Intratumoral Cytotoxic T-Lymphocyte Density and PD-L1 Expression Are Prognostic Biomarkers for Patients with Colorectal Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Pathological Specimens
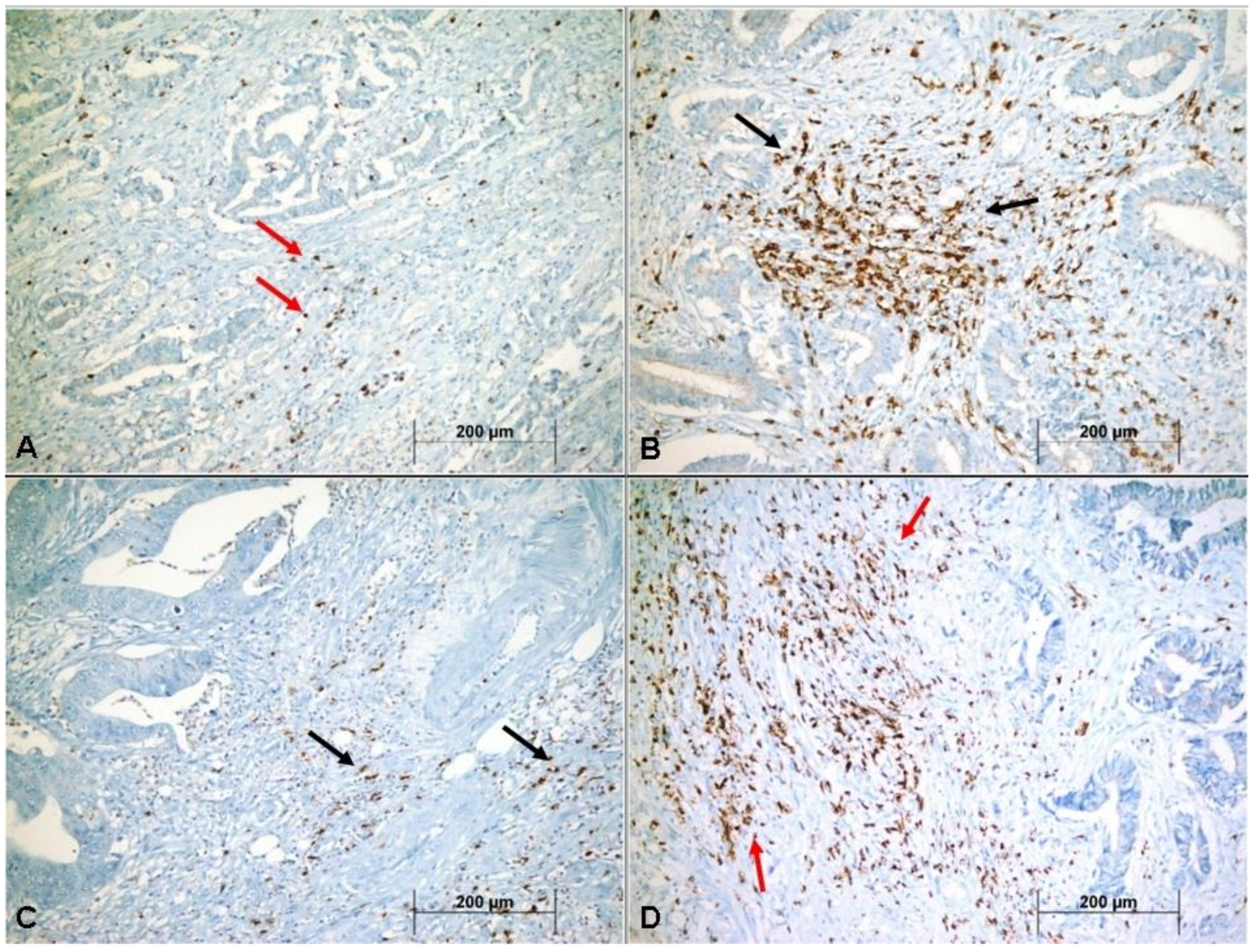
2.2. Immunohistochemistry
2.3. Scoring System for PD-L1 Expression
2.4. Scoring System for CD8+ CTLs Density
2.5. Statistical Analyses
3. Results
3.1. General Clinicopathological Features of the Cases and Their Relationship with Disease-Free Survival
3.2. Relationship of CTLs Density to Classical Clinicopathologic Features
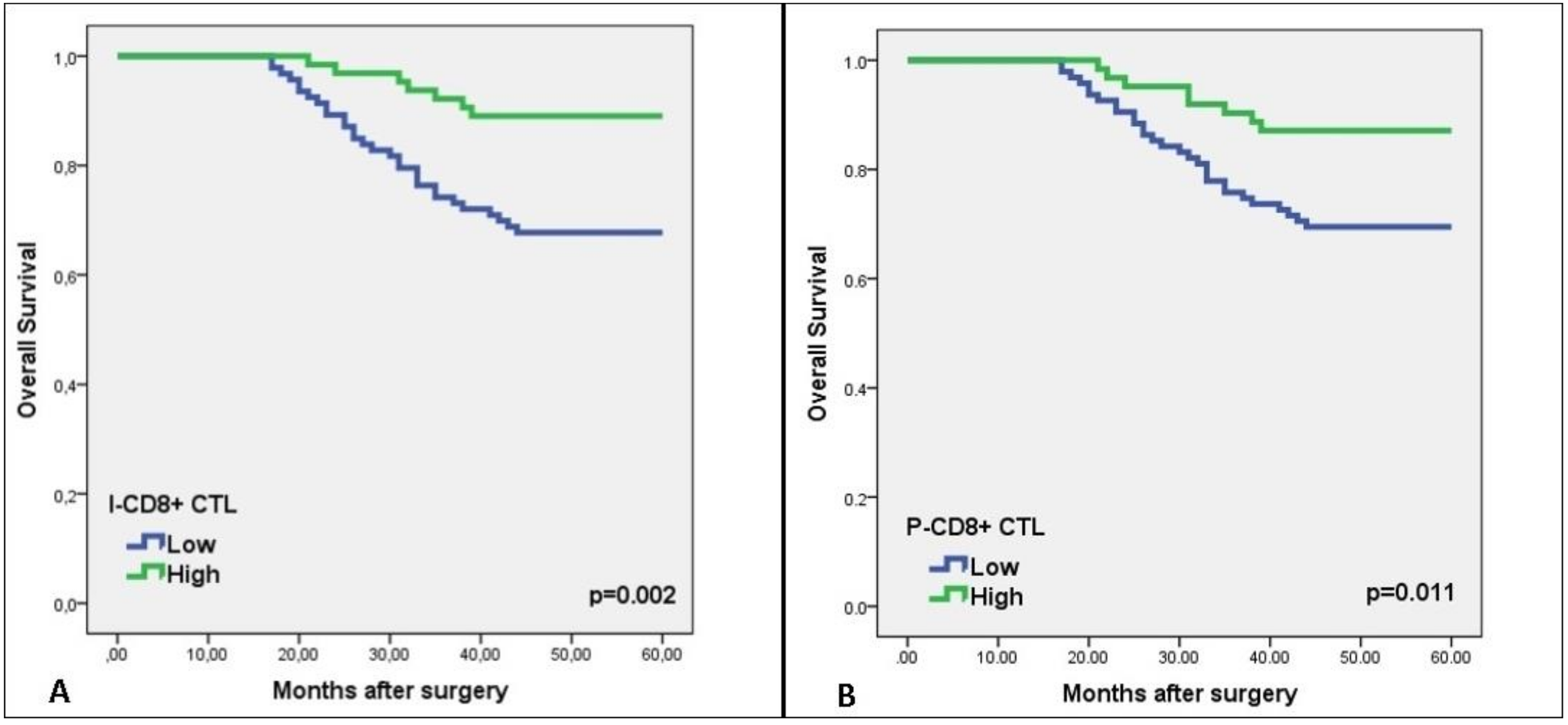
3.3. Relationship of CTLs Density to OS and DFS
3.4. Relationship of PD-L1 Expression to Classical Clinicopathological Features
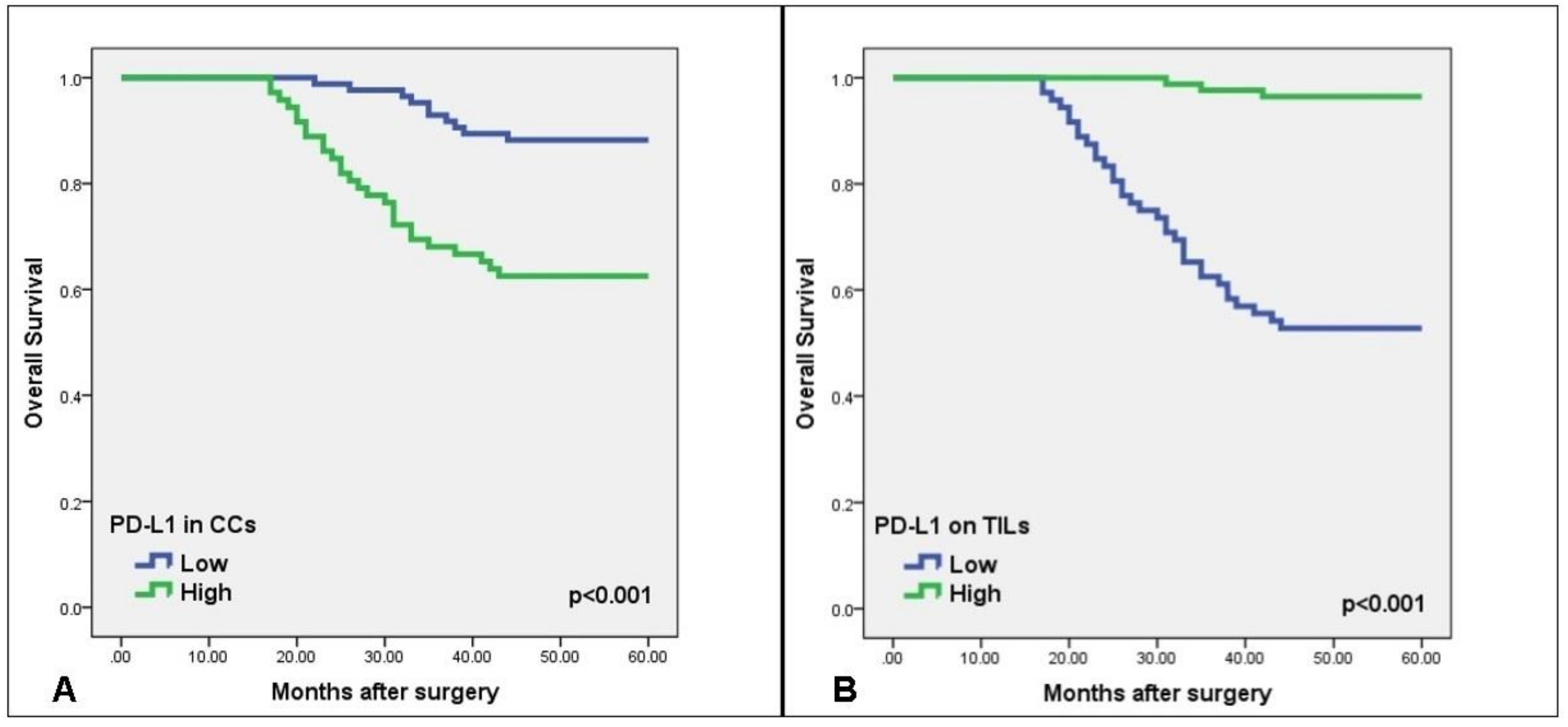
3.5. Relationship of PD-L1 Expression to OS and DFS
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dylag-Trojanowska, K.; Rogala, J.; Pach, R.; Siedlar, M.; Baran, J.; Sierzega, M.; Zybaczynska, J.; Lenart, M.; Rutkowska-Zapala, M.; Szczepanik, A.M. T Regulatory CD4+CD25+FoxP3+ Lymphocytes in the Peripheral Blood of Left-Sided Colorectal Cancer Patients. Medicina 2019, 55, 307. [Google Scholar] [CrossRef] [PubMed]
- Koganemaru, S.; Inoshita, N.; Miura, Y.; Miyama, Y.; Fukui, Y.; Ozaki, Y.; Tomizawa, K.; Hanaoka, Y.; Toda, S.; Suyama, K.; et al. Prognostic value of programmed death ligand 1 expression in patients with stage III colorectal cancer. Cancer Sci. 2017, 108, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; He, M.; Zhou, Y.; Yang, C.; Wei, S.; Bian, X.; Christopher, O.; Xie, L. The Prognostic and Clinicopathological Roles of PD-L1 Expression in Colorectal Cancer: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2019, 10, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Azer, S.A. Challenges Facing the Detection of Colonic Polyps: What Can Deep Learning Do? Medicina 2019, 55, 473. [Google Scholar] [CrossRef]
- Rosso, C.; Cabianca, L.; Gili, F.M. Non-invasive markers to detect colorectal cancer in asymptomatic population. Minerva Biotecnol. 2019, 31, 23–29. [Google Scholar] [CrossRef]
- Iseki, Y.; Shibutani, M.; Maeda, K.; Nagahara, H.; Fukuoka, T.; Matsutani, S.; Kashiwagi, S.; Tanaka, H.; Hirakawa, K.; Ohira, M. A new method for evaluating tumor-infiltrating lymphocytes (TILs) in colorectal cancer using hematoxylin and eosin (H-E)-stained tumor sections. PLoS ONE 2018, 26, e0192744. [Google Scholar] [CrossRef]
