hurdman, J.; Thomas, S.; Capener, D.; Elliot, C.; Condliffe, R.; Wild, J.M.; Kiely, D.G. Prognostic value of cardiovascular magnetic resonance imaging measurements corrected for age and sex in idiopathic pulmonary arterial hypertension. Circ. Cardiovasc. Imaging 2014, 7, 100–106. [Google Scholar] [CrossRef]
- Wolferen, S.A.; Marcus, J.T.; Boonstra, A.; Marques, K.M.; Bronzwaer, J.G.; Spreeuwenberg, M.D. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur. Heart J. 2007, 28. [Google Scholar] [CrossRef] [PubMed]
- Van De Veerdonk, M.C.; Kind, T.; Marcus, J.T.; Mauritz, G.-J.; Heymans, M.W.; Bogaard, H.-J.; Boonstra, A.; Marques, K.M.; Westerhof, N.; Vonk-Noordegraaf, A. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J. Am. Coll. Cardiol. 2011, 58, 2511–2519. [Google Scholar] [CrossRef] [PubMed]
- Swift, A.J.; Capener, D.; Johns, C.; Hamilton, N.; Rothman, A.; Elliot, C.; Condliffe, R.; Charalampopoulos, A.; Rajaram, S.; Lawrie, A.; et al. Magnetic resonance imaging in the prognostic evaluation of patients with pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2017, 196, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Gan, C.T.-J.; Lankhaar, J.-W.; Marcus, J.T.; Westerhof, N.; Marques, K.M.; Bronzwaer, J.G.F.; Boonstra, A.; Postmus, P.E.; Vonk-Noordegraaf, A. Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, 1528–1533. [Google Scholar] [CrossRef]
- Knight, D.S.; Steeden, J.A.; Moledina, S.; Jones, A.; Coghlan, J.G.; Muthurangu, V. Left ventricular diastolic dysfunction in pulmonary hypertension predicts functional capacity and clinical worsening: A tissue phase mapping study. J. Cardiovasc. Magn. Reson. 2015, 17, 116. [Google Scholar] [CrossRef] [PubMed]
- Manders, E.; Bogaard, H.J.; Handoko, M.L.; Veerdonk, M.C.; Keogh, A.; Westerhof, N. Contractile dysfunction of left ventricular cardiomyocytes in patients with pulmonary arterial hypertension. J. Am. Coll. Cardiol. 