Common Variations in Prothrombotic Genes and Susceptibility to Ischemic Stroke in Young Patients: A Case-Control Study in Southeast Iran

 ,
,
Abstract
:1. Intoduction
2. Materials and Methods
2.1. Participants
2.2. Genomic DNA Extraction and Genotyping
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. MTHFR Polymorphisms and Ischemic Stroke Risk
3.3. MTHFR C677T Polymorphism
3.4. MTHFR A1298C Polymorphism
3.5. MTHFR C2572A Polymorphism
3.6. MTHFR C4869G Polymorphism
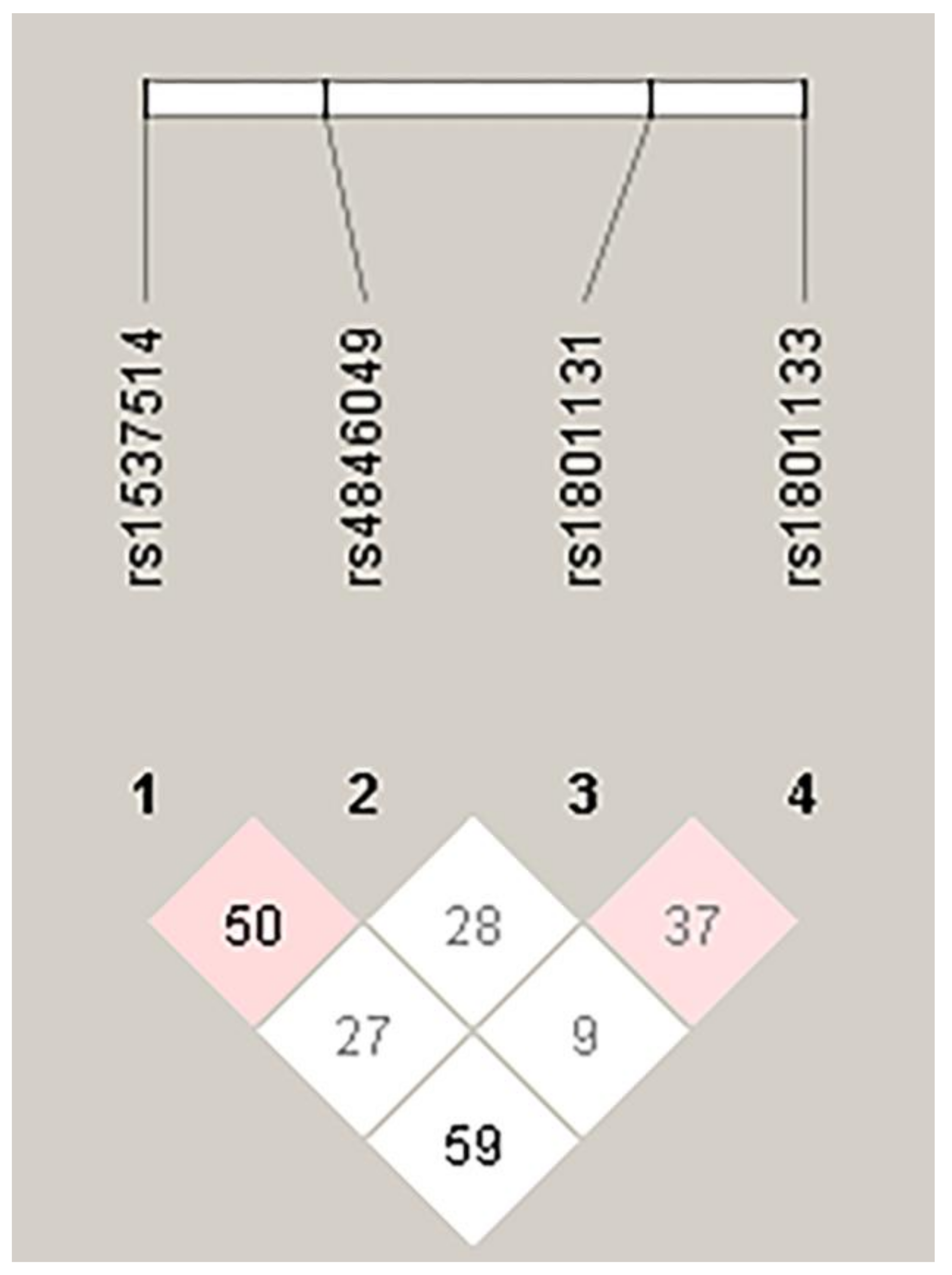
3.7. Haplotype Analysis of MTHFR Polymorphisms
3.8. FVL G1691A and Prothrombin G20210A Polymorphisms and Ischemic Stroke Risk
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Mukherjee, D.; Patil, C.G. Epidemiology and the global burden of stroke. World Neurosurg. 2011, 76, S85–S90. [Google Scholar] [CrossRef]
- Deresse, B.; Shaweno, D. Epidemiology and in-hospital outcome of stroke in South Ethiopia. J. Neurol. Sci. 2015, 355, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Owolabi, M.O.; Akarolo-Anthony, S.; Akinyemi, R.; Arnett, D.; Gebregziabher, M.; Jenkins, C.; Tiwari, H.; Arulogun, O.; Akpalu, A.; Sarfo, F.S.; et al. The burden of stroke in Africa: A glance at the present and a glimpse into the future. Cardiovasc. J. Afr. 2015, 26, S27–S38. [Google Scholar] [CrossRef] [PubMed]
- WHO Statistical Information System (WHO SIS): Core Health Indicators Database IRoI; World Health Organization: Geneva, Switzerland, 2015.
- Caplan, L. Caplan’s Stroke, 4th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2009. [Google Scholar]
- Arsene, D.; Gaina, G.; Balescu, C.; Ardeleanu, C. C677T and A1298C methylenetetrahydropholate reductase (MTHFR) polymorphisms as factors involved in ischemic stroke. Rom. J. Morphol. Embryol. 2011, 52, 1203–1207. [Google Scholar]
- Salimi, S.; Firoozrai, M.; Zand, H.; Nakhaee, A.; Shafiee, S.M.; Tavilani, H.; Mohebbi, A. Endothelial nitric oxide synthase gene Glu298Asp polymorphism in patients with coronary artery disease. Ann. Saudi Med. 2010, 30, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Salimi, S.; Naghavi, A.; Firoozrai, M.; Zand, H.; Tavilani, H.; Nakhaee, A.; Mohebbi, A. Association of plasma nitric oxide concentration and endothelial nitric oxide synthase T-786C gene polymorphism in coronary artery disease. Pathophysiology 2012, 19, 157–162. [Google Scholar] [CrossRef]
- Amin, F.; Jahani, M.M.; Ghaedi, H.; Alipoor, B.; Fatemi, A.; Tajik, M.; Sharifi, Z.; Golmohammadi, T.; Askari, M.; Azarnejad, A.; et al. Genetic Variants of Cytochrome b-245, Alpha Polypeptide Gene and Premature Acute Myocardial Infarction Risk in an Iranian Population. J. Med. Biochem. 2015, 34, 402–408. [Google Scholar] [CrossRef]
- Miranda-Vilela, A.L. Role of polymorphisms in factor V (FV Leiden), prothrombin, plasminogen activator inhibitor type-1 (PAI-1), methylenetetrahydrofolate reductase (MTHFR) and cystathionine beta-synthase (CBS) genes as risk factors for thrombophilias. Mini Rev. Med. Chem. 2012, 12, 997–1006. [Google Scholar] [CrossRef]
- Hoffbrand, A.V.M.P.; Pettit, J.A. Thrombosis and Antithrombotic Therapy. In Essential Haematology; Blackwell Publishing: Hoboken, NJ, USA, 2006. [Google Scholar]
- D’Uva, M.; Micco, P.D.; Strina, I.; Placido, G.D. Recurrent pregnancy loss and thrombophilia. J. Clin. Med. Res. 2010, 2, 18–22. [Google Scholar] [CrossRef]
- Santilli, F.; Davi, G.; Patrono, C. Homocysteine, methylenetetrahydrofolate reductase, folate status and atherothrombosis: A mechanistic and clinical perspective. Vascul. Pharmacol. 2016, 78, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Li, B.; Wang, C.; Wang, P.; Gao, X.; Liu, G. Association between 5,10-Methylenetetrahydrofolate Reductase C677T Gene Polymorphism and Risk of Ischemic Stroke: A Meta-analysis. J. Stroke Cerebrovasc. Dis. 2016, 25, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Carp, H.; Salomon, O.; Seidman, D.; Dardik, R.; Rosenberg, N.; Inbal, A. Prevalence of genetic markers for thrombophilia in recurrent pregnancy loss. Hum Reprod. 2002, 17, 1633–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, M.V.; Newcombe, P.; Hubacek, J.A.; Sofat, R.; Ricketts, S.L.; Cooper, J.; Breteler, M.M.; Bautista, L.E.; Sharma, P.; Whittaker, J.C.; et al. Effect modification by population dietary folate on the association between MTHFR genotype, homocysteine, and stroke risk: A meta-analysis of genetic studies and randomised trials. Lancet 2011, 378, 584–594. [Google Scholar] [CrossRef]
- Mohammadpour-Gharehbagh, A.; Teimoori, B.; Narooei-Nejad, M.; Mehrabani, M.; Saravani, R.; Salimi, S. The association of the placental MTHFR 3’-UTR polymorphisms, promoter methylation, and MTHFR expression with preeclampsia. J. Cell Biochem. 2018, 119, 1346–1354. [Google Scholar] [CrossRef] [PubMed]
- Mohammadpour-Gharehbagh, A.; Salimi, S.; Keshavarzi, F.; Saeidian, F.; Mousavi, M.; Teimoori, B.; Esmaeilipour, M.; Mokhtari, M. Genetic variants in 3’-UTRs of MTHFR in the pregnancies complicated with preeclampsia and bioinformatics analysis. J. Cell Biochem. 2018, 119, 773–781. [Google Scholar] [CrossRef]
- Salimi, S.; Saravani, M.; Yaghmaei, M.; Fazlali, Z.; Mokhtari, M.; Naghavi, A.; Farajian-Mashhadi, F. The early-onset preeclampsia is associated with MTHFR and FVL polymorphisms. Arch Gynecol. Obstet. 2015, 291, 1303–1312. [Google Scholar] [CrossRef]