- Eriksen, A.C.; Sørensen, F.B.; Lindebjerg, J.; Hager, H.; de Pont Christensen, R.; Kjær-Frifeldt, S.; Hansen, T.F. Programmed Death Ligand-1 expression in stage II colon cancer—Experiences from a nationwide populationbased cohort. BMC Cancer 2019, 19, 142. [Google Scholar] [CrossRef]
- Tao, M.Y.; Wang, Z.H.; Zhang, M.H.; Ma, T.H.; Yang, X.Z.; Wu, S.N.; Chen, X.F.; Wang, H.G. Prognostic value of the systematic immune-inflammation index among patients with operable colon cancer: A retrospective study. Medicine 2018, 97. [Google Scholar] [CrossRef]
- Mei, Z.; Liu, Y.; Liu, C.; Cui, L. Response to comment on ‘Tumour-infiltrating inflammation and prognosis in colorectal cancer: Systematic review and meta-analysis’. Br. J. Cancer 2014, 111, 2372–2373. [Google Scholar] [CrossRef]
- Wu, B.; Zhao, S.; Sheng, Y.; Ren, L.; Song, G. The prognostic value of combining the CD8+ lymphocyte density and the circulating lymphocyte ratio in circumferential resection margin biopsy in rectal cancer. Medicine 2018, 97, e11972. [Google Scholar] [CrossRef] [PubMed]
- Trajkovski, G.; Ognjenovic, L.; Jota, G.; Hadzi-Manchev, D.; Trajkovska, V.; Volcevski, G.; Nikolova, D.; Petrushevska, G.; Janevska, V.; Janevski, V. Tumour Lymphocytic Infiltration, Its Structure and Influence in Colorectal Cancer Progression. Open Access Maced. J. Med. Sci. 2018, 6, 1003–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwak, Y.; Koh, J.; Kim, D.W.; Kang, S.B.; Kim, W.H.; Lee, H.S. Immunoscore encompassing CD3+ and CD8+ T cell densities in distant metastasis is a robust prognostic marker for advanced colorectal cancer. Oncotarget 2016, 7, 81778–81790. [Google Scholar] [CrossRef] [PubMed]
- Valentini, A.M.; Di Pinto, F.; Cariola, F.; Guerra, V.; Giannelli, G.; Caruso, M.L.; Pirrelli, M. PD-L1 expression in colorectal cancer defines three subsets of tumor immune microenvironments. Oncotarget 2018, 9, 8584–8596. [Google Scholar] [CrossRef] [PubMed]
- Inaguma, S.; Lasota, J.; Felisiak-Golabek, A.; Kowalik, A.; Wang, Z.; Zieba, S.; Kalisz, J.; Ikeda, H.; Miettinen, M. Histopathological and genotypic characterization of metastatic colorectal carcinoma with PD-L1 (CD274)-expression: Possible roles of tumour micro environmental factors for CD274 expression. J. Pathol. Clin. Res. 2017, 3, 268–278. [Google Scholar] [CrossRef]
