The Clinical Importance of Cystatin C and Hepatic Artery Resistive Index in Liver Cirrhosis

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biochemistry
2.2. Abdominal Doppler Ultrasonography
2.3. Upper Endoscopy
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Asrani, S.K.; Larson, J.J.; Yawn, B.; Therneau, T.M.; Kim, W.R. Underestimation of liver-related mortality in the United States. Gastroenterology 2013, 145, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawy, A.M.; Oakley, F.; Mann, D.A. The role and regulation of hepatic stellate cell apoptosis in reversal of liver fibrosis. Apoptosis 2005, 10, 927–939. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Bosch, J.; Blei, A.; Arroyo, V. Portal hypertension and its complications. Gastroenterology 2008, 134, 1715–1728. [Google Scholar] [CrossRef] [PubMed]
- Schuppan, D.; Afdhal, N.H. Liver cirrhosis. Lancet 2008, 371, 838–851. [Google Scholar] [CrossRef]
- Chu, S.C.; Wang, C.P.; Chang, Y.H.; Hsieh, Y.S.; Yang, S.F.; Su, J.M.; Yang, C.C.; Chiou, H.L. Increased cystatin C serum concentrations in patients with hepatic diseases of various severities. Clin. Chim. Acta 2004, 341, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Gressner, A.M.; Lahme, B.; Meurer, S.K.; Gressner, O.; Weiskirchen, R. Variable expression of cystatin C in cultured trans-differentiating rat hepatic stellate cells. World J. Gastroenterol. 2006, 12, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Jiborn, T.; Abrahamson, M.; Wallin, H.; Malm, J.; Lundwall, A.; Gadaleanu, V.; Abrahamsson, P.A.; Bjartell, A. Cystatin C is highly expressed in the human male reproductive system. J. Androl. 2004, 25, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Fukuda, Y.; Nakano, I.; Katano, Y.; Hayakawa, T. Elevation of serum cystatin C concentrations in patients with chronic liver disease. Eur. J. Gastroenterol. Hepatol. 2001, 13, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Piscaglia, F.; Gaiani, S.; Calderoni, D.; Donati, G.; Celli, N.; Gramantieri, L.; Crespi, C.; Bolondi, L. Influence of liver fibrosis on hepatic artery Doppler resistance index in chronic hepatitis of viral origin. Scand. J. Gastroenterol. 2001, 36, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Child, C.G.; Turcotte, J.G. Surgery and portal hypertension. Major Probl. Clin. Surg. 1964, 1, 1–85. [Google Scholar] [PubMed]
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic encephalopathy—Definition, nomenclature, diagnosis, and quantification: Final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Shankar, R.; Shetty, G.S.; Srinath, M.G.; Kulkarni, R. Estimation of portal vein diameter in correlation with the age, sex and height of an individual. Anat. Karnataka 2011, 5, 13–16. [Google Scholar]
- Wood, M.M.; Romine, L.E.; Lee, Y.K.; Richman, K.M.; O’Boyle, M.K.; Paz, D.A.; Chu, P.K.; Pretorius, D.H. Spectral Doppler signature waveforms in ultrasonography: A review of normal and abnormal waveforms. Ultrasound Q. 2010, 26, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Paquet, K.J. Prophylactic endoscopic sclerosing treatment of the esophageal wall in varices—A prospective controlled randomized trial. Endoscopy 1982, 14, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Culafic, D.; Stulic, M.; Obrenovic, R.; Miletic, D.; Mijac, D.; Stojkovic, M.; Jovanović, M.; Ćulafić, M. Role of cystatin C and renal resistive index in assessment of renal function in patients with liver cirrhosis. World J. Gastroenterol. 2014, 20, 6573–6579. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Bosch, J. Management of varices and variceal hemorrhage in cirrhosis. N. Engl. J. Med. 2010, 362, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Kok, T.; van der Jagt, E.J.; Haagsma, E.B.; Bijleveld, C.M.; Jansen, P.L.; Boeve, W.J. The value of Doppler ultrasound in cirrhosis and portal hypertension. Scand. J. Gastroenterol. Suppl. 1999, 230, 82–88. [Google Scholar] [PubMed]
- Bolognesi, M.; Sacerdoti, D.; Merkel, C.; Bombonato, G.; Gatta, A. Noninvasive grading of the severity of portal hypertension in cirrhotic patients by echo-color-Doppler. Ultrasound Med. Biol. 2001, 27, 901–907. [Google Scholar] [CrossRef]
- Shateri, K.; Mohammadi, A.; Moloudi, F.; Nosair, E.; Ghasemi-Rad, M. Correlation Between Sonographic Portal Vein Diameter and Flow Velocity With the Clinical Scoring Systems MELD and CTP in Cirrhotic Patients: Is There a Relationship? Gastroenterol. Res. 2012, 5, 112–119. [Google Scholar] [CrossRef]
- Plestina, S.; Pulanic, R.; Kralik, M.; Plestina, S.; Samarzija, M. Color Doppler ultrasonography is reliable in assessing the risk of esophageal variceal bleeding in patients with liver cirrhosis. Wien. Klin. Wochenschr. 2005, 117, 711–777. [Google Scholar] [CrossRef] [PubMed]