2014, 64, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Hardegree, E.L.; Sachdev, A.; Fenstad, E.R.; Villarraga, H.R.; Frantz, R.P.; McGoon, M.D. Impaired left ventricular mechanics in pulmonary arterial hypertension: Identification of a cohort at high risk. Circ. Heart Fail. 2013, 6, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Marcus, J.T.; Gan, C.T.; Zwanenburg, J.J.; Boonstra, A.; Allaart, C.P.; Gotte, M.J. Interventricular mechanical asynchrony in pulmonary arterial hypertension: Left-to-right delay in peak shortening is related to right ventricular overload and left ventricular underfilling. J. Am. Coll. Cardiol. 2008, 51, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Marcus, J.T.; Noordegraaf, A.V.; Roeleveld, R.J.; Postmus, P.E.; Heethaar, R.M.; Van Rossum, A.C.; Boonstra, A. Impaired left ventricular filling due to right ventricular pressure overload in primary pulmonary hypertension. Chest 2001, 119, 1761–1765. [Google Scholar] [CrossRef]
- Leitman, M.; Lysyansky, P.; Sidenko, S.; Shir, V.; Peleg, E.; Binenbaum, M.; Kaluski, E.; Krakover, R.; Vered, Z. Two-dimensional strain—A novel software for real-time quantitative echocardiographic assessment of myocardial function. J. Am. Soc. Echocardiogr. 2004, 17, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Steadman, C.D.; Khan, J.N.; Horsfield, M.A.; Bekele, S.; Nazir, S.A.; Kanagala, P.; Masca, N.G.; Clarysse, P.; McCann, G.P. Intertechnique agreement and interstudy reproducibility of strain and diastolic strain rate at 1.5 and 3 tesla: A comparison of feature-tracking and tagging in patients with aortic stenosis. J. Magn. Reson. Imaging 2015, 41, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.S.; Broberg, C.S.; Rydman, R.; Diller, G.P.; Li, W.; Dimopoulos, K.; Wort, S.J.; Pennell, D.J.; Gatzoulis, M.A.; Babu-Narayan, S.V. Impaired right, left, or biventricular function and resting oxygen saturation are associated with mortality in eisenmenger syndrome: A clinical and cardiovascular magnetic resonance study. Circ. Cardiovasc. Imaging 2015, 8, e003596. [Google Scholar] [CrossRef]
