Periodontal status in 18-year-old Lithuanian adolescents: An epidemiological study

Abstract
:1. Introduction
2. Materials and methods
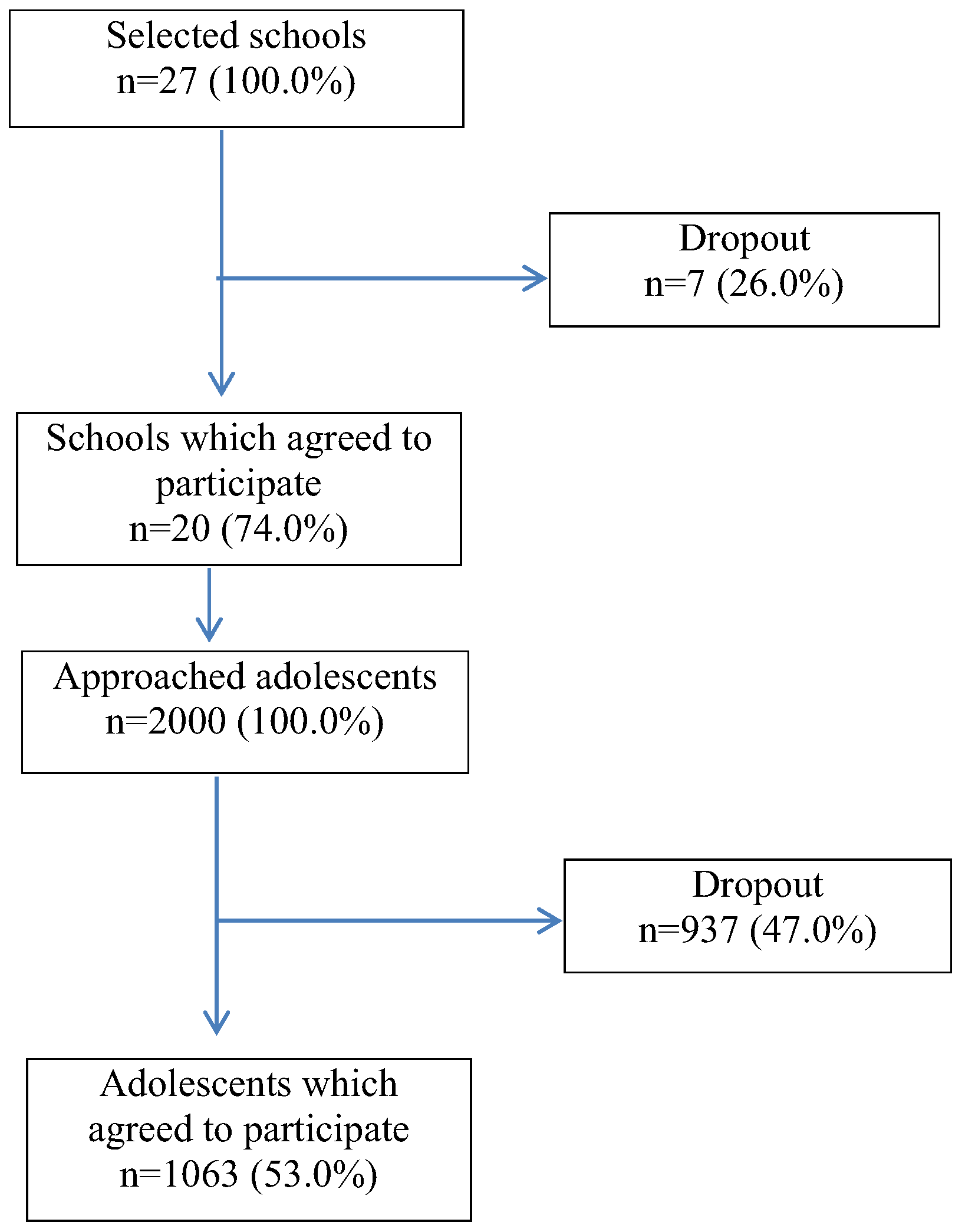
2.1. Study population
2.2. Final sample
2.3. Clinical examination and interview
2.4. Statistical analysis
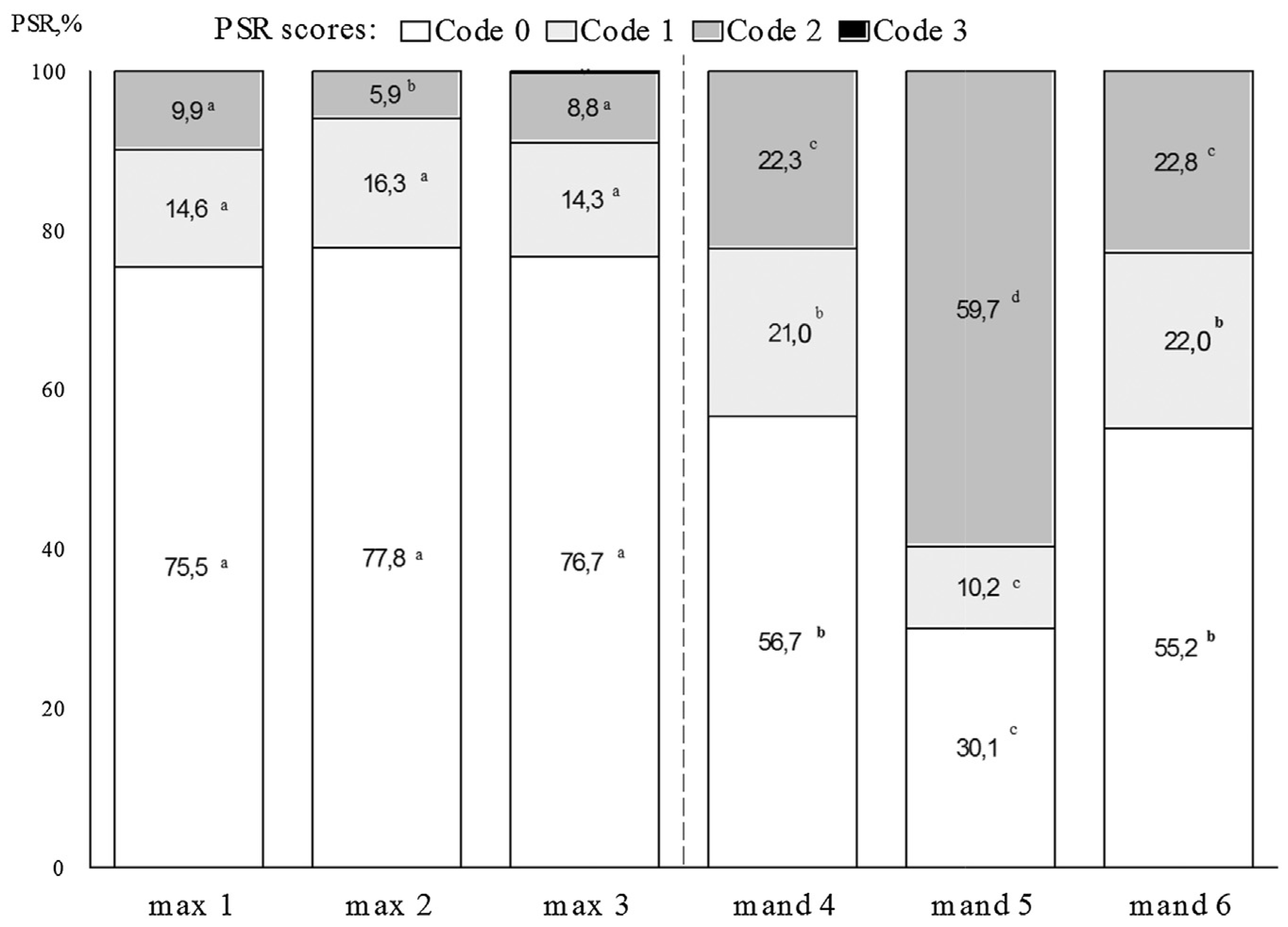
3. Results
4. Discussion
5. Conclusions
Conflict of interest
References
- World Health Organisation. The World Health Report 2002. Reducing risks, promoting healthy life. World Health Organisation: Geneva, 2002. [Google Scholar]
- Petersen, PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century – the approach of WHO Global Oral Health Programme. Commun Dent Oral Epidemiol 2003, 31 (Suppl. 1), 3–24. [Google Scholar] [CrossRef]
- Albandar, JM; Tinoco, EMB. Global epidemiology of periodontal diseases in children and young persons. Periodontology 2000 2002, 29, 153–76. [Google Scholar] [CrossRef]
- Bendoraitiene, E; Milciuviene, S. Periodontal status and oral hygiene among Lithuanian 12 years old schoolchildren. Stomatologija 2001, 3(2), 10–3. [Google Scholar]