- Chen, T.W.; Huang, K.C.; Chiang, S.F.; Chen, W.T.; Ke, T.W.; Chao, K.S.C. Prognostic relevance of programmed cell death-ligand 1 expression and CD8+ TILs in rectal cancer patients before and after neoadjuvant chemoradiotherapy. J. Cancer Res. Clin. Oncol. 2019, 145, 1043–1053. [Google Scholar] [CrossRef]
- Wu, P.; Wu, D.; Li, L.; Chai, Y.; Huang, J. PD-L1 and survival in solid tumors: A meta-analysis. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Herbst, R.S.; Soria, J.C.; Kowanetz, M.; Fine, G.D.; Hamid, O.; Gordon, M.S.; Sosman, J.A.; McDermott, D.F.; Powderly, J.D.; Gettinger, S.N.; et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 2014, 515, 563–567. [Google Scholar] [CrossRef] [Green Version]
- Deschoolmeester, V.; Baay, M.; Van Marck, E.; Weyler, J.; Vermeulen, P.; Lardon, F.; Vermorken, J.B. Tumor infiltrating lymphocytes: An intriguing player in the survival of colorectal cancer patients. BMC Immunol. 2010, 11, 19. [Google Scholar] [CrossRef]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Mazieres, J.; Planchard, D.; Stinchcombe, T.E.; Dy, G.K.; Antonia, S.J.; Horn, L.; Lena, H.; Minenza, E.; Mennecier, B.; et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): A phase 2, single-arm trial. Lancet Oncol. 2015, 16, 257–265. [Google Scholar] [CrossRef]
- Ansell, S.M.; Lesokhin, A.M.; Borrello, I.; Halwani, A.; Scott, E.C.; Gutierrez, M.; Schuster, S.J.; Millenson, M.M.; Cattry, D.; Freeman, G.J.; et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin‘s lymphoma. N. Engl. J. Med. 2015, 372, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.W.; Weber, J.S.; et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N. Engl. J. Med. 2013, 369, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (Keynote-012): An open-label, multicentre, phase 1b trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]
- Di Caro, G.; Marchesi, F.; Laghi, L.; Grizzi, F. Immune cells: Plastic players along colorectal cancer progression. J. Cell Mol. Med. 2013, 17, 1088–1095. [Google Scholar] [CrossRef]
