Exercise-Associated Hyponatremia During a Self-Paced Marathon Attempt in a 15-Year-Old Male Teenager




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
2.1. Subject and Event
2.2. Measurements
2.3. Data Analysis
3. Results
4. Discussion
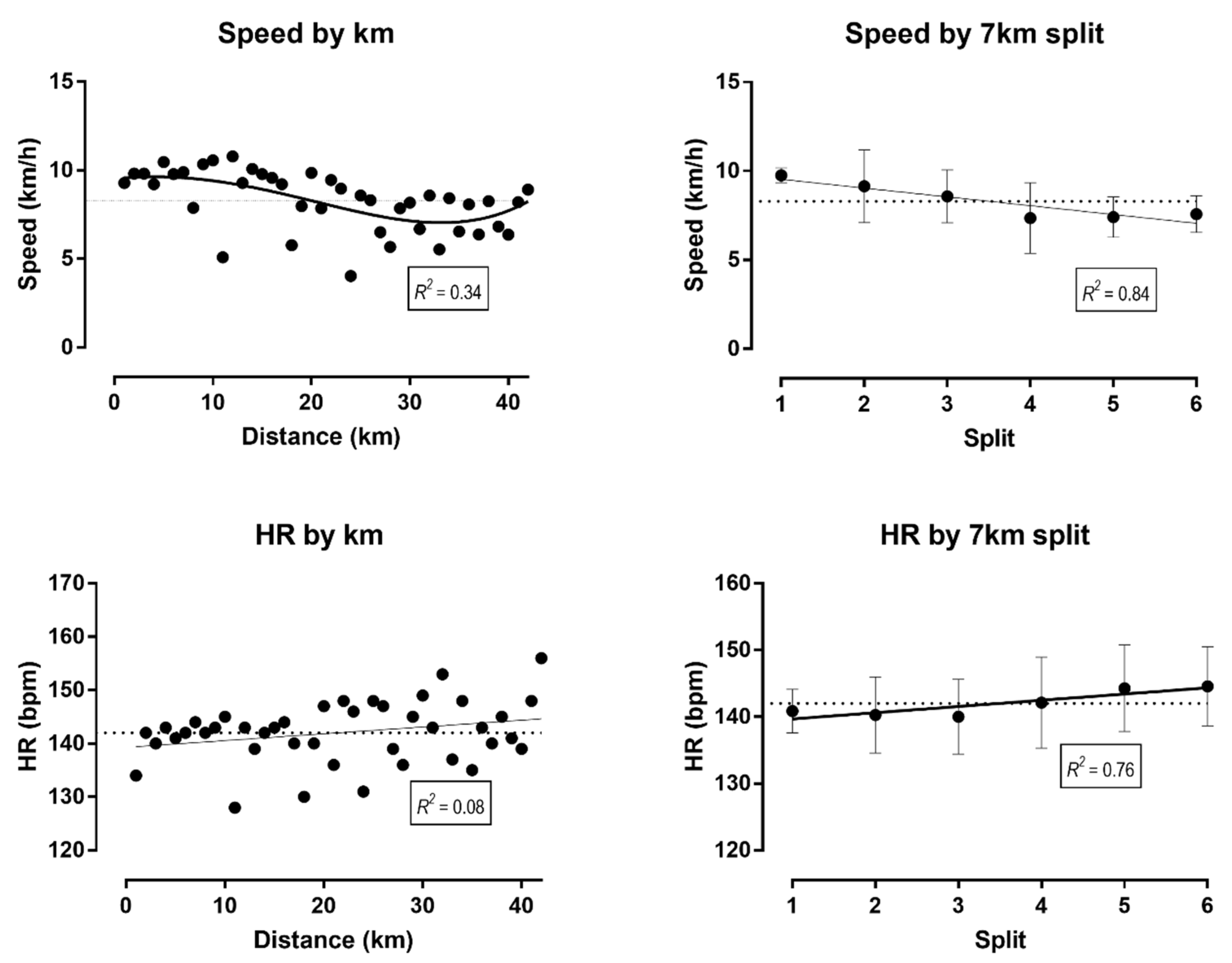
4.1. Positive Pacing with a Final End Spurt
4.2. Exercise-Associated Hyponatremia after the Run
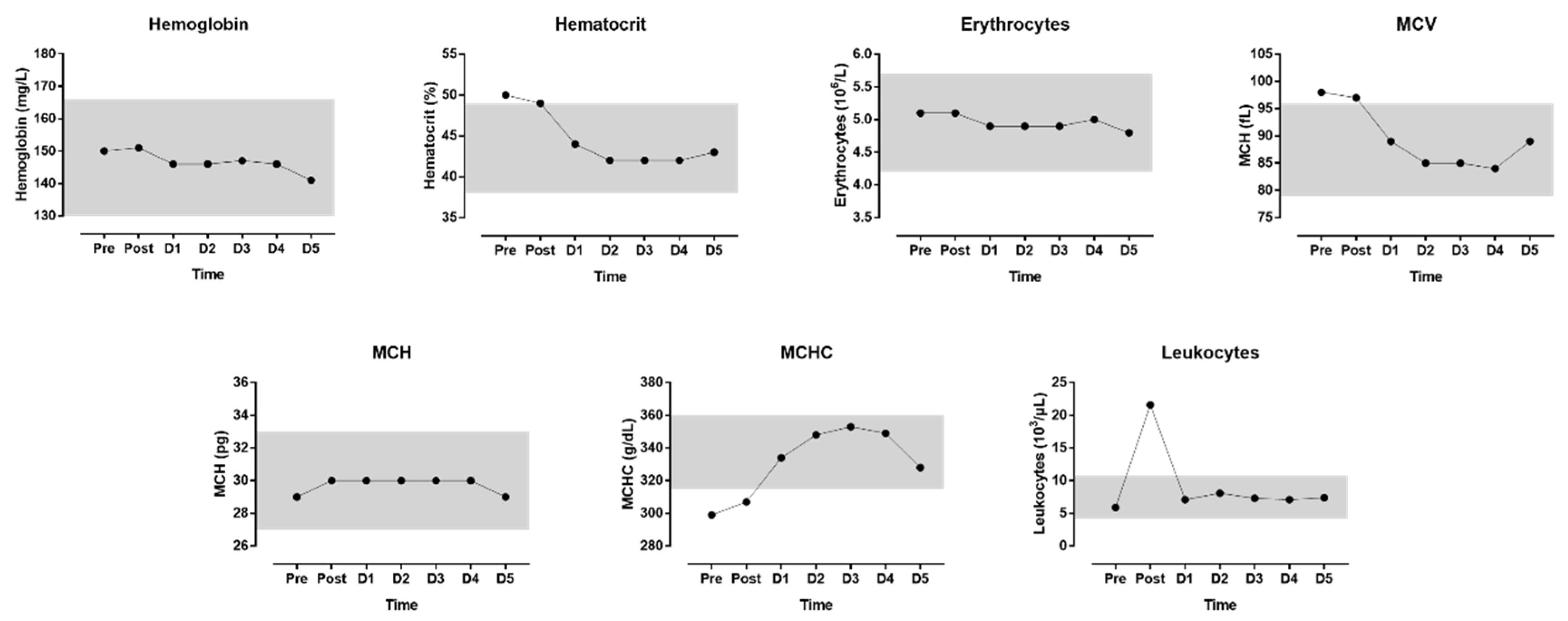
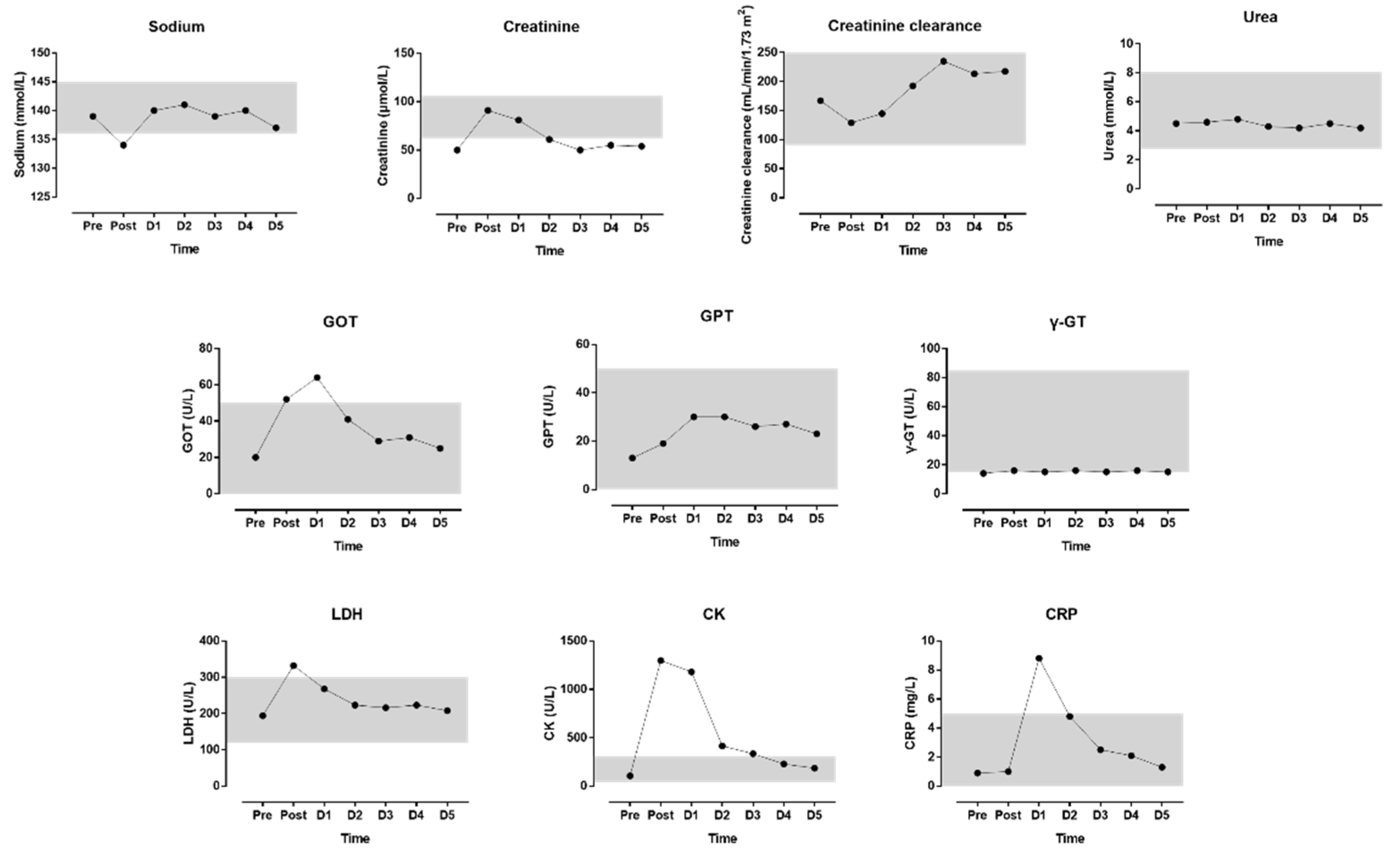
4.3. Changes in Laboratory Values
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Diaz, J.J.; Fernandez-Ozcorta, E.J.; Santos-Concejero, J. The influence of pacing strategy on marathon world records. Eur. J. Sport Sci. 2018, 18, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Santos-Lozano, A.; Collado, P.S.; Foster, C.; Lucia, A.; Garatachea, N. Influence of sex and level on marathon pacing strategy. Insights from the new york city race. Int. J. Sports Med. 2014, 35, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.T.; Knechtle, B. Do fast older runners pace differently from fast younger runners in the ‘New York city marathon’? J. Strength Cond. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.T.; Knechtle, B. Effect of age and performance on pacing of marathon runners. Open Access J. Sports Med. 2017, 8, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.T.; Knechtle, B. Pacing strategies in the ‘Athens classic marathon’: Physiological and psychological aspects. Front. Physiol. 2018, 9, 1539. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.T.; Di Gangi, S.; Knechtle, B. World records in half-marathon running by sex and age. J. Aging Phys. Act. 2018, 26, 629–636. [Google Scholar] [CrossRef]