- Skudutytė, R; Aleksejūnienė, J; Eriksen, HM. Periodontal conditions among Lithuanian adults. Acta Med Litu 2001, 8(1), 57–61. [Google Scholar]
- Kelbauskas, E; KelbauskienėS, S; Paipalienė, P. Šauktinių į Lietuvos kariuomenę burnos higiena ir apydančio audinių (periodonto) būklė [Oral hygiene and periodontal status among Lithuanian army recruits]. Stomatologija (Moksliniai darbai) 2000, 4(2), 10–4, ISSN 1392-8589. [Google Scholar]
- Nakagawa, S; Fujii, H; Machida, Y; Okuda, K. A longitudinal study from prepuberty to puberty of gingivitis. Correlation between the occurrence of Prevotella intermedia and sex hormones. J Clin Periodontol 1994, 21, 658–65. [Google Scholar] [CrossRef] [PubMed]
- Albandar, JM; Rams, TE. Risk factors for periodontitis in children and young persons. Periodontol 2000 2002, 29, 207–22. [Google Scholar] [CrossRef] [PubMed]
- Dentino, A; Lee, S; Mailhot, J. Principles of periodontology. Periodontol 2000 2013, 61, 16–53. [Google Scholar] [CrossRef] [PubMed]
- Albandar, JM; Rams, TE. Global epidemiology of periodontal diseases: an overview. Periodontol 2000 2002, 29, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Clerehugh, V; Worhtington, HV; Lennon, MA. Site progression of loss of attