1. Introduction
Scientists have been interested in the global construct of emotional intelligence (EI) for three decades, but even today there is no accepted unanimous model of EI. However, the following fundamental dimensions of EI are observed at the intersection of various viewpoints: the ability to understand one’s own emotions and those of other people, and the ability to use this understanding to control one’s own and other people’s emotions and behavior, as well as resolve emotion-related social situations [
1,
2]. Many scientists regard each of the mentioned areas as developing since early childhood rather than being genetically predetermined. For example, the ability to perceive basic emotions reflected in a face develops before the ability to recognize feigned emotional expressions [
1]. Therefore, as abilities in one area develop and grow (e.g., perception of emotions), abilities in other areas are also developing and getting stronger (e.g., control of emotions).
When the construct of EI was introduced, two viewpoints quickly emerged. The first, originated by Mayer and Salovey, is considered a classical viewpoint that regards EI as a set of abilities that suppose a new form of intelligence [
1]. Scientists belonging to this classical movement consider EI as intelligence that operates using emotional information [
3]. It should be noted that cognitive treatment of EI developed from theory to empiricism. The second, more recent movement views EI as a dimension of a personality attributable to traits describing emotions of a person [
4]. This latter approach to EI, contrary to the classical perspective, was developed conversely; that is, data obtained in the empirical research was theorized. The Baron model is one of the most prominent representations of this approach [
5]. This model views EI as all non-cognitive abilities, knowledge, and competencies that allow a person to successfully handle various life situations. The dispute between scientists over the nature of EI is still active [
6,
7,
8], but efforts to combine these two approaches emerge through the development of new EI models [
9], and such models have both a theoretical and practical significance.
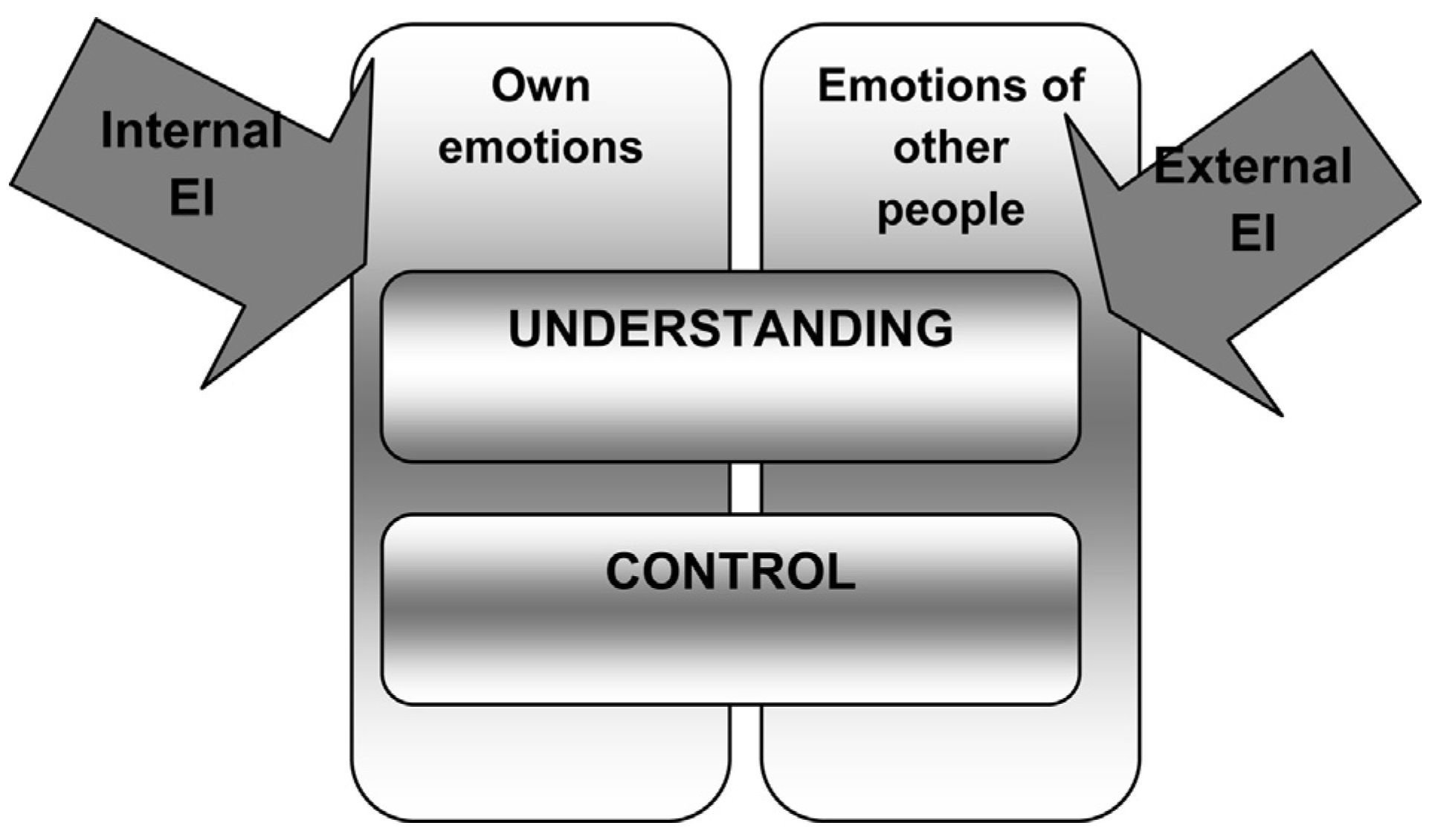
Since there are no convincing data that give priority to one EI approach, a discussion of theoretical personality-based and cognitive EI approaches and related methodologies were integrated in this study. Thus, in the present study, EI is defined as both internal (when individuals are capable of understanding and controlling their own emotions) and external (when individuals are capable of understanding and controlling emotions of other people) (see
Fig. 1).
Recently, an increasing number of interdisciplinary studies have been conducted on psychological health, good physical state, and high-quality interpersonal relationships within the context of cognitive and emotional processes [