- Knechtle, B.; Assadi, H.; Lepers, R.; Rosemann, T.; Rust, C.A. Relationship between age and elite marathon race time in world single age records from 5 to 93 years. BMC Sports Sci. Med. Rehabil. 2014, 6, 31. [Google Scholar] [CrossRef]
- Knechtle, B.; Nikolaidis, P.T.; Di Gangi, S. World single age records in running from 5 km to marathon. Front. Psychol. 2018, 9, 2013. [Google Scholar] [CrossRef]
- Knechtle, B.; Knechtle, C.; Rosemann, T.; Nikolaidis, P.T. Pacing of an untrained 17-year-old teenager in a marathon attempt. Int. J. Exerc. Sci. 2018, 11, 856–866. [Google Scholar]
- Roberts, W.O.; Nicholson, W.G. Youth marathon runners and race day medical risk over 26 years. Clin. J. Sport Med. 2010, 20, 318–321. [Google Scholar] [CrossRef]
- Traiperm, N.; Gatterer, H.; Burtscher, M. Plasma electrolyte and hematological changes after marathon running in adolescents. Med. Sci. Sports Exerc. 2013, 45, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.T.; Knechtle, B. Pacing in age group marathoners in the “New York city marathon”. Res. Sports Med. (Print) 2018, 26, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Hew, T.D.; Chorley, J.N.; Cianca, J.C.; Divine, J.G. The incidence, risk factors, and clinical manifestations of hyponatremia in marathon runners. Clin. J. Sport Med. 2003, 13, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Mettler, S.; Rusch, C.; Frey, W.O.; Bestmann, L.; Wenk, C.; Colombani, P.C. Hyponatremia among runners in the zurich marathon. Clin. J. Sport Med. 2008, 18, 344–349. [Google Scholar] [CrossRef]
