Molecular Characterization of Uropathogenic Escherichia coli Reveals Emergence of Drug Resistant O15, O22 and O25 Serogroups

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Escherichia coli Isolates
2.2. Study Groups
2.3. Evaluation of Antimicrobial Susceptibility
2.4. Preparation of Template DNA
2.5. Serogrouping of E. coli Isolates by Using Multiplex PCR
2.6. Phylogenetic Grouping of E. coli Isolates
2.7. Statistical Analysis
3. Results
3.1. Prevalence of E. coli-Caused Conditions
3.2. Age Distribution among Patients with E. coli-Caused UTC
3.3. Antimicrobial Susceptibility Patterns among UPEC
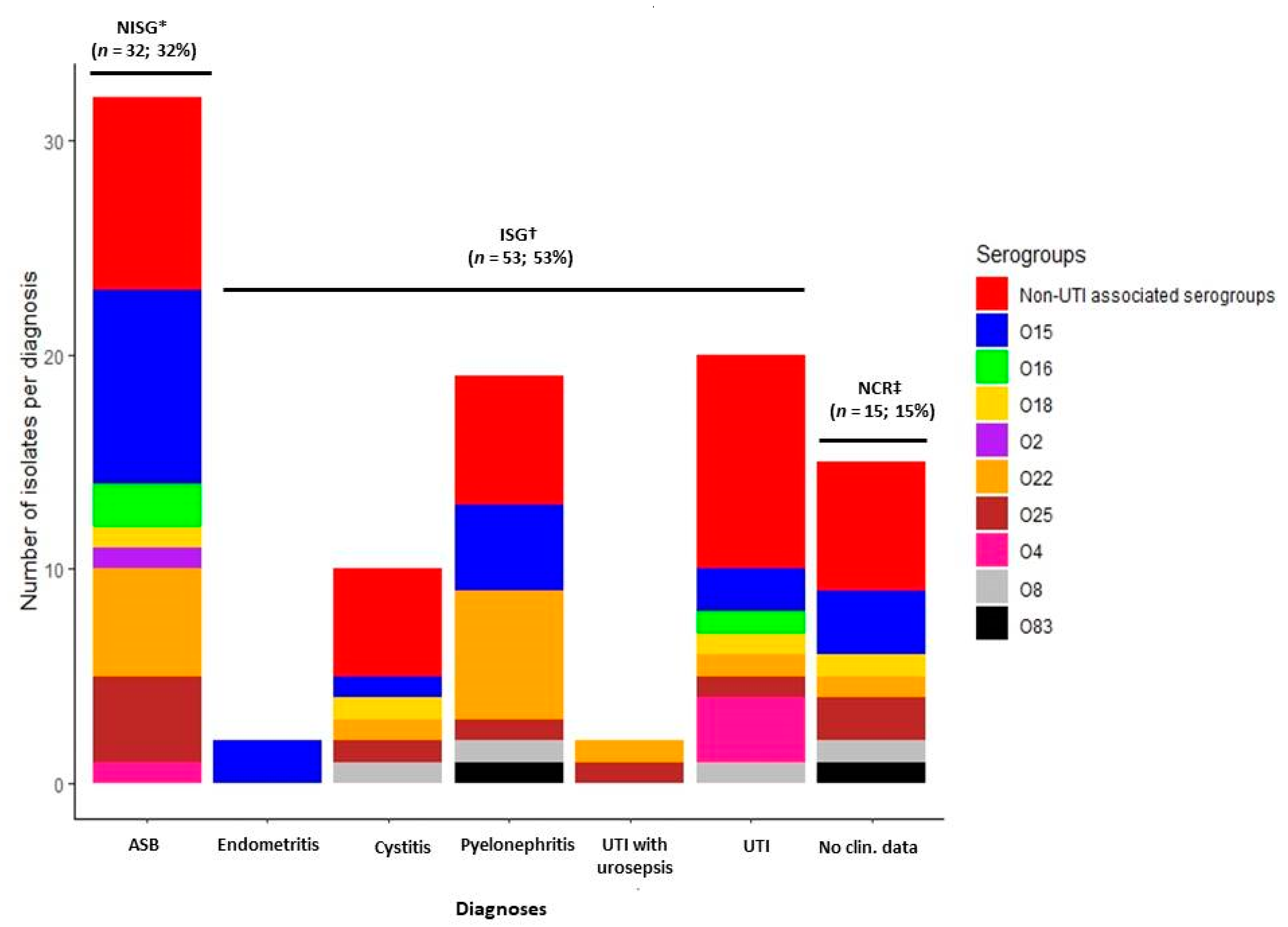
3.4. Serological Diversity among E. coli Strains Isolated from Patients with UTC
3.5. Increased Multidrug Antimicrobial Resistance Observed among O15 Serogroup
3.6. Phylogenetic Diversity among E. coli Isolates
3.7. Patterns of Antimicrobial Susceptibility among E. coli Phylogenetic Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Russo, T. Medical and economic impact of extraintestinal infections due to Escherichia coli: Focus on an increasingly important endemic problem. Microbes Infect. 2003, 5, 449–456. [Google Scholar] [CrossRef]
- Köhler, C.-D.; Dobrindt, U. What defines extraintestinal pathogenic Escherichia coli? Int. J. Med. Microbiol. 2011, 301, 642–647. [Google Scholar]
- Hooton, T.M. Clinical practice. Uncomplicated urinary tract infection. N. Engl. J. Med. 2012, 366, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Urinary tract infection syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. N. Am. 2014, 28, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mediavilla, J.R.; Patrawalla, A.; Chen, L.; Chavda, K.D.; Mathema, B.; Vinnard, C.; Dever, L.L.; Kreiswirth, B.N. Colistin- and carbapenem-resistant Escherichia coli harboring mcr-1 and blaNDM-5, causing a complicated urinary tract infection in a patient from the United States. mBio 2016, 7, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Nicolas-Chanoine, M.H.; Blanco, J.; Leflon-Guibout, V.; Demarty, R.; Alonso, M.P.; Caniça, M.M.; Park, Y.-J.; Lavigne, J.-P.; Pitout, J.; Johnson, J.R. Intercontinental emergence of Escherichia coli clone O25:H4-ST131 producing CTX-M-15. J. Antimicrob. Chemother. 2008, 61, 273–281. [Google Scholar]
- Banerjee, R.; Johnson, J.R. A new clone sweeps clean: The enigmatic emergence of Escherichia coli sequence type 131. Antimicrob. Agents Chemother. 2014, 58, 4997–5004. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S. Human Meningitis-Associated Escherichia coli. EcoSal Plus 2016, 7. [Google Scholar] [CrossRef] [PubMed]
- Blanco, M.; Alonso, M.P.; Blanco, J. Virulence factors and O groups of Escherichia coli isolates from patients with acute pyelonephritis, cystitis and asymptomatic bacteriuria. Eur. J. Epidemiol. 1996, 12, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Momtaz, H.; Karimian, A.; Madani, M.; Dehkordi, F.S.; Ranjbar, R.; Sarshar, M.; Souod, N. Uropathogenic Escherichia coli in Iran: Serogroup distributions, virulence factors and antimicrobial resistance properties. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Clermont, O.; Christenson, J.K.; Denamur, E.; Gordon, D.M. The Clermont Escherichia coli phylo-typing method revisited: Improvement of specificity and detection of new phylo-groups. Environ. Microbiol. Rep. 2013, 5, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.R.; Stell, A.L. Extended virulence genotypes of Escherichia coli strains from patients with urosepsis in relation to phylogeny and host compromise. J. Infect. Dis. 2000, 181, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Picard, B.; Garcia, J.S.; Gouriou, S.; Duriez, P.; Brahimi, N.; Bingen, E.; Elion, J.; Denamur, E. The Link between Phylogeny and Virulence in Escherichia coli Extraintestinal Infection. Infect. Immun. 1999, 67, 546–553. [Google Scholar] [PubMed]
- Stoppe, N.D.C.; Silva, J.S.; Carlos, C.; Sato, M.I.Z.; Saraiva, A.M.; Ottoboni, L.M.M.; Torres, T.T. Worldwide Phylogenetic Group Patterns of Escherichia coli from Commensal Human and Wastewater Treatment Plant Isolates. Front. Microbiol. 2017, 8, 2512. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Saralaya, V.; Adhikari, P.; Shenoy, S.; Baliga, S.; Hegde, A. Characterization of Escherichia coli Phylogenetic Groups Associated with Extraintestinal Infections in South Indian Population. Ann. Med Heal. Sci. Res. 2015, 5, 241–246. [Google Scholar]
- Da Silva, G.J.; Mendonça, N. Association between antimicrobial resistance and virulence in Escherichia coli. Virulence 2012, 3, 18–28. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters, version 8.1. 2018. Available online: http://www.eucast.org/clinical_breakpoints/ (accessed on 5 March 2019).