10]. The relationship between emotional and cognitive information processing and dysfunctional thinking has been explored. Dysfunctional thinking is defined as excessive concentration on negative feelings, as well as the causes and effects of such feelings. Dysfunctional thinking is a way of responding to a problem that encompasses continuously repeating and passive concentration on stress symptoms as well as possible causes and effects of such symptoms [
11]. Concentration on problems, a depressive state, and other components of negative personal experiences determines poor adjustment and dysfunctional consequences [
12].
Results of various studies show that individuals with higher EI are of better psychological health [
13,
14], are more physically active [
15], and are more satisfied with their lives [
16]. The importance of EI on the quality of psychological health becomes evident as early as adolescence: Teens with higher EI employ more pro-active strategies rather than avoidant strategies, which often cause harm to mental health [
17]. EI also reduces the probability of negative mood dominance [
18]. EI is negatively related with levels of stress and depressive moods [
16,
19,
20].
Various studies have shown that individuals who are able to restore their emotional balance faster are distinguished by better emotional adaptation, stronger psychological health, and lower levels of depressiveness [
21]. Conversely, depressive individuals are distinguished by selective emotional attention for negative emotional stimuli like angry faces, depressive or ill-mood comments, or negative partner responses [
22]. On the other hand, not all authors agree that selective emotional attention is directly related to depressive moods. Balluerka et al. demonstrated that such correlation is not linear [
23]. Low levels of emotional attention limit the scope of emotional control processes, whereas high levels of emotional attention activate personality processes directed toward oneself, which facilitates rather than reduces expression of negative moods [
24].
Studies show that levels of EI may be related to expressions of behavior that damage individual’s health. Brackett et al. have determined that the inability to analyze one’s own emotions and use this information to create mental stability is related with negative outcomes like drug use and antisocial behavior [
25]. Low EI is also associated with alcohol addiction, deviant behavior, and poor interpersonal relationships [
26]. Humphrey et al. maintain that EI may be regarded as an important factor in preventing mental health problems and encouraging adjustment and well-being [
27]. A study performed by Brown and Schutte revealed that low EI levels significantly correlated with feelings of cognitive, physical, and social fatigue [
28]. Individuals with higher EI experienced less subjective stress, were in better physical health, and less often experienced mental burnout in jobs that required great tension [
29].
In summary, international studies have revealed a correlation between EI and psychological as well as physical health. However, the data presented is ambiguous. Furthermore, it is important to question whether these studies are culturally influenced. Therefore, it is feasible to explore how subjectively assessed physical health and some psychological states of Lithuanian youth are related to their EI.
The aim of this study was to reveal if the EI of Lithuanian youth was related to how they subjectively assessed their states of physical health, depressiveness, anxiety, and psychological well-being, as well as to find out whether the aforementioned factors were reliable predictors of EI constituents.
2. Materials and methods
Participants were selected using quota selection while observing natural proportions of the whole population of Lithuania. A total of 1430 participants from various regions of Lithuania – Vilnius, Kaunas, Klaipėda, Šiauliai, Panevėžys, Utena, Marijampolė, Kaišiadorys, and Alytus – were surveyed. The age of participants varied from 17 to 27 years (mean = 19.7, SD = 3.29). A total of 1092 study participants were surveyed, and included 11th- and 12th-grade students from general education schools and gymnasia (N = 371), students in vocational schools (N = 384), college students (N = 1580), and university students (N = 399). Some social movement and youth union members (e.g., young liberals [N = 11], scouts [N = 7], young unemployed people [N = 15], young imprisoned people [N = 54]) were surveyed as well. A total of 236 young people with working experience participated in the survey; the majority of them worked in private enterprises (N = 154) and state institutions (N = 55), and the rest worked in youth and sports organizations, or were individual entrepreneurs, farmers, or similar.
By summarizing the characteristics of the survey sample, it may be maintained that due to the nature of the study, variety of groups, sample size, and correlation of socio-demographic characteristics to the statistical indexes of the population, the sample may be considered conditionally representative and meeting the requirements of the study.
The study was performed using an original EI test (EI-DARL-V1/V2), which was comprised of three parts. The first portion was a traditional 73-item self-report questionnaire. Responses were scored on a 6-point Likert scale ranging from 1 (not true of me; strongly disagree) to 6 (true of me; strongly agree). Statements comprising the EI questionnaire portion were multiplexed into the following subscales using multi-step factor analysis: understanding of own emotions (e.g., “I well understand why I experience certain feelings”; “Sometimes I am very sad, but I do not know why”); control of own emotions and behavior (e.g., “I know very well what I have to do to cheer up”; “I manage to contain myself even in those cases when it seems that my patience is exhausted”); understanding emotions of other people (e.g., “I always recognize emotional states of my friends from their behavior”; “It is enough for me to listen to tone of voice to understand what a person is feeling”); control of interpersonal relationships (e.g., “I know how to encourage a person who is in a difficult situation”; “I would know how to comfort a crying child who was lost from their parents in a store”); and manipulation (e.g., “I know how to find a weak point in a person and sometimes I take advantage of it”; “If needed, I would know how to mock other people knowing that it would hurt them badly”).
Statements in the manipulation subscale were designed to determine personal abilities to control the behavior of other people by using their emotions or discovering their weaknesses, all of which do not indicate a high level of EI. Therefore, this subscale was eliminated from the EI construct used in this study. The results of multi-step factor analysis and multidi-mensional scaling confirmed that the manipulation subscale should not be included in the total EI scale. However, the manipulation subscale was incorporated into the test as an independent qualitative EI evaluation component, even though it was not a part of the total EI scale. Manipulative behavior subscale estimates that reflected a person’s ability to control the emotions of other people enabled this study to create a more comprehensive psychological portrait of the participant.
Only the subscales related to the ability of individuals to understand and manage their own emotions and the emotions of others were included in the total EI scale. Cronbach’s α was 0.67 and the resolution index r/itt varied from 0.36 and 0.54 in the total EI index. This index was comprised of the following subscales: understanding of own emotions, control of own emotions and behavior, understanding emotions of other people, and control of interpersonal relationships.
In addition to the traditional self-report questionnaire, two more scales were used: recognition of emotions in facial expressions (photographs), and resolution of emotional, social, and interpersonal situations. The participants were provided with albums of 20 photographs which reflected various emotional states. Participants were asked to recognize emotions in facial expressions by choosing one of four available options. Cronbach’s
α for the facial expression identification scale was relatively low (0.54), but it minimally satisfied requirements of psychometric quality. The test theory specifies the acceptable factor variation range as 0.5 <
α < 1 [
30,
31].
Furthermore, participants were given ten emotional, social, and/or interpersonal situations. Each situation had two mandatory answering formats: The first format implied assignments associated with hypothetical theoretical knowledge of how the situation should be solved (Cronbach’s α = 0.57), while the second format included the question of how the participant would personally resolve the given situation in reality (Cronbach’s α = 0.53). The participant was asked to select one of the provided answers that seemed to be the best/psychologically correct resolution of the situation. After having analyzed descriptive statistical data of this scale, it was found that in almost all cases, participants best resolved situations theoretically, and were less effective when asked to personally resolve situations.
Validity of the EI-DARL test was verified by comparing it to the results (averages) of Ullrich and Muynck’s (1998) Social Competence Test, adapted by Lekavičienė (1999) [
32]. Analysis of variance (ANOVA) was used to this end, and revealed similarities between the estimates of the EI-DARL and Social Competence Test. Reliability of the test (task compatibility) was assessed by comparing the results of two equivalent test parts. In other words, along with the classic Cronbach’s
α, the Spearman-Brown coefficient, based on split-half method, was used for scale reliability control. For the EI subscales, the Spearman–Brown correlation coefficient was above 0.7 and reached 0.87; therefore it can be stated that the reliability of the EI test is sufficient. More information on the EI-DARL test design and indexes of psychometric quality may be found in the following works of this article’s authors: “Design features of the short version EI-DARL-V1 original EI measurement technique”, and “The construction principles and problems of the long version EI-DARL-V2 original measurement methodology of emotional intelligence” [
33,
34].
Special questionnaires were designed and presented to the participants together with the EI questionnaire in order to assess subjective physical and mental health, depressiveness, anxiety, and psychological well-being. It must be emphasized that physical and mental health of participants was not assessed by objective clinical indicators, but by the self-knowledge questionnaire. A small group of nine statements (e.g., “Recently I experienced: headaches, disposition to cry often, pressure under chest, etc.”) was incorporated into the questionnaire. The statement block was conditionally called the health scale. Participants had to assess their health in the broadest sense by choosing indicators in the scale ranging from 0 (never; it is not characteristic of me) to 3 (often; this is very characteristic of me). In addition to EI test items and items that reflected a subjective assessment of individual health, participants were also given 16 items to assess signs of depressiveness and anxiety. Based on these items, two separate scales – depressiveness and anxiety – were multiplexed using factor analysis. After having applied factor analysis, sufficiently high correlation factors were obtained, with the KMO index reaching 0.93. Descriptive dispersion of both factors was 50.13%.
Depressiveness in the scale was represented by such items as, “I feel that others would be better off if I did not exist in this world at all”, or “Things that delighted me earlier do not cheer me anymore.” Anxiety was represented by items like “I feel embarrassed when upon my entrance into the room people suddenly stop talking”, or “I am more nervous than most people.” Agreement with the items was evaluated in a 6-step scale ranging from 1 (certainly no) to 6 (certainly yes).
The objective of this study was to find out how important psychological well-being is in regards to EI. This correlation has been researched by many authors who found that EI and psychological well-being are closely related phenomena [
35,
36]. A 10-question block was incorporated in the survey instrument, where participants were asked to assess their satisfaction in various aspects of their lives (e.g., relationships with friends, acquaintances, peers, colleagues; material status; activities like studies or work) on a scale from 0 (certainly no) to 2 (certainly yes) to determine the level of their psychological well-being.
Data analysis was conducted using the SPSS 23.0 statistical data processing package. The results were processed using the methods of mathematical statistics by calculating the mean, standard deviation, and standard error. For the assessment of internal consistency of the scales and subscales, Cronbach’s α and item-total correlations were calculated. The linear regression model was used to discover connections between EI and independent research variables like health, psychological well-being, depressiveness, and anxiety. The level of statistical significance of 0.05 was used for testing statistical hypotheses.
3. Results
Summarized descriptive statistics of dependent variables of the research are presented in
Table 1.
Participants rated EI test statements on a 6-point Likert scale; therefore, results could vary from 0 to 5. The average approval score was 2.5; the closer the average approached 5, the more expressed the measured characteristic. As shown in
Table 1, the averages of the total EI scale and all of its subscales surpass the formal average score; that is, they are higher than w2.5, with the control of interpersonal relations subscale presenting as the most expressed in the researched population.
Considering that the participant health assessment scale could vary in the 4-step range, from a minimum of 0 to a maximum of 3 points, the data showed that participants assessed their health status as very good, which may be expected in a population of young people. Health status assessments varied from 0.73 to 1.47, and did not reach the possible average of 2; in the health scale (mean, 1.02). Cronbach’s α for the aforementioned scale is good, equaling 0.79. The statement resolution indexes r/itt varies from 0.39 to 0.63.
Regression analysis was applied to find out whether individual health is a reliable predictor of a person’s EI and its constituents. It was noted that total EI is related to subjective health assessment (β = −0.25, P ≤ 0.05). Regression analysis did not reveal the relationship between subjective health assessment and understanding emotions of other people and manipulation subscales. The relationship between the health scale and resolution of social, interpersonal, and emotion-related situations and facial emotion recognition was not determined either. However, a negative linear correlation between the subjective assessment of one’s own health and the understanding of one’s own emotions subscale (β = −0.37, P ≤ 0.001) and control of own emotions and behavior subscale (β = −0.48, p ≤ 0.001) was determined. Also, the relationship between the health scale and control of interpersonal relationships subscale was determined, but it was not very strong (β = −0.11, P ≤ 0.05).
As seen in
Table 1, a mean score for the depressives and the anxiety scales was 1.52, and 2.02, respectively. Thus, the level of depression and anxiety in this population of young people was not high, but the average level of anxiety was slightly higher than the average level of depressiveness. Cronbach’s
α was calculated for both scales. In the depressiveness scale, Cronbach’s
α was 0.85 with a resolution factor r/itt varying from 0.45 to 0.67; in the anxiety scale, Cronbach’s
α was 0.83 with the r/itt varying from 0.43 to 0.68. Thus, it may be maintained that measurement accuracy of both scales is sufficient.
The correlations between the EI test subscale and depressiveness and anxiety scales were calculated. The results revealed the following major issues: (a) total EI was connected to both depressiveness (β = −0.32, P ≤ 0.01) and anxiety (β = −0.27, P ≤ 0.01); (b) depressive participants were poorer at understanding the emotions of other people (β = −0.19, P ≤ 0.0001) and controlling interpersonal relationships (β = −0.27, P ≤ 0.001); (c) depressiveness was significantly negatively related to understanding one’s own emotions (β = −0.44, P ≤ 0.001), and the ability to control one’s own emotions (β = −0.47, P ≤ 0.001); (d) anxious participants were less capable of understanding the emotions of other people (β = −0.16, P ≤ 0.01), and were worse at controlling interpersonal relationships (β = −0.24, P ≤ 0.001); (e) anxiety was more significantly negatively related to understanding one’s own emotions (β = −0.44, P ≤ 0.001), and the ability to control one’s own emotions (β = −0.55, P ≤ 0.001); (f) the relationship between expressiveness and resolution of emotional, social, and interpersonal situations (the second part of responses, in which the participants specified their own personal resolution of the situation) was determined (β = −0.21, P ≤ 0.001); (g) analogous to the case of depressiveness, a weak inverse linear correlation with the resolution of emotional social and interpersonal situations scale was detected on the anxiety scale (β = −0.14, P ≤ 0.05); and (h) the authors did not detect a correlation between depressiveness and anxiety, and the emotion recognition in facial expressions and manipulation subscales.