- Kallianos, K.; Brooks, G.C.; Mukai, K.; De Carvalho, F.S.; Liu, J.; Naeger, D.M.; De Marco, T.; Ordovas, K.G. Cardiac magnetic resonance evaluation of left ventricular myocardial strain in pulmonary hypertension. Acad. Radiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.N.; Singh, A.; Nazir, S.A.; Kanagala, P.; Gershlick, A.H.; McCann, G.P. Comparison of cardiovascular magnetic resonance feature tracking and tagging for the assessment of left ventricular systolic strain in acute myocardial infarction. Eur. J. Radiol. 2015, 84, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Kutty, S.; Rangamani, S.; Venkataraman, J.; Li, L.; Schuster, A.; Fletcher, S.E.; Danford, D.A.; Beerbaum, P. Reduced global longitudinal and radial strain with normal left ventricular ejection fraction late after effective repair of aortic coarctation: A CMR feature tracking study. Int. J. Cardiovasc. Imaging 2013, 29, 141–150. [Google Scholar] [CrossRef]
- Yang, L.T.; Yamashita, E.; Nagata, Y.; Kado, Y.; Oshima, S.; Otsuji, Y.; Takeuchi, M. Prognostic value of biventricular mechanical parameters assessed using cardiac magnetic resonance feature-tracking analysis to predict future cardiac events. J. Magn. Reson. Imaging 2017, 45, 1034–1045. [Google Scholar] [CrossRef] [PubMed]
- Pedrizzetti, G.; Claus, P.; Kilner, P.J.; Nagel, E. Principles of cardiovascular magnetic resonance feature tracking and echocardiographic speckle tracking for informed clinical use. J. Cardiovasc. Magn. Reson. 2016, 18, 51. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.C.W.; Seale, H.; Hamilton-Craig, C.; Morris, N.R.; Strugnell, W. Quantification of biventricular strain and assessment of ventriculo–ventricular interaction in pulmonary arterial hypertension using exercise cardiac magnetic resonance imaging and myocardial feature tracking. J. Magn. Reson. Imaging 2018. [Google Scholar] [CrossRef]