- Zardi, E.M.; Uwechie, V.; Gentilucci, U.V.; Dobrina, A.; Petitti, T.; Laghi, V.; Picardi, A.; Afeltra, A. Portal diameter in the diagnosis of esophageal varices in 266 cirrhotic patients: Which role? Ultrasound Med. Biol. 2007, 33, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Arjmand, S.A.; Nikoukar, E.; Bakhshandeh, H. Hepatic Doppler Ultrasound in Assessment of the Severity of Esophageal Varices in Cirrhotic Patients. Iran J. Radiol. 2007, 4, 151–158. [Google Scholar]
- Haktanir, A.; Cihan, B.S.; Celenk, C.; Cihan, S. Value of Doppler sonography in assessing the progression of chronic viral hepatitis and in the diagnosis and grading of cirrhosis. J. Ultrasound Med. 2005, 24, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.; Khanna, S.K.; Sundas, A.; Rauniyar, R.K.; Koirala, R.; Gupta, M.K. Duplex Sonographic Evaluation of Hepatic Vasculature in Cirrhosis. Nepal. J. Med. Sci. 2013, 2, 13–19. [Google Scholar] [CrossRef]
- Vassiliades, V.G.; Ostrow, T.D.; Chezmar, J.L.; Hertzler, G.L.; Nelson, R.C. Hepatic arterial resistive indices: Correlation with the severity of cirrhosis. Abdom. Imaging 1993, 18, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L. Mechanisms of hepatic fibrogenesis. Gastroenterology 2008, 134, 1655–1669. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.P.; Sukhova, G.K.; Grubb, A.; Ducharme, A.; Rhode, L.H.; Lee, R.T.; Ridker, P.M.; Libby, P.; Chapman, H.A. Cystatin C deficiency in human atherosclerosis and aortic aneurysms. J. Clin. Investig. 1999, 104, 1191–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuman, M.G.; Benhamou, J.P.; Marcellin, P.; Valla, D.; Malkiewicz, I.M.; Katz, G.G.; Trepo, C.; Bourliere, M.; Cameron, R.G.; Cohen, L. Cytokine—Chemokine and apoptotic signatures in patients with hepatitis, C. Transl. Res. 2007, 149, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Ladero, J.M.; Cardenas, M.C.; Ortega, L.; Gonzalez-Pino, A.; Cuenca, F.; Morales, C.; Lee-Brunner, A. Serum cystatin C: A non-invasive marker of liver fibrosis or of current liver fibrogenesis in chronic hepatitis C? Ann. Hepatol. 2012, 11, 648–651. [Google Scholar] [PubMed]