- Almond, C.S.; Shin, A.Y.; Fortescue, E.B.; Mannix, R.C.; Wypij, D.; Binstadt, B.A.; Duncan, C.N.; Olson, D.P.; Salerno, A.E.; Newburger, J.W.; et al. Hyponatremia among runners in the boston marathon. N. Engl. J. Med. 2005, 352, 1550–1556. [Google Scholar] [CrossRef]
- Chorley, J.; Cianca, J.; Divine, J. Risk factors for exercise-associated hyponatremia in non-elite marathon runners. Clin. J. Sport Med. 2007, 17, 471–477. [Google Scholar] [CrossRef]
- Davis, D.P.; Videen, J.S.; Marino, A.; Vilke, G.M.; Dunford, J.V.; Van Camp, S.P.; Maharam, L.G. Exercise-associated hyponatremia in marathon runners: A two-year experience. J. Emerg. Med. 2001, 21, 47–57. [Google Scholar] [CrossRef]
- Reid, S.A.; Speedy, D.B.; Thompson, J.M.; Noakes, T.D.; Mulligan, G.; Page, T.; Campbell, R.G.; Milne, C. Study of hematological and biochemical parameters in runners completing a standard marathon. Clin. J. Sport Med. 2004, 14, 344–353. [Google Scholar] [CrossRef]
- Hew-Butler, T.; Ayus, J.C.; Kipps, C.; Maughan, R.J.; Mettler, S.; Meeuwisse, W.H.; Page, A.J.; Reid, S.A.; Rehrer, N.J.; Roberts, W.O.; et al. Statement of the second international exercise-associated hyponatremia consensus development conference, New Zealand, 2007. Clin. J. Sport Med. 2008, 18, 111–121. [Google Scholar] [CrossRef]
- Noakes, T. Fluid replacement during marathon running. Clin. J. Sport Med. 2003, 13, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.A.; Stull, G.A.; Apple, F.S. Creatine kinase isoenzyme activities in men and women following a marathon race. Med. Sci. Sports Exerc. 