- Vigneault, D.M.; te Riele, A.S.; James, C.A.; Zimmerman, S.L.; Selwaness, M.; Murray, B.; Tichnell, C.; Tee, M.; Noble, J.A.; Calkins, H.; et al. Right ventricular strain by MR quantitatively identifies regional dysfunction in patients with arrhythmogenic right ventricular cardiomyopathy. J. Magn. Reson. Imaging 2016, 43, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Buss, S.J.; Breuninger, K.; Lehrke, S.; Voss, A.; Galuschky, C.; Lossnitzer, D.; Andre, F.; Ehlermann, P.; Franke, J.; Taeger, T.; et al. Assessment of myocardial deformation with Cardiac magnetic resonance strain imaging improves risk stratification in patients with dilated cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Augustine, D.; Lewandowski, A.J.; Lazdam, M.; Rai, A.; Francis, J.; Myerson, S.; Noble, A.; Becher, H.; Neubauer, S.; Petersen, E.S.; et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: Comparison with tagging and relevance of gender. J. Cardiovasc. Magn. Reson. 2013, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maceira, A.M.; Prasad, S.K.; Khan, M.; Pennell, D.J. Normalized left ventricular systolic and diastolic function by steady state free precession cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2006, 8, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Grothues, F.; Moon, J.C.; Bellenger, N.G.; Smith, G.S.; Klein, H.U.; Pennell, D.J. Interstudy reproducibility of right ventricular volumes, function, and mass with cardiovascular magnetic resonance. Am. Heart J. 2004, 147, 218–223. [Google Scholar] [CrossRef]
- Baggen, V.J.M.; Leiner, T.; Post, M.C.; Van Dijk, A.P.; Roos-Hesselink, J.W.; Boersma, E.; Habets, J.; Sieswerda, G.T. Cardiac magnetic resonance findings predicting mortality in patients with pulmonary arterial hypertension: A systematic review and meta-analysis. Eur. Radiol. 2016, 26, 3771–3780. [Google Scholar] [CrossRef] [PubMed]
- Vo, H.Q.; Marwick, T.H.; Negishi, K. MRI-derived myocardial strain measures in normal subjects. JACC Cardiovasc. Imaging 2018, 11, 196–205. [Google Scholar] [CrossRef]