- van Tongeren, S.P.; Degener, J.E.; Harmsen, H.J. Comparison of three rapid and easy bacterial DNA extraction methods for use with quantitative real-time PCR. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1053–1061. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Liu, B.; Chen, M.; Guo, D.; Guo, X.; Liu, F.; Feng, L.; Wang, L. A multiplex PCR method to detect 14 Escherichia coli serogroups associated with urinary tract infections. J. Microbiol. Methods 2010, 82, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Clermont, O.; Bonacorsi, S.; Bingen, E. Rapid and Simple Determination of the Escherichia coli Phylogenetic Group. Appl. Environ. Microbiol. 2000, 66, 4555–4558. [Google Scholar] [CrossRef] [PubMed]
- Minardi, D.; D’Anzeo, G.; Cantoro, D.; Conti, A.; Muzzonigro, G. Urinary tract infections in women: Etiology and treatment options. Int. J. Gen. Med. 2011, 4, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Scholes, D.; Hooton, T.M.; Roberts, P.L.; Stapleton, A.E.; Stamm, W.E. Risk Factors for Recurrent Urinary Tract Infection in Young Women. J. Infect. Dis. 2000, 182, 1177–1182. [Google Scholar]
- Raz, R. Urinary Tract Infection in Postmenopausal Women. Korean J. Urol. 2011, 52, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Swami, S.K.; Liesinger, J.T.; Shah, N.; Baddour, L.M.; Banerjee, R. Incidence of Antibiotic-Resistant Escherichia coli Bacteriuria According to Age and Location of Onset: A Population-Based Study from Olmsted County, Minnesota. Mayo Clin. Proc. 2012, 87, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, A.; Goldman, R.D. Management of asymptomatic bacteriuria in children. Can. Fam. Physician. 2018, 64, 821–824. [Google Scholar] [PubMed]
- Imade, P.E.; Izekor, P.E.; Eghafona, N.O.; Enabulele, O.I.; Ophori, E. Asymptomatic bacteriuria among pregnant women. N. Am. J. Med. Sci. 2010, 2, 263–266. [Google Scholar] [PubMed]
- Mor, G.; Cardenas, I. The immune system in pregnancy: A unique complexity. Am. J. Reprod. Immunol. 2010, 63, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Sheiner, E.; Mazor-Drey, E.; Levy, A. Asymptomatic bacteriuria during pregnancy. J. Matern. Neonatal Med. 2009, 22, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Krohn, M.A.; Thwin, S.S.; Rabe, L.K.; Brown, Z.; Hillier, S.L. Vaginal Colonization by Escherichia coli as a Risk Factor for Very Low Birth Weight Delivery and Other Perinatal Complications. J. Infect. Dis. 1997, 175, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Caciagli, P.; Mereu, L.; Cai, T.; Nesi, G.; Mazzoli, S.; Meacci, F.; Lanzafame, P.; Tateo, S.; Malossini, G.; Selli, C.; et al. Asymptomatic Bacteriuria Treatment Is Associated With a Higher Prevalence of Antibiotic Resistant Strains in Women With Urinary Tract Infections. Clin. Infect. Dis. 2015, 61, 1655–1661. [Google Scholar]