It was discovered that in the researched population, the Mean for the psychological well-being scale was relatively high at 147. To ensure that all psychological well-being scale items sufficiently reflected the research values, Cronbach’s α was calculated at 0.76, with a resolution index r/itt varying from 0.30 to 0.54. Therefore, it may be maintained that reliability of the scale is sufficient.
After applying linear regression, it was established that the state of psychological well-being correlated with total EI (β = 0.21, P ≤ 0.05). Furthermore, the scale of psychological well-being correlated with some components of EI: for example, the ability to control interpersonal relationships (β = 0.18, P ≤ 0.001), under- standing of one’s own emotions (β = 0.30, P ≤ 0.001), and control of one’s own emotions and behavior (β = 0.31, P ≤ 0.001) were directly related to psychological well-being.
The authors failed to determine the relationship between the psychological well-being scale, understanding emotions of other people subscale, emotional, social, and interpersonal situations scale, and the emotion recognition in facial expression (pictures) scale.
Standardized regression factor values and their reliability indexes are presented in
Table 2 in order to obtain a clearer general view of correlations determined in the study. Health, depressiveness, anxiety, and psychological well-being scales were included in the regression model as independent variables; understanding of own emotions, control of own emotions and behavior, understanding emotions of other people, and control of interpersonal relationships subscales were included as dependent variables.
For the sake of objectivity, it must be noted that values of set correlation factors and determination factors in the discussed regression models are not high, but regression model reliability, beta factors, and beta factor reliability is satisfactory. Therefore, the data theoretically may be meaningfully interpreted.
4. Discussion
The objective of this study was to find out how the EI of young Lithuanian individuals is related to subjectively assessed states of health, depressiveness, anxiety, and psychological well-being. Self-knowledge questionnaires, resolution of emotional, social, and interpersonal situations, and recognition of emotions in facial expressions were used to achieve this goal. Regression analysis was applied to calculate correlations between EI and its factors.
As seen in
Table 2, an established negative correlation demonstrated that participants who experienced certain somatic symptoms or unpleasant psychological conditions had lower EI. Particularly strong correlation was observed between poor health conditions and understanding and control over one’s own emotions. This correlation is easily interpretable: it is natural that an individual who is not well and who suffers from certain physical conditions would be irritable, nervous, and less agreeable.
This study did not succeed in finding analogous studies proving EI’s relationship with psychosomatic indexes after having researched scientific literature. However, studies in which correlations between EI and health-related behavior were investigated demonstrated for instance that higher EI correlated with lower tobacco (
r = −0.16) and alcohol (
r = −0.19) consumption among teenagers [
37]. In a survey of college students, an inverse correlation was determined between alcohol consumption by men and EI (
r = −0.2) [
25,
38]. Also, EI may be regarded as an illegal drug-use predictor (
r = −0.32) [
39]. A small-scale study done at the Stockholm School of Economics has proven that a strong ability to understand emotions reduces the risk of addiction to the Internet [
40]. In summary, it may be asserted that obtained results from these studies confirm tendencies recorded in the present study.
Studies performed by international scientists show that EI improves psychological health, reduces depression, and soothes anxiety [
39]. Scientists maintain that people with lower EI quite often experience depression or anxiety. This study surveyed the EI of Lithuanian teenagers and also determined a weak negative, but statistically significant correlation between EI and depressiveness/anxiety [
41].
Results of the present study have revealed that EI, similarly to the subjective assessment of one’s own physical and psychological health, was inversely linearly related to depressiveness and anxiety. There was an unsubstantial inverse linear correlation between EI and the subscale of understanding emotions of other people, as well as with depressiveness and anxiety. A stronger correlation was observed between EI and the control of interpersonal relations subscale. The strongest correlation was determined between EI and the understanding of one’s own emotions and control of one’s own emotions and behavior subscales. Brown and Schutte reported similar correlations to those found in this study [
28]. They presented a relatively high correlation between depressiveness and low EI (
r = 0.35), and an even greater correlation between low EI and experiences of fear (
r = 0.39,
P < 0.01).