- Ueland, P.M.; Refsum, H.; Beresford, S.A.; Vollset, S.E. The controversy over homocysteine and cardiovascular risk. Am. J. Clin. Nutr. 2000, 72, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Austin, R.C.; Lentz, S.R.; Werstuck, G.H. Role of hyperhomocysteinemia in endothelial dysfunction and atherothrombotic disease. Cell Death Differ. 2004, 11 (Suppl. 1), S56–S64. [Google Scholar] [CrossRef] [Green Version]
- Buemi, M.; Marino, D.; Di Pasquale, G.; Floccari, F.; Ruello, A.; Aloisi, C.; Corica, F.; Senatore, M.; Romeo, A.; Frisina, N. Effects of homocysteine on proliferation, necrosis, and apoptosis of vascular smooth muscle cells in culture and influence of folic acid. Thromb Res. 2001, 104, 207–213. [Google Scholar] [CrossRef]
- White, W.M.; Turner, S.T.; Bailey, K.R.; Mosley, T.H.; Jr Kardia, S.L.; Wiste, H.J.; Kullo, I.J.; Garovic, V.D. Hypertension in pregnancy is associated with elevated homocysteine levels later in life. Am. J. Obstet. Gynecol. 2013, 209, 454.e1–454.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaffer, A.; Verdoia, M.; Cassetti, E.; Marino, P.; Suryapranata, H.; De Luca, G.; Novara Atherosclerosis Study, G. Relationship between homocysteine and coronary artery disease. Results from a large prospective cohort study. Thromb Res. 2014, 134, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Lehotsky, J.; Tothova, B.; Kovalska, M.; Dobrota, D.; Benova, A.; Kalenska, D.; Kaplan, P. Role of Homocysteine in the Ischemic Stroke and Development of Ischemic Tolerance. Front Neurosci. 2016, 10, 538. [Google Scholar] [CrossRef] [PubMed]
- Kullo, I.J.; Ding, K.; Boerwinkle, E.; Turner, S.T.; Mosley, T.H.; Kardia, S.L., Jr.; de Andrade, M. Novel genomic loci influencing plasma homocysteine levels. Stroke 2006, 37, 1703–1709. [Google Scholar] [CrossRef]
- Trimmer, E.E. Methylenetetrahydrofolate reductase: Biochemical characterization and medical significance. Curr. Pharm. Des. 2013, 19, 2574–2593. [Google Scholar] [CrossRef] [PubMed]
- Van Meurs, J.B.; Pare, G.; Schwartz, S.M.; Hazra, A.; Tanaka, T.; Vermeulen, S.H.; Cotlarciuc, I.; Yuan, X.; Malarstig, A.; Bandinelli, S.; et al. Common genetic loci influencing plasma homocysteine concentrations and their effect on risk of coronary artery disease. Am. J. Clin. Nutr. 2013, 98, 668–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisberg, I.S.; Jacques, P.F.; Selhub, J.; Bostom, A.G.; Chen, Z.; Curtis Ellison, R.; Eckfeldt, J.H.; Rozen, R. The 1298A-->C polymorphism in methylenetetrahydrofolate reductase (MTHFR): In vitro expression and association with homocysteine. Atherosclerosis 2001, 156, 409–415. [Google Scholar] [CrossRef]