1985, 17, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Munjal, D.D.; McFadden, J.A.; Matix, P.A.; Coffman, K.D.; Cattaneo, S.M. Changes in serum myoglobin, total creatine kinase, lactate dehydrogenase and creatine kinase mb levels in runners. Clin. Biochem. 1983, 16, 195–199. [Google Scholar] [CrossRef]
- Niemela, M.; Kangastupa, P.; Niemela, O.; Bloigu, R.; Juvonen, T. Acute changes in inflammatory biomarker levels in recreational runners participating in a marathon or half-marathon. Sports Med. Open 2016, 2, 21. [Google Scholar] [CrossRef] [PubMed]
- Neviackas, J.A.; Bauer, J.H. Renal function abnormalities induced by marathon running. South. Med J. 1981, 74, 1457–1460. [Google Scholar] [CrossRef] [PubMed]
- Mydlik, M.; Derzsiova, K.; Bohus, B. Renal function abnormalities after marathon run and 16-kilometre long-distance run. Prz. Lek. 2012, 69, 1–4. [Google Scholar] [PubMed]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knechtle, B.; Bamert, J.; Rosemann, T.; Nikolaidis, P.T. Exercise-Associated Hyponatremia During a Self-Paced Marathon Attempt in a 15-Year-Old Male Teenager. Medicina 2019, 55, 63. https://doi.org/10.3390/medicina55030063
Knechtle B, Bamert J, Rosemann T, Nikolaidis PT. Exercise-Associated Hyponatremia During a Self-Paced Marathon Attempt in a 15-Year-Old Male Teenager. Medicina. 2019; 55(3):63. https://doi.org/10.3390/medicina55030063
Chicago/Turabian StyleKnechtle, Beat, Jonah Bamert, Thomas Rosemann, and Pantelis T. Nikolaidis. 2019. "Exercise-Associated Hyponatremia During a Self-Paced Marathon Attempt in a 15-Year-Old Male Teenager" Medicina 55, no. 3: 63. https://doi.org/10.3390/medicina55030063