Similar results are also found in other publications presented by international authors. Individuals who are anxious and inclined to avoidance tend to reject emotion-related thoughts in order to avoid emotion-related actions, or suppress both verbal and non-verbal emotional expressions when they control their emotions [
42]. Lanciano et al. supported the empirically confirmed view that depressive thinking is related to the inability to use and to substantiate emotions [
43]. This means that anxious individuals face serious resource limitations when processing emotions. Such people are not capable of coping with emotional problems and finding resolution, which creates an environment that facilitates symptoms of depression. At the same time, different data is obtained when EI is measured using different methodologies (i.e., when EI is considered as a set of certain traits versus as a set of certain abilities). Negative correlations between EI and depressiveness, anxiety, and apprehension are more often recorded when methodologies of the first type are applied; correlations established by applying methodologies of the second type are very weak or even statistically insignificant [
17,
44].
As seen in
Table 2, unlike poor assessment of health, depressiveness, and anxiety, EI is directly related to the state of psychological well-being in three subscales: understanding of one’s own emotions, control of one’s own emotions and behavior, and control of interpersonal relationships. In other words, psychological well-being is a reliable EI predictor.
Various studies performed internationally also reveal the existence of analogous correlations. For example, Berezovskaya and Kirilova recorded fairly high correlations between EI levels and life satisfaction (
r = 0.415) [
45]. Positive correlations are also confirmed by studies performed by Schutte et al.; Rothmann; Schutte and Malouff; and others [
44,
46].
It is worth noting that the cultural environment may influence the solidity of correlations. Koydemir et al. compared the correlation between life satisfaction and EI levels of students from an individualistic culture (Germany) versus a collectivist culture (India) [
47]. Even though statistically meaningful correlation was recorded in both participant groups, the said correlation was much stronger among students from individualistic cultures.
It must be noted that the second part of the EI-DARL test – solutions to emotional, social, and interpersonal situations – was related to the depressiveness scale, whereas the third part – recognition of emotions in non-verbal signs (photographs of faces) – was not related to any of the EI subscales.
In summary, it may be maintained that in the cultural context of Lithuania, a statistically reliable correlation between EI and subjective assessment of individual health in terms of mental, physical, and social well-being has been determined. In many cases, the results agree with data obtained by other authors. It has been determined that best forecast, reaching as much as 35%, is of the control of own emotions subscale by considering subjective assessment of individual’s health, depressiveness, anxiety, and psychologi- cal well-being.
The data from this study may be useful in two aspects. First, it supplements conclusions of the latest empirical studies suggesting that EI is related to various factors, including subjective assessment of physical and psychological well-being, depressiveness, and anxiety. Secondly, the results of the study are valuable in a practical aspect because they may be used by psychologists and educators who are interested in EI development.
This study has revealed several meaningful factors influencing the construct of EI. Future investigations into what types of somatic disorders and what levels of hypochon-dria are related (or not related) to EI – and to what degree – would be worthwhile.
5. Conclusions
This study has revealed that some factors (e.g., subjective assessment of physical and mental health, depressiveness, anxiety, and psychological well-being) in populations of Lithuanian youth are reliable predictors of some EI indexes, including understanding and control of one’s own emotions, and understanding and controlling the emotions of other people. Some significant discoveries from this study include the following:
It has been determined that participants experiencing certain somatic symptoms or other unpleasant states are characterized by lower total EI.
Negative linear correlations have been determined among total EI scores and all EI subscales on the one hand, and with depressiveness and anxiety on the other hand. Furthermore, depressive and anxious individuals more often choose inappropriate solutions to emotional, social, and interpersonal situations in real life than those who were not found to be depressive and anxious individuals.
It has been revealed that total EI positively and significantly correlates with subjectively perceived well-being.



{kind=link}