- Kujovich, J.L. Factor V Leiden thrombophilia. Genet. Med. 2011, 13, 1–16. [Google Scholar] [CrossRef]
- Chen, M.; Mao, B.Y.; Wang, D.; Cheng, X.; Xu, C.X. Association between rs1801133 polymorphism and risk of adult ischemic stroke: Meta-analysis based on case-control studies. Thromb Res. 2016, 137, 17–25. [Google Scholar] [CrossRef]
- Kumar, A.; Kumar, P.; Prasad, M.; Sagar, R.; Yadav, A.K.; Pandit, A.K.; Jali, V.P.; Pathak, A. Association of C677T polymorphism in the methylenetetrahydrofolate reductase gene (MTHFR gene) with ischemic stroke: A meta-analysis. Neurol Res. 2015, 37, 568–577. [Google Scholar] [CrossRef]
- Cui, T. MTHFR C677T mutation increased the risk of Ischemic Stroke, especially in large-artery atherosclerosis in adults: An updated meta-analysis from 38 researches. Int. J. Neurosci. 2016, 126, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Abhinand, P.A.; Manikandan, M.; Mahalakshmi, R.; Ragunath, P.K. Meta-analysis study to evaluate the association of MTHFR C677T polymorphism with risk of ischemic stroke. Bioinformation 2017, 13, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.J.; Hu, Z.C.; Yin, Y.W.; Li, B.H.; Liu, Y.; Liao, S.Q.; Gao, C.Y.; Li, J.C.; Zhang, L.L. A meta-analysis of the relationship between MTHFR gene A1298C polymorphism and the risk of adult stroke. Cerebrovasc. Dis. 2014, 38, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Sarecka-Hujar, B.; Kopyta, I.; Skrzypek, M. Is the 1298A>C polymorphism in the MTHFR gene a risk factor for arterial ischaemic stroke in children? The results of meta-analysis. Clin. Exp. Med. 2018, 18, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, L.K.; Au, A.; Menon, S.; Griffiths, L.R.; Kooi, C.W.; Irene, L.; Zhao, J.; Lee, C.; Alekseevna, A.M.; Hassan, M.R.A.; et al. Polymorphisms of MTHFR, eNOS, ACE, AGT, ApoE, PON1, PDE4D, and Ischemic Stroke: Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 2482–2493. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.O.; Park, H.S.; Ryu, C.S.; Shin, J.W.; Kim, J.; Oh, S.H.; Kim, O.J.; Kim, N.K. Interplay between 3’-UTR polymorphisms in the methylenetetrahydrofolate reductase (MTHFR) gene and the risk of ischemic stroke. Sci. Rep. 2017, 7, 12464. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; He, W.; Wang, Y.; Hua, J. Tagging Functional Polymorphism in 3’ Untranslated Region of Methylene Tetrahydrofolate Reductase and Risk of Ischemic Stroke. Cell Physiol. Biochem. 2018, 46, 1019–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentley, P.; Peck, G.; Smeeth, L.; Whittaker, J.; Sharma, P. Causal relationship of susceptibility genes to ischemic stroke: Comparison to ischemic heart disease and biochemical determinants. PLoS ONE 2010, 5, e9136. [Google Scholar] [CrossRef] [PubMed]