- Córdoba, G.; Holm, A.; Hansen, F.; Hammerum, A.M.; Bjerrum, L. Prevalence of antimicrobial resistant Escherichia coli from patients with suspected urinary tract infection in primary care, Denmark. BMC Infect. Dis. 2017, 17, 670. [Google Scholar] [CrossRef] [PubMed]
- Kõljalg, S.; Truusalu, K.; Vainumäe, I.; Stsepetova, J.; Sepp, E.; Mikelsaar, M. Persistence of Escherichia coli Clones and Phenotypic and Genotypic Antibiotic Resistance in Recurrent Urinary Tract Infections in Childhood. J. Clin. Microbiol. 2008, 47, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Giedraitienė, A.; Vitkauskienė, A.; Ašmonienė, V.; Plančiūnienė, R.; Simonytė, S.; Pavilonis, A. CTX-M-producing Escherichia coli in Lithuania: Associations between sites of infection, coresistance, and phylogenetic groups. Medicina 2013, 49, 393–398. [Google Scholar]
- Hitzenbichler, F.; Simon, M.; Holzmann, T.; Iberer, M.; Zimmermann, M.; Salzberger, B.; Hanses, F. Antibiotic resistance in E. coli isolates from patients with urinary tract infections presenting to the emergency department. Infection 2018, 46, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Fasugba, O.; Gardner, A.; Mitchell, B.G.; Mnatzaganian, G. Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: A systematic review and meta-analysis of observational studies. BMC Infect. Dis. 2015, 15, 545. [Google Scholar] [CrossRef] [PubMed]
- van de Sande-Bruinsma, N.; Grundmann, H.; Verloo, D.; Tiemersma, E.; Monen, J.; Goossens, H.; Ferech, M.; European Antimicrobial Resistance Surveillance System Group; European Surveillance of Antimicrobial Consumption Project Group. Antimicrobial drug use and resistance in Europe. Emerg. Infect. Dis. 2008, 14, 1722–1730. [Google Scholar] [CrossRef] [PubMed]
- Stefaniuk, E.; Suchocka, U.; Bosacka, K.; Hryniewicz, W. Etiology and antibiotic susceptibility of bacterial pathogens responsible for community-acquired urinary tract infections in Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1363–1369. [Google Scholar] [CrossRef] [PubMed]
- Olesen, B.; Scheutz, F.; Menard, M.; Skov, M.N.; Kolmos, H.J.; Kuskowski, M.A.; Johnson, J.R. Three-Decade Epidemiological Analysis of Escherichia coli O15:K52:H1. J. Clin. Microbiol. 2009, 47, 1857–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, M.; Blanco, J.E.; Alonso, M.; Mora, A.; Balsalobre, C.; Muñoa, F.; Juárez, A.; Blanco, J. Detection of pap, sfa and afa adhesin-encoding operons in uropathogenic Escherichia coli strains: Relationship with expression of adhesins and production of toxins. Res. Microbiol. 1997, 148, 745–755. [Google Scholar] [CrossRef]
- Mora, A.; Blanco, M.; Lopez, C.; Mamani, R.; Blanco, J.E.; Alonso, M.P.; García-Garrote, F.; Dahbi, G.; Herrera, A.; Fernández, A.; et al. Emergence of clonal groups O1:HNM-D-ST59, O15:H1-D-ST393, O20:H34/HNM-D-ST354, O25b:H4-B2-ST131 and ONT:H21,42-B1-ST101 among CTX-M-14-producing Escherichia coli clinical isolates in Galicia, northwest Spain. Int. J. Antimicrob. Agents 2011, 37, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study Groups | No. of Isolates (%) | Distribution among Sexes | Frequency of Resistance (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. among F (%) a | No. among M (%) b | AMP | AMC | CXM | CIP | AK | CN | TOB | F | TMP | IPM | MEM | ||