- Mlecnik, B.; Bindea, G.; Angell, H.K.; Maby, P.; Angelova, M.; Tougeron, D.; Church, S.E.; Lafontaine, L.; Fischer, M.; Fredriksen, T.; et al. Integrative analyses of colorectal cancer show immunoscore is a stronger predictor of patient survival than microsatellite instability. Immunity 2016, 44, 698–711. [Google Scholar] [CrossRef]
- Zlobec, I.; Karamitopoulou, E.; Terracciano, L.; Piscuoglio, S.; Iezzi, G.; Muraro, M.G.; Spagnoli, G.; Baker, K.; Tzankov, A.; Lugli, A. TIA-1 cytotoxic granule-associated RNAbinding protein improves the prognostic performance of CD8 in mismatch repair-proficient colorectal cancer. PLoS ONE 2010, 5, e14282. [Google Scholar] [CrossRef]
- Klintrup, K.; Makinen, J.M.; Kauppila, S.; Vare, P.O.; Melkko, J.; Tuominen, H.; Tuppurainen, K.; Mäkelä, J.; Karttunen, T.J.; Mäkinen, M.J. Inflammation and prognosis in colorectal cancer. Eur. J. Cancer 2005, 41, 2645–2654. [Google Scholar] [CrossRef]
- Huh, J.W.; Lee, J.H.; Kim, H.R. Prognostic significance of tumor-infiltrating lymphocytes for patients with colorectal cancer. Arch. Surg. 2012, 147, 366–371. [Google Scholar] [CrossRef]
- Väyrynen, J.P.; Sajanti, S.A.; Klintrup, K.; Mäkelä, J.; Herzig, K.H.; Karttunen, T.J.; Tuomisto, A.; Mäkinen, M.J. Characteristics and significance of colorectal cancer associated lymphoid reaction. Int. J. Cancer 2014, 134, 2126–2135. [Google Scholar] [CrossRef]
- Lee, K.S.; Kwak, Y.; Ahn, S.; Shin, E.; Oh, H.K.; Kim, D.W.; Kang, S.B.; Choe, G.; Kim, W.H.; Lee, H.S. Prognostic implication of CD274 (PD-L1) protein expression in tumor-infiltrating immune cells for microsatellite unstable and stable colorectal cancer. Cancer Immunol. Immunother. 2017, 66, 927–939. [Google Scholar] [CrossRef] [PubMed]
- Ohaegbulam, K.C.; Assal, A.; Lazar-Molnar, E.; Yao, Y.; Zang, X. Human cancer immunotherapy with antibodies to the PD-1 and PD-L1 pathway. Trends Mol. Med. 2015, 21, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.U.; Jeong, W.K.; Baek, S.K.; Kim, N.K.; Hwang, I. Prognostic impact of programmed cell death ligand 1 expression on long-term oncologic outcomes in colorectal cancer. Oncol. Lett. 2018, 16, 5214–5222. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Chiang, S.F.; Ke, T.W.; Chen, T.W.; You, Y.S.; Chen, W.T.; Chao, K.S.C. Clinical significance of programmed death 1 ligand-1 (CD274/PD-L1) and intra-tumoral CD8+ T-cell infiltration in stage II-III colorectal cancer. Sci. Rep. 2018, 8, 15658. [Google Scholar] [CrossRef] [PubMed]