- Hamzi, K.; Tazzite, A.; Nadifi, S. Large-scale meta-analysis of genetic studies in ischemic stroke: Five genes involving 152,797 individuals. Indian J. Hum. Genet. 2011, 17, 212–217. [Google Scholar] [CrossRef]
- Peck, G.; Smeeth, L.; Whittaker, J.; Casas, J.P.; Hingorani, A.; Sharma, P. The genetics of primary haemorrhagic stroke, subarachnoid haemorrhage and ruptured intracranial aneurysms in adults. PLoS ONE 2008, 3, e3691. [Google Scholar] [CrossRef]
- Alhazzani, A.A.; Kumar, A.; Selim, M. Association between Factor V Gene Polymorphism and Risk of Ischemic Stroke: An Updated Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2018, 27, 1252–1261. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Controls n = 157 | IS n = 106 | p-Value |
|---|---|---|---|
| Age (years) | 37.2 ±10.8 | 36.9 ± 10.3 | 0.8 a |
| Sex (male/female) | 69/88 | 42/64 | 0.5 b |
| Smoking (n, %) | 28 (17.8) | 29 (27.4) | 0.07 b |
| SBP (mmHg) | 117 ± 18 | 118 ± 24 | 0.7 a |
| DBP (mmHg) | 75 ± 8.4 | 77 ± 17 | 0.3 a |
| Triglycerides (mg/dL) | 100 ± 64 | 109 ± 79 | 0.3 a |
| Total Cholesterol(mg/dL) | 148 ± 35 | 160 ± 39 | 0.08 a |
| LDL Cholesterol (mg/dL) | 87± 22 | 92 ± 25 | 0.1 a |
| HDL Cholesterol (mg/dL) | 39 ± 10 | 39 ± 11 | 0.9 a |
| Polymorphism | IS (n = 106) | Control (n = 157) | p-Value | Odds Ratio (95% CI) | |
|---|---|---|---|---|---|
| MTHFRC677T rs1801133 | genotype | ||||
| CC, n (%) | 66 (62.3) | 119 (75.8) | 1 | ||
| CT, n (%) | 32 (30.2) | 30 (19.1) | 0.028 | 1.9 (1.1–3.4) | |
| TT, n (%) | 8 (7.5) | 8 (5.1) | 0.26 | 1.8 (0.7–5) | |
| Dominant (CT + TT vs. CC) | 0.019 | 1.9 (1.1–3.3) | |||
| Recessive (TT vs. CT + CC) | 0.4 | 1.5 (0.6–4.2) | |||
| Allele | |||||
| C, n (%) | 164 (77.4) | 268 (85) | 1 | ||
| T, n (%) | 48 (22.6) | 46 (15) | 0.02 | 1.7 (1.1–2.7) | |
| MTHFRA1298C | genotype | ||||
| rs1801131 | AA, n (%) | 72 (67.9) | 120 (76.4) | 1 | |
| AC, n (%) | 31 (29.3) | 32 (20.4) | 0.1 | 1.6 (0.9–2.9) | |
| CC, n (%) | 3 (2.8) | 5 (3.2) | 1 | 1 (0.2–4.3) | |
| Dominant (AC + CC vs. AA) | 0.13 | 1.5 (0.9–2.7) | |||
| Recessive (CC vs. AC + AA) | 0.9 | 0.9 (0.2–3.8) | |||
| Allele | |||||
| A, n (%) | 175 (83) | 272 (87) | 1 | ||
| C, n (%) | 37 (17) | 42 (13) | 0.2 | 1.4 (0.9–2.2) | |
| MTHFR C2572A rs4846049 | genotype | ||||
| AA, n (%) | 25 (23.6) | 25 (15.9) | 1 | ||
| AC, n (%) | 50 (47.2) | 84 (53.5) | 0.12 | 0.6 (0.3–1.2) | |
| CC, n (%) | 31 (29.2) | 48 (30.6) | 0.23 | 0.7 (0.3–1.3) | |