| Total isolates of E. coli | 100 (100) | 87 (87) | 13 (13) | 32 (32) | 28 (28) | 43 (43) | 31 (31) | 4 (4) | 3 (3) | 6 (6) | 3 (3) | 16 (16) | 0 (0) | 0 (0) |
| Infectious group (total) | 53 (100) | 40 (75.5) | 13 (24.5) | 19 (35.8) | 15 (28.3) | 26 (49.1) | 15 (28.3) | 2 (3.8) | 1 (1.9) | 4 (7.5) | 1 (1.9) | 6 (11.3) | 0 (0) | 0 (0) |
| Cystitis | 10 (18.9) | 9 (90) | 1 (10) | 3 (30) | 1 (10) | 5 (50) | 2 (20) | 1 (10) | 0 (0) | 1 (10) | 0 (0) | 1 (100) | 0 (0) | 0 (0) |
| Endometritis | 2 (3.8) | 2 (100) | 0 (0) | 2 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (100) | 0 (0) | 0 (0) |
| Pyelonephritis | 19 (35.8) | 10 (52.6) | 9 (47.4) | 8 (42.1) | 6 (31.6) | 9 (47.4) | 7 (36.8) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (10.5) | 0 (0) | 0 (0) |
| UTI with urosepsis | 2 (3.8) | 2 (100) | 0 (0) | 1 (50) | 1 (50) | 1 (50) | 2 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| UTI c | 20 (37.7) | 17 (85) | 3 (15) | 5 (25) | 7 (35) | 11 (55) | 4 (20) | 1 (5) | 1 (5) | 3 (15) | 1 (5) | 2 (5) | 0 (0) | 0 (0) |
| Non-infectious group (total) | 32 (100) | 32 (100) | 0 (0) | 8 (8) | 8 (8) | 11 (11) | 12 (12) | 1 (1) | 2 (2) | 2 (2) | 0 (0) | 6 (6) | 0 (0) | 0 (0) |
| ASB d | 32 (100) | 32 (100) | 0 (0) | 8 (25) | 8 (25) | 11 (34.4) | 12 (37.5) | 1 (3.1) | 2 (6.3) | 2 (6.3) | 0 (0) | 6 (18.8) | 0 (0) | 0 (0) |
| Unavailable clinical records (total) | 15 (100) | 15 (100) | 0 (0) | 5 (5) | 5 (5) | 6 (6) | 6 (6) | 1 (1) | 0 (0) | 0 (0) | 2 (2) | 4 (4) | 0 (0) | 0 (0) |
| No clin. data e | 15 (100) | 15 (100) | 0 (0) | 5 (33.3) | 5 (33.3) | 6 (40) | 6 (40) | 1 (6.7) | 0 (0) | 0 (0) | 2 (13.3) | 4 (26.7) | 0 (0) | 0 (0) |
| E. coli Serogroups | No. of Isolates (%) per Group | Distribution of Serogroups among Sex | Frequency of Resistance (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. among F (%) a | No. among M (%) b | AMP | AMC | CXM | CIP | AK | CN | TOB | F | TMP | IPM | MEM | ||
| Non-UTI associated c | 36 (100) | 29 (80.6) | 7 (19.4) | 0 (0) | 16 (44.4) | 35 (97.2) | 1 (2.8) | 2 (5.6) | 0 (0) | 5 (13.9) | 0 (0) | 3 (8.3) | 0 (0) | 0 (0) |
| UTI associated d | 64 (100) | 58 (90.3) | 6 (9.4) | 32 (50) | 12 (18.8) | 8 (12.5) | 30 (46.9) | 2 (3.1) | 3 (4.7) | 1 (1.6) | 3 (4.7) | 13 (20.3) | 0 (0) | 0 (0) |
| O2 | 1 (0.6) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | 1 (100) | 0 (0) | 0 (0) | 1 (100) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| O4 | 4 (6.2) | 3 (75) | 1 (25) | 1 (25) | 1 (25) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (25) | 0 (0) | 0 (0) | 0 (0) |