- Spranger, S.; Spaapen, R.M.; Zha, Y.; Williams, J.; Meng, Y.; Ha, T.T.; Gajewski, T.F. Up-regulation of PD-L1, IDO, and T(regs) in the melanoma tumor microenvironment is driven by CD8(+) T cells. Sci. Transl. Med. 2013, 5, 200ra116. [Google Scholar] [CrossRef] [PubMed]
- Masugi, Y.; Nishihara, R.; Yang, J.; Mima, K.; da Silva, A.; Shi, Y.; Inamura, K.; Cao, Y.; Song, M.; Nowak, J.A. Tumour CD274 (PD-L1) expression and T cells in colorectal cancer. Gut 2017, 66, 1463–1473. [Google Scholar] [CrossRef] [PubMed]
- Droeser, R.A.; Hirt, C.; Viehl, C.T.; Frey, D.M.; Nebiker, C.; Huber, X.; Zlobec, I.; Eppenberger-Castori, S.; Tzankov, A.; Rosso, R.; et al. Clinical impact of programmed cell death ligand 1 expression in colorectal cancer. Eur. J. Cancer 2013, 49, 2233–2242. [Google Scholar] [CrossRef]
- Lee, L.H.; Cavalcanti, M.S.; Segal, N.H.; Hechtman, J.F.; Weiser, M.R.; Smith, J.J.; Garcia-Aguilar, J.; Sadot, E.; Ntiamoah, P.; Markowitz, A.J.; et al. Patterns and prognostic relevance of PD-1 and PD-L1 expression in colorectal carcinoma. Mod. Pathol. 2016, 29, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Dunne, P.D.; McArt, D.G.; O’Reilly, P.G.; Coleman, H.G.; Allen, W.L.; Loughrey, M.; Van Schaeybroeck, S.; McDade, S.; Salto Tellez, M.; Longley, D.B.; et al. Immune-derived PD-L1 gene expression defines a subgroup of stage II/III colorectal cancer patients with favorable prognosis who may be harmed by adjuvant chemotherapy. Cancer Immunol. Res. 2016, 4, 582–591. [Google Scholar] [CrossRef]
- Wang, L.; Ren, F.; Wang, Q.; Baldridge, L.A.; Monn, M.F.; Fisher, K.W.; Sheng, W.; Zhou, X.; Du, X.; Cheng, L. Signifcance of programmed death ligand 1 (PD-L1) immunohistochemical expression in colorectal cancer. Mol. Diagn. Ther. 2016, 20, 175–181. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recurrence n (%) | Cox Regression (Univariate) | |||||
|---|---|---|---|---|---|---|
| n (%) | Absent n (%) | Present n (%) | HR | 95% CI | p-Value | |
| Sex | ||||||
| Male | 97 (61.8) | 59 (60.8) | 38 (39.2) | 0.82 | 0.48–1.42 | 0.497 |
| Female | 60 (38.2) | 40 (66.7) | 20 (33.3) | |||
| Age (median 60) | ||||||
| (range 19–90) | ||||||