| Dominant (AC + CC vs. AA) | 0.12 | 0.6 (0.3–1.1) | |||
| Recessive (CC vs. AC + AA) | 0.8 | 0.9 (0.6–1.6) | |||
| Allele | |||||
| A, n (%) | 100 (47) | 134 (43) | |||
| C, n (%) | 112 (53) | 180 (57) | 0.3 | 0.8 (0.6–1.2) | |
| MTHFR C4869G rs1537514 | genotype | ||||
| CC, n (%) | 93 (87.7) | 117 (74.5) | 1 | ||
| CG, n (%) | 13 (12.3) | 38 (24.2) | 0.016 | 0.4 (0.2–0.9) | |
| GG, n (%) | 0 | 2 (1.3) | 1 | - | |
| Dominant (CG + GG vs. CC) | 0.01 | 0.4 (0.2–0.8) | |||
| Recessive (GG vs. CG + CC) | - | - | |||
| Allele | |||||
| C, n (%) | 199 (94) | 272 (87) | |||
| G, n (%) | 13 (6) | 42 (13) | 0.009 | 0.4 (0.2-0.8) | |
| FVL G1691A rs6025 | genotype | ||||
| GG, n (%) | 90 (84.9) | 144 (91.7) | |||
| GA, n (%) | 16 (15.1) | 13 (8.3) | 0.09 | 2 (0.9–4.3) | |
| AA, n (%) | 0 (0) | 0 (0) | - | - | |
| Allele | |||||
| G, n (%) | 196 (92.5) | 301 (96) | |||
| A, n (%) | 16 (7.5) | 13 (4) | 0.12 | 1.9 (0.9–4) |
| Haplotypes | IS | Control | p-Value | OR (95% CI) |
|---|---|---|---|---|
| CCAC | 73 (0.344) | 127 (0.404) | 0.17 | 0.8 (0.5–1.1) |
| CAAC | 60 (0.283) | 84 (0.268) | 0.76 | 1.1 (0.7–1.6) |
| GAAC | 8 (0.0377) | 29 (0.092) | 0.02 | 0.4 (0.2–0.9) |
| CCCC | 16 (0.0750) | 16 (0.051) | 0.28 | 1.5 (0.7–3.1) |
| CAAT | 18 (0.0849) | 10 (0.032) | 0.01 | 2.8 (1.3–6.2) |
| CCAT | 11 (0.052) | 14 (0.045) | 0.83 | 1.2 (0.5–2.6) |
| CCCT | 8 (0.038) | 13 (0.041) | 0.96 | 0.9 (0.4–2.2) |
| CACT | 8 (0.0380) | 5 (0.016) | 0.15 | 2.4 (0.8–7.5) |
| GCAC | 3 (0.014) | 9 (0.029) | 0.38 | 0.5 (0.1–1.8) |
| CACC | 4 (0.019) | 3 (0.010) | 0.43 | 2 (0.4–9) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashemi, S.M.; Ramroodi, N.; Amiri Fard, H.; Talebian, S.; Haghighi Rohani, M.; Rezaei, M.; Noora, M.; Salimi, S. Common Variations in Prothrombotic Genes and Susceptibility to Ischemic Stroke in Young Patients: A Case-Control Study in Southeast Iran. Medicina 2019, 55, 47. https://doi.org/10.3390/medicina55020047
Hashemi SM, Ramroodi N, Amiri Fard H, Talebian S, Haghighi Rohani M, Rezaei M, Noora M, Salimi S. Common Variations in Prothrombotic Genes and Susceptibility to Ischemic Stroke in Young Patients: A Case-Control Study in Southeast Iran. Medicina. 2019; 55(2):47. https://doi.org/10.3390/medicina55020047
Chicago/Turabian StyleHashemi, Seyed Mehdi, Nourollah Ramroodi, Hamed Amiri Fard, Sahar Talebian, Maryam Haghighi Rohani, Mahnaz Rezaei, Mehrangiz Noora, and Saeedeh Salimi. 2019. "Common Variations in Prothrombotic Genes and Susceptibility to Ischemic Stroke in Young Patients: A Case-Control Study in Southeast Iran" Medicina 55, no. 2: 47. https://doi.org/10.3390/medicina55020047