- Ahn, H.S.; Kim, Y.S.; Kim, S.G.; Kim, H.K.; Min, S.K.; Jeong, S.W.; Jang, J.Y.; Lee, S.H.; Kim, H.S.; Kim, B.S. Cystatin C is a good predictor of hepatorenal syndrome and survival in patients with cirrhosis who have normal serum creatinine levels. Hepato-gastroenterology 2012, 59, 1168–1173. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Group | Control Group | p Value | |
|---|---|---|---|
| Age, mean ± SD, years | 50.8 ± 13.5 | 48.2 ± 17.6 | 0.434 a |
| Males, n (%) | 47 (74.6) | 24 (80) | 0.567 b |
| VPD, mean ± SD, mm | 13.51 ± 3.02 | 10.55 ± 0.96 | <0.001 a |
| VP BFV, mean ± SD, cm/s | 26.48 ± 8.38 | 34.25 ± 5.48 | <0.001 a |
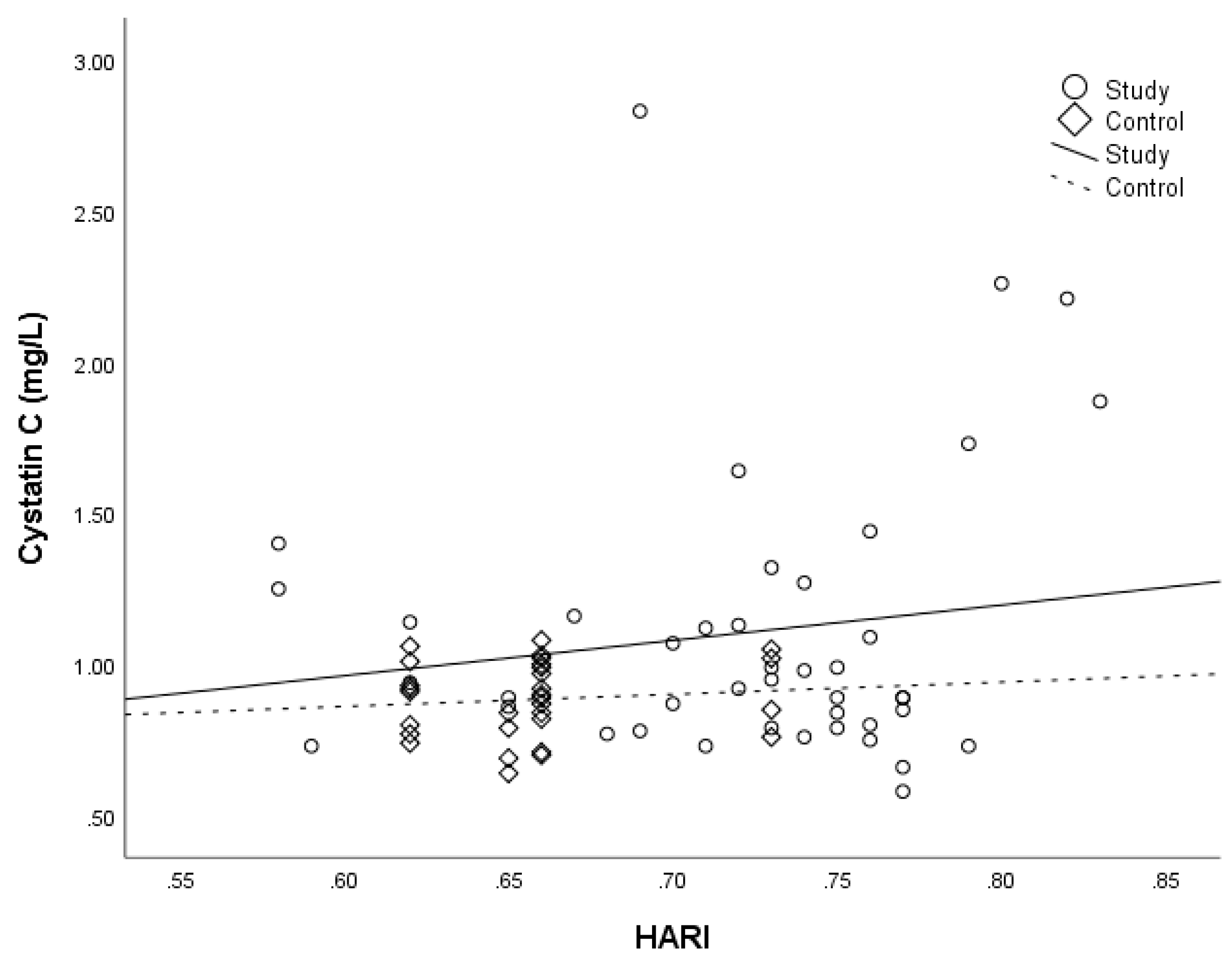
| HARI, mean ± SD | 0.72 ± 0.06 | 0.66 ± 0.03 | <0.001 a |
| CysC, median (25–75th percentile), mg/L | 0.97 (0.80–1.20) | 0.90 (0.79–1.00) | 0.036 c |
| CysC | ||||
|---|---|---|---|---|
| Study Group | Control Group | |||
| rs | p | rs | p | |
| VPD | 0.052 | 0.741 | 0.270 | 0.149 |
| VP BFV | −0.242 | 0.123 | –0.071 | 0.710 |
| HARI | 0.268 | 0.038 | 0.175 | 0.356 |
| Area (95% CI) | p Value | Cut off Value | Sn | Sp | PPV | NPV | Accuracy | ||
|---|---|---|---|---|---|---|---|---|---|
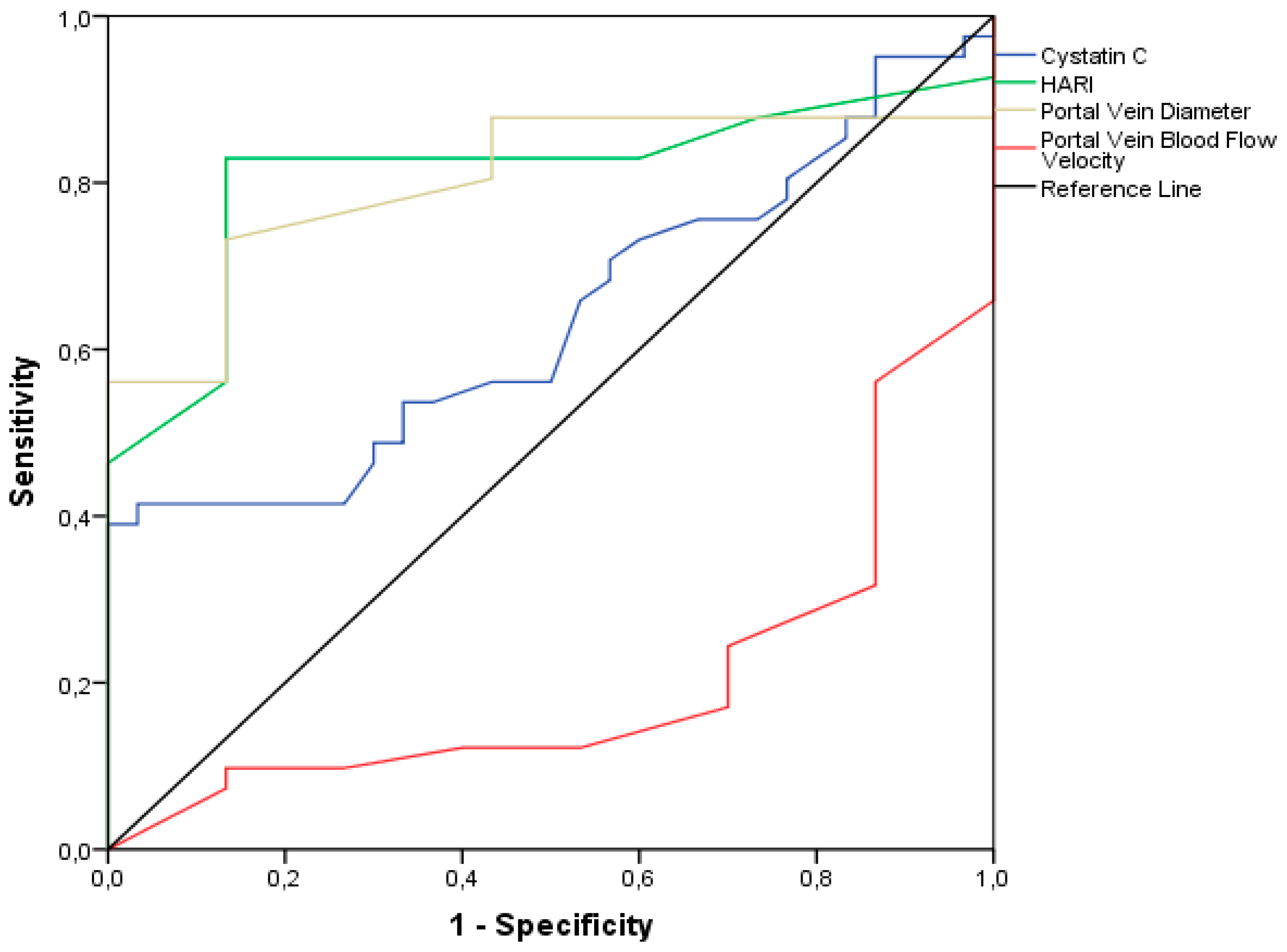
| CysC | 0.637 (0.509–0.765) | 0.050 | 1.085 | 38.3 | 100 | 100 | 44.7 | 58.5 | |
| HARI | 0.810 (0.703–0.917) | <0.001 | 0.665 | 83.7 | 86.7 | 90.0 | 78.8 | 84.9 | |
| VPD | 0.803 (0.695–0.910) | <0.001 | 11.2 | 73.8 | 86.6 | 88.6 | 70.3 | 79.2 | |
| VP BFV | 0.799 (0.693–0.904) | <0.001 | 29.5 | 66.6 | 86.6 | 87.5 | 65.0 | 75.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stulic, M.; Culafic, D.; Obrenovic, R.; Jankovic, G.; Alempijevic, T.; Lalosevic, M.S.; Dostanic, N.; Kovacevic, S.V.; Culafic, M. The Clinical Importance of Cystatin C and Hepatic Artery Resistive Index in Liver Cirrhosis. Medicina 2018, 54, 37. https://doi.org/10.3390/medicina54030037
Stulic M, Culafic D, Obrenovic R, Jankovic G, Alempijevic T, Lalosevic MS, Dostanic N, Kovacevic SV, Culafic M. The Clinical Importance of Cystatin C and Hepatic Artery Resistive Index in Liver Cirrhosis. Medicina. 2018; 54(3):37. https://doi.org/10.3390/medicina54030037
Chicago/Turabian StyleStulic, Milos, Djordje Culafic, Radmila Obrenovic, Goran Jankovic, Tamara Alempijevic, Milica Stojkovic Lalosevic, Natasa Dostanic, Sandra Vezmar Kovacevic, and Milica Culafic. 2018. "The Clinical Importance of Cystatin C and Hepatic Artery Resistive Index in Liver Cirrhosis" Medicina 54, no. 3: 37. https://doi.org/10.3390/medicina54030037