| 19–44 | 25 (15.9) | 21 (84.0) | 4 (16.0) | 3.14 | 1.12–8.84 | 0.029 |
| 45–54 | 50 (31.8) | 33 (66.0) | 17 (34.0) | |||
| ≥55 | 82 (52.2) | 45 (54.9) | 37 (45.1) | |||
| Tumor site | ||||||
| Right side | 43 (27.4) | 20 (46.5) | 23 (53.5) | 0.5 | 0.29–0.84 | 0.01 |
| Left side | 114 (72.6) | 79 (69.3) | 35 (30.7) | |||
| Tumor size | ||||||
| <5 cm | 61 (38.9) | 41 (67.2) | 20 (32.8) | 1.3 | 0.75–2.24 | 0.342 |
| ≥5 cm | 96 (61.1) | 58 (60.4) | 38 (39.6) | |||
| Histopathologic type | ||||||
| Adenocarcinoma | 99 (63.1) | 69 (69.7) | 30 (30.3) | 0.38 | 0.18–0.80 | 0.012 |
| Mucinous | 38 (24.2) | 21 (55.3) | 17 (44.7) | |||
| Signet-ring | 20 (12.7) | 9 (45.0) | 11 (55.0) | |||
| Histologic grade | ||||||
| Well | 25 (15.9) | 16 (64.0) | 9 (36.0) | 0.58 | 0.29–1.13 | 0.114 |
| Moderate | 109 (69.4) | 71 (65.1) | 38 (34.9) | |||
| Poor | 23 (14.6) | 12 (52.2) | 11 (47.8) | |||
| Depth of invasion | ||||||
| pT1 | 26 (16.6) | 20 (76.9) | 6 (23.1) | 0.42 | 0.24–0.75 | 0.004 |
| pT2 | 64 (40.8) | 46 (71.9) | 18 (28.1) | |||
| pT3 | 67 (42.7) | 33 (49.3) | 34 (50.7) | |||
| Lymph node status | ||||||
| Absent | 91 (58.0) | 67 (73.6) | 24 (26.4) | 0.51 | 0.25–1.02 | 0.008 |
| 1–3 | 34 (21.7) | 12 (35.3) | 22 (64.7) | |||
| ≥4 | 32 (20.4) | 20 (62.5) | 12 (37.5) | |||
| Distant Metastasis | ||||||
| Absent | 123 (78.3) | 90 (73.2) | 33 (26.8) | 0.15 | 0.09–0.27 | <0.001 |
| Present | 34 (21.7) | 9 (26.5) | 25 (73.5) | |||
| TNM staging | ||||||
| Stage I | 18 (11.5) | 13 (72.2) | 5 (27.8) | 0.14 | 0.22–0.84 | <0.001 |
| Stage II | 40 (25.5) | 33 (82.5) | 7 (12.5) | |||
| Stage III | 80 (50.9) | 46 (57.5) | 34 (42.5) | |||
| Stage IV | 19 (12.1) | 7 (36.8) | 12 (63.2) | |||
| I-CD8+ CTLs Density | P-CD8+ CTLs Density | |||||
|---|---|---|---|---|---|---|
| Low n (%) | High n (%) | p-Value | Low n (%) | High n (%) | p-Value | |
| Sex | ||||||
| Male | 60 (61.9) | 37 (38.1) | 0.442 † | 62 (63.9) | 35 (36.1) | 0.270 † |
| Female | 33 (55.0) | 27 (45.5) | 33 (55.0) | 27 (45.5) | ||
| Age (median 60) | ||||||
| (range 19–90) | ||||||
| 19–44 | 15 (60.0) | 10 (40.0) | 0.992 ‡ | 14 (56.0) | 11 (44.0) | 0.856 ‡ |
| 45–54 | 29 (58.0) | 21 (42.0) | 30 (60.0) | 20 (40.0) | ||
| ≥55 | 49 (59.8) | 33 (40.2) | 51 (62.2) | 31 (37.8) | ||
| Tumor site | ||||||