- De Siqueira, M.E.; Pozo, E.; Fernandes, V.R.; Sengupta, P.P.; Modesto, K.; Gupta, S.S.; Barbeito-Caamaño, C.; Narula, J.; Fuster, V.; Caixeta, A.; et al. Characterization and clinical significance of right ventricular mechanics in pulmonary hypertension evaluated with cardiovascular magnetic resonance feature tracking. J. Cardiovasc. Magn. Reson. 2016, 18, 39. [Google Scholar] [CrossRef]
- Nahum, J.; Bensaid, A.; Dussault, C.; Macron, L.; Clémence, D.; Bouhemad, B.; Monin, J.-L.; Rande, J.L.D.; Guéret, P.; Lim, P. Impact of longitudinal myocardial deformation on the prognosis of chronic heart failure patients. Circ. Cardiovasc. Imaging 2010, 3, 249–256. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Non-Survival Group (n = 12) | Survival Group (n = 31) | p Value |
|---|---|---|---|
| Age (years) | 56.0 [43.8–70.8] | 55.0 [44.0–70.0] | 0.840 |
| Women/men (n (%)) | 7 (25)/5 (33.3) | 21 (75)/10 (66.7) | 0.561 * |
| IPAH (n (%)) | 3 (25) | 10 (32.3) | 0.643 * |
| PHSsc (n (%)) | 3 (25) | 5 (16.1) | 0.505 * |
| Eisenmenger syndrome (n (%)) | 4 (33.3) | 9 (29.0) | 0.784 * |
| CTEPH (n (%)) | 2 (16.7) | 7 (22.6) | 0.672 * |
| NYHA class 2/3/4 (n (%)) | 3 (25)/6 (50)/3 (25) | 6 (19.4)/20 (64.5)/5 (16.1) | 0.708 ** |
| mPAP (mmHg) | 56.5 [41.75–64.75] | 54.0 [44.0–72.0] | 0.753 |
| 6MWT (m) | 270 [160.0–406.0] | 313.5 [250.0–380.75] | 0.488 |
| NT-pro BNP (ng/mL) | 2588.0 [1215.5–5521.0] | 763.0 [238.0–2156.0] | 0.022 |
| Parameter | Non-Survival Group (n = 12) | Survival Group (n = 31) | p Value |
|---|---|---|---|
| RVEDVI (mL/m2) | 87.0 [76.0–112.3] | 82.0 [68.0–101.0] | 0.243 |
| RVESVI (mL/m2) | 63.5 [45.8–91.3] | 48.0 [37.0–60.0] | 0.060 |
| RVEF (%) | 37.5 [18.8–41.8] | 42.0 [32.0–47.0] | 0.088 |
| LVEDVI (mL/m2) | 60.5 [48.0–84.5] | 62.0 [53.0–83.0] | 0.862 |
| LVESVI (mL/m2) | 30.0 [20.75–45.25] | 29.0 [18.0–38.0] | 0.621 |
| LVEF (%) | 48.0 [38.8–60.5] | 60.0 [50.0–66.0] | 0.042 |
| RV Free Wall LS (%) | −16.4 [−21.4–(−11.3)] | −18.1 [−22.9–(−13.8)] | 0.243 |
| RV Septum LS (%) | −9.95 [−13.85–(−6.3)] | −12.0 [−14.3–(−6.9)] | 0.621 |
| RV GLS (%) | −12.9 [−17.2–(−9.5)] | −14.1 [−16.9–(−11.0)] | 0.399 |