| O8 | 4 (6.2) | 4 (100) | 0 (0) | 2 (50) | 1 (25) | 0 (0) | 1 (25) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (50) | 0 (0) | 0 (0) |
| O15 | 21 (32.8) | 20 (95.2) | 1 (4.8) | 15 (71.4) | 3 (14.3) | 2 (9.5) | 12 (57.1) | 1 (4.8) | 0 (0) | 1 (4.8) | 1 (4.8) | 4 (19.0) | 0 (0) | 0 (0) |
| O16 | 3 (4.7) | 3 (100) | 0 (0) | 2 (66.7) | 0 (0) | 1 (33.3) | 2 (66.7) | 0 (0) | 1 (33.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| O18 | 4 (6.2) | 3 (75) | 1 (25) | 2 (50) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| O22 | 15 (23.4) | 13 (86.7) | 2 (13.3) | 3 (20) | 2 (13.3) | 1 (6.7) | 9 (60) | 0 (0) | 1 (6.7) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| O25 | 10 (15.6) | 10 (100) | 0 (0) | 6 (60) | 4 (40) | 2 (20) | 5 (50) | 1 (10) | 0 (0) | 0 (0) | 0 (0) | 4 (40) | 0 (0) | 0 (0) |
| O83 | 2 (3.1) | 1 (50) | 1 (50) | 1 (50) | 1 (50) | 1 (50) | 1 (50) | 0 (0) | 0 (0) | 0 (0) | 1 (50) | 1 (50) | 0 (0) | 0 (0) |
| Phylogenetic Groups | No. among F (%) a | No. among M (%) b | Total Number of Isolates per Group |
|---|---|---|---|
| Group A | 7 (8.0) | 0 (0) | 7 |
| Group B1 | 14 (16.1) | 4 (30.8) | 18 |
| Group B2 | 43 (49.4) | 7 (53.8) | 50 |
| Group D | 23 (26.4) | 2 (15.4) | 25 |
| Phylogenetic Groups | Antimicrobial Resistance Profiles | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AMP | AMC | CXM | CIP | AK | CN | TOB | F | TMP | IPM | MEM | |
| Group A | 3 (42.9) | 1 (14.3) | 4 (57.1) | 2 (28.6) | 0 (0) | 0 (0) | 1 (14.3) | 0 (0) | 2 (28.6) | 0 (0) | 0 (0) |
| Group B1 | 5 (27.8) | 4 (22.2) | 6 (33.3) | 8 (44.4) | 1 (5.6) | 0 (0) | 1 (5.6) | 0 (0) | 1 (5.6) | 0 (0) | 0 (0) |
| Group B2 | 15 (30) | 11 (22) | 20 (40) | 14 (28) | 1 (2) | 3 (6) | 2 (4) | 2 (4) | 6 (12) | 0 (0) | 0 (0) |
| Group D | 9 (36) | 12 (48) | 13 (52) | 7 (28) | 2 (8) | 0 (0) | 2 (8) | 1 (4) | 7 (28) | 0 (0) | 0 (0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prakapaite, R.; Saab, F.; Planciuniene, R.; Petraitis, V.; Walsh, T.J.; Petraitiene, R.; Semoskaite, R.; Baneviciene, R.; Kalediene, L.; Kavaliauskas, P. Molecular Characterization of Uropathogenic Escherichia coli Reveals Emergence of Drug Resistant O15, O22 and O25 Serogroups. Medicina 2019, 55, 733. https://doi.org/10.3390/medicina55110733
Prakapaite R, Saab F, Planciuniene R, Petraitis V, Walsh TJ, Petraitiene R, Semoskaite R, Baneviciene R, Kalediene L, Kavaliauskas P. Molecular Characterization of Uropathogenic Escherichia coli Reveals Emergence of Drug Resistant O15, O22 and O25 Serogroups. Medicina. 2019; 55(11):733. https://doi.org/10.3390/medicina55110733
Chicago/Turabian StylePrakapaite, Ruta, Frederic Saab, Rita Planciuniene, Vidmantas Petraitis, Thomas J. Walsh, Ruta Petraitiene, Rasa Semoskaite, Rasa Baneviciene, Lilija Kalediene, and Povilas Kavaliauskas. 2019. "Molecular Characterization of Uropathogenic Escherichia coli Reveals Emergence of Drug Resistant O15, O22 and O25 Serogroups" Medicina 55, no. 11: 733. https://doi.org/10.3390/medicina55110733