| Right side | 27 (62.8) | 16 (37.2) | 0.147 † | 28 (65.1) | 15 (35.9) | 0.472 † |
| Left side | 66 (57.9) | 48 (42.1) | 67 (58.8) | 47 (41.2) | ||
| Tumor size | ||||||
| <5 cm | 34 (56.7) | 26 (43.3) | 0.663 † | 32 (53.3) | 28 (46.7) | 0.150 † |
| ≥5 cm | 59 (60.8) | 38 (39.2) | 63 (64.9) | 34 (35.1) | ||
| Histopathologic type | ||||||
| Adenocarcinoma | 55 (55.6) | 44 (44.4) | 0.055 ‡ | 55 (55.5) | 44 (44.4) | 0.117 ‡ |
| Mucinous | 21 (55.3) | 17 (44.7) | 24 (63.2) | 14 (36.8) | ||
| Signet-ring | 17 (85.0) | 3 (15.0) | 16 (80.0) | 4 (20.0) | ||
| Histologic grade | ||||||
| Well | 14 (56.0) | 11 (44.0) | 0.884 ‡ | 14 (56.0) | 11 (44.0) | 0.600 ‡ |
| Moderate | 64 (58.7) | 45 (41.3) | 65 (59.6) | 44 (40.4) | ||
| Poor | 15 (65.2) | 8 (34.8) | 16 (69.6) | 7 (30.4) | ||
| Depth of invasion | ||||||
| pT1 | 9 (34.6) | 17 (65.4) | 0.011‡ | 12 (46.2) | 14 (53.8) | 0.016 ‡ |
| pT2 | 38 (59.4) | 26 (40.6) | 34 (53.1) | 30 (46.9) | ||
| pT3 | 46 (68.7) | 21 (31.3) | 49 (73.1) | 18 (26.9) | ||
| Node status | ||||||
| Absent | 53 (58.2) | 38 (41.8) | 0.696 ‡ | 54 (59.3) | 37 (40.7) | 0.939 ‡ |
| 1–3 | 19 (55.9) | 15 (44.1) | 21 (61.8) | 13 (38.2) | ||
| ≥4 | 21 (65.6) | 11 (34.4) | 20 (62.5) | 12 (37.5) | ||
| Distant Metastasis | ||||||
| Absent | 66 (53.7) | 57 (46.3) | 0.007 † | 70 (56.9) | 53 (43.1) | 0.037 † |
| Present | 27 (79.4) | 7 (20.6) | 25 (73.5) | 9 (26.5) | ||
| TNM staging | ||||||
| Stage I | 9 (50.0) | 9 (50.0) | 0.512 ‡ | 11 (61.1) | 7 (38.9) | 0.486 ‡ |
| Stage II | 23 (57.5) | 17 (42.5) | 21 (52.5) | 19 (47.5) | ||
| Stage III | 47 (58.8) | 33 (41.2) | 49 (61.2) | 31 (38.8) | ||
| Stage IV | 14 (73.7) | 5 (26.3) | 14 (73.7) | 5 (26.3) | ||
| Parameters | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| I-CD8+ CTLs density | 0.41 (0.23–0.75) | 0.004 | 2.06 (1.01–4.23) | 0.043 |
| P-CD8+ CTLs density | 0.39 (0.23–0.66) | 0.001 | 0.76 (0.38–1.53) | 0.459 |
| PD-L1 in CCs | 2.55 (1.50–4.34) | 0.001 | 0.48 (0.28–0.82) | 0.007 |
| PD-L1 on TILs | 0.25 (0.14–0.44) | <0.001 | 3.42 (1.95–6.01) | <0.001 |
| Parameters | PD-L1 Expression in CCs | PD-L1 Expression on TILs | ||||
|---|---|---|---|---|---|---|
| Low n (%) | High n (%) | p-Value | Low n (%) | High n (%) | p-Value | |
| Sex | ||||||
| Male | 49 (50.5) | 48 (49.5) | 0.249 † | 46 (47.4) | 51 (52.6) | 0.620 † |