| LV GLS (%) | −12.4 [−19.0–(−7.8)] | −18.4 [−22.5–(−15.5)] | 0.009 |
| LV GCS (%) | −28.5 [−34.2–(−23.5)] | −32.0 [−36.8–(−28.2)] | 0.221 |
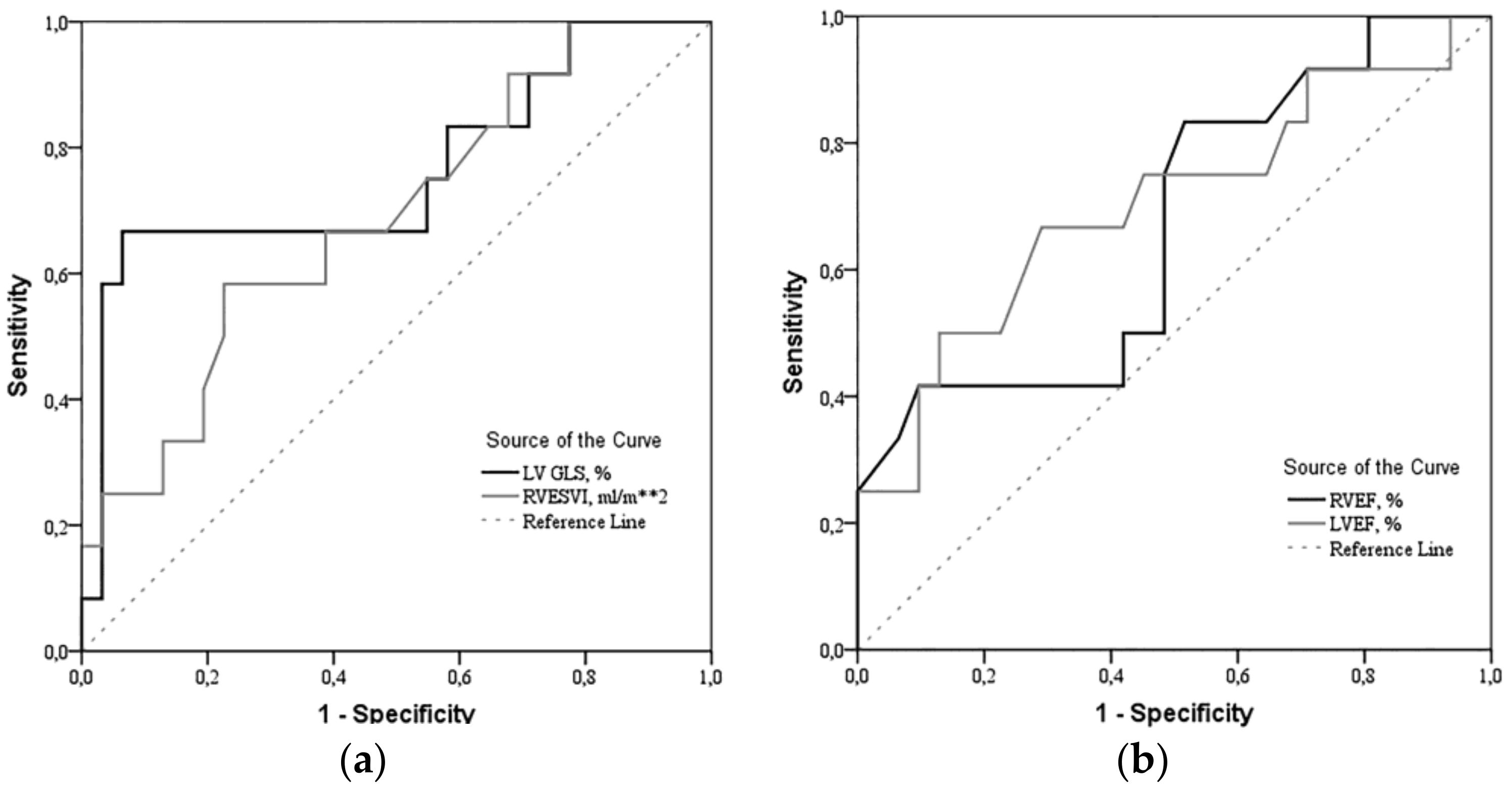
| Parameter | Area under the ROC Curve, % | Sensitivity/Specificity, % | Survival/Non-Survival Group, n (%) | Non-Survival Group OR [95% CI] |
|---|---|---|---|---|
| LV GLS > −14.2% | 76.1 | 77.8/93.5 | 2 (6.5)/8 (66.7) | 20.3 [3.237–127.288] |
| RVESVI > 60 mL/m2 | 68.7 | 58.3/77.4 | 7 (22.6)/7 (58.3) | 4.8 [1.156–19.925] |
| RVEF < 25.5% | 66.9 | 41.7/90.3 | 3 (9.7)/5 (41.7) | 6.667 [1.276–34.842] |
| LVEF < 52% | 70.2 | 66.7/71.0 | 9 (29.0)/8 (66.7) | 4.889 [1.171–20.408] |
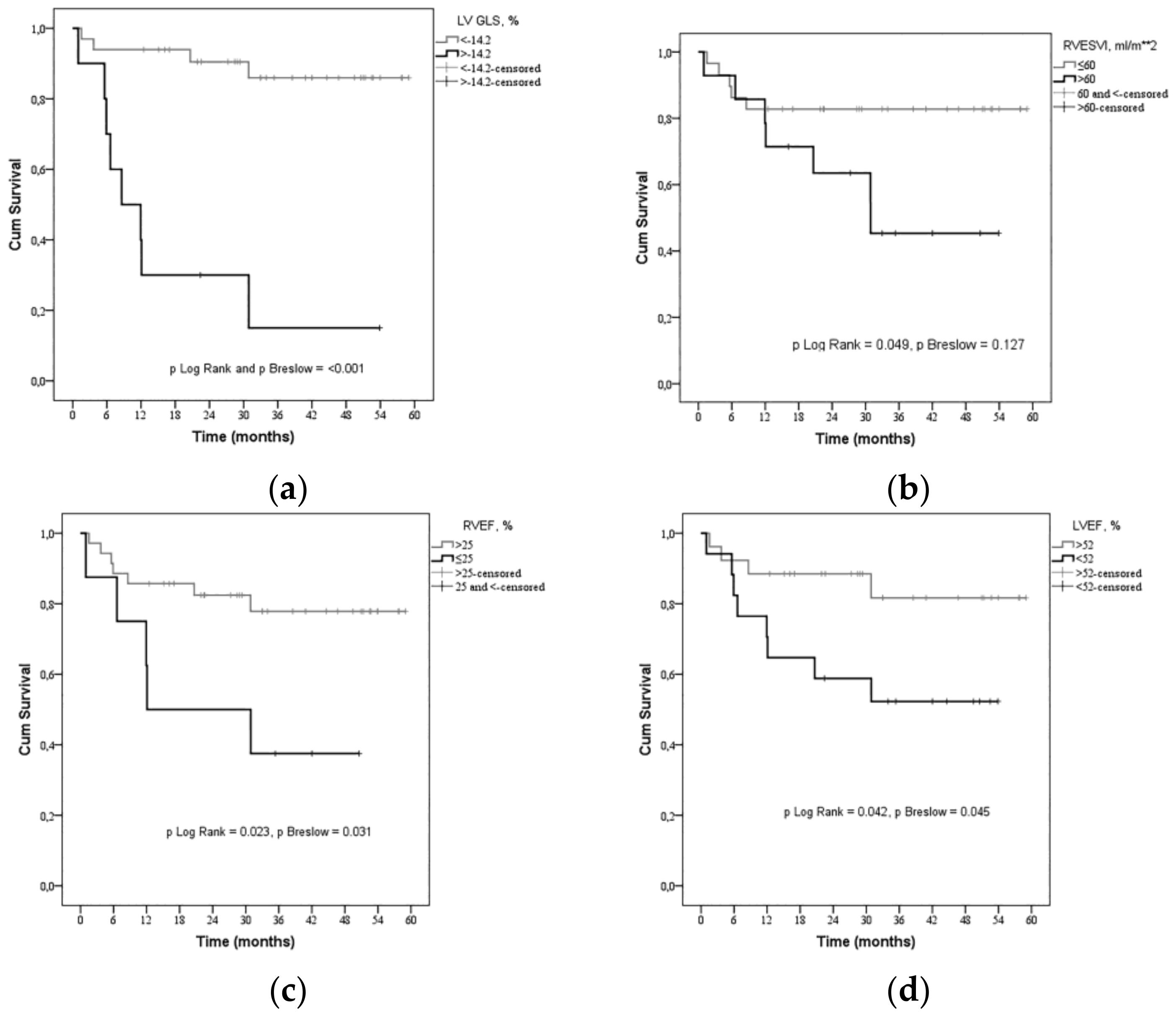
| Parameter | Coefficient Beta | SE | p Value | HR [95% CI] |
|---|---|---|---|---|
| LV GLS > −14.2% | 2.396 | 0.624 | <0.001 | 10.974 [3.229–37.301] |
| RVESVI > 60 mL/m2 | 1.096 | 0.586 | 0.061 | 2.992 [0.949–9.433] |
| RVEF < 25.5% | 1.253 | 0.587 | 0.033 | 3.501 [1.109–11.053] |
| LVEF < 52% | 1.179 | 0.613 | 0.055 | 3.25 [0.977–10.809] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padervinskienė, L.; Krivickienė, A.; Hoppenot, D.; Miliauskas, S.; Basevičius, A.; Nedzelskienė, I.; Jankauskas, A.; Šimkus, P.; Ereminienė, E. Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study. Medicina 2019, 55, 73. https://doi.org/10.3390/medicina55030073
Padervinskienė L, Krivickienė A, Hoppenot D, Miliauskas S, Basevičius A, Nedzelskienė I, Jankauskas A, Šimkus P, Ereminienė E. Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study. Medicina. 2019; 55(3):73. https://doi.org/10.3390/medicina55030073
Chicago/Turabian StylePadervinskienė, Lina, Aušra Krivickienė, Deimantė Hoppenot, Skaidrius Miliauskas, Algidas Basevičius, Irena Nedzelskienė, Antanas Jankauskas, Paulius Šimkus, and Eglė Ereminienė. 2019. "Prognostic Value of Left Ventricular Function and Mechanics in Pulmonary Hypertension: A Pilot Cardiovascular Magnetic Resonance Feature Tracking Study" Medicina 55, no. 3: 73. https://doi.org/10.3390/medicina55030073