| Female | 36 (60.0) | 24 (40.0) | 26 (43.3) | 34 (56.7) | ||
| Age (median 60) | ||||||
| (range 19–90) | ||||||
| 19–44 | 16 (64.0) | 9 (36.0) | 0.333 ‡ | 10 (40.0) | 15 (60.0) | 0.803 ‡ |
| 45–54 | 29 (58.0) | 21 (42.0) | 24 (48.0) | 26 (52.0) | ||
| ≥55 | 40 (48.8) | 42 (51.2) | 38 (46.3) | 44 (53.7) | ||
| Tumor site | ||||||
| Right side | 24 (55.8) | 19 (44.2) | 0.798 † | 21 (48.8) | 22 (51.2) | 0.648 † |
| Left side | 61 (53.5) | 53 (46.5) | 51 (44.7) | 63 (55.3) | ||
| Tumor size | ||||||
| <5 cm | 37 (61.7) | 23 (38.3) | 0.138† | 25 (41.7) | 35 (58.3) | 0.410 † |
| ≥5 cm | 48 (49.5) | 49 (50.5) | 47 (48.5) | 50 (51.5) | ||
| Histopathologic type | ||||||
| Adenocarcinoma | 57 (57.6) | 42 (42.4) | <0.001 ‡ | 38 (38.4) | 61 (61.6) | 0.038 ‡ |
| Mucinous | 25 (65.8) | 13 (34.2) | 21 (55.3) | 17 (44.7) | ||
| Signet-ring | 3 (15.0) | 17 (85.0) | 13 (65.0) | 7 (35.0) | ||
| Histologic grade | ||||||
| Well | 15 (60.0) | 10 (40.0) | 0.704 ‡ | 10 (40.0) | 15 (60.0) | 0.493 ‡ |
| Moderate | 59 (54.1) | 50 (45.9) | 49 (45.0) | 60 (55.0) | ||
| Poor | 11 (47.8) | 12 (52.2) | 13 (56.5) | 10 (43.5) | ||
| Depth of invasion | ||||||
| pT1 | 22 (84.6) | 4 (15.4) | <0.001 ‡ | 7 (26.9) | 19 (73.1) | 0.026 ‡ |
| pT2 | 41 (64.1) | 23 (35.9) | 27 (42,2) | 37 (57.8) | ||
| pT3 | 22 (32.8) | 45 (67.2) | 38 (56.7) | 29 (43.3) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calik, I.; Calik, M.; Turken, G.; Ozercan, I.H.; Dagli, A.F.; Artas, G.; Sarikaya, B. Intratumoral Cytotoxic T-Lymphocyte Density and PD-L1 Expression Are Prognostic Biomarkers for Patients with Colorectal Cancer. Medicina 2019, 55, 723. https://doi.org/10.3390/medicina55110723
Calik I, Calik M, Turken G, Ozercan IH, Dagli AF, Artas G, Sarikaya B. Intratumoral Cytotoxic T-Lymphocyte Density and PD-L1 Expression Are Prognostic Biomarkers for Patients with Colorectal Cancer. Medicina. 2019; 55(11):723. https://doi.org/10.3390/medicina55110723
Chicago/Turabian StyleCalik, Ilknur, Muhammet Calik, Gulistan Turken, Ibrahim Hanifi Ozercan, Adile Ferda Dagli, Gokhan Artas, and Burcu Sarikaya. 2019. "Intratumoral Cytotoxic T-Lymphocyte Density and PD-L1 Expression Are Prognostic Biomarkers for Patients with Colorectal Cancer" Medicina 55, no. 11: 723. https://doi.org/10.3390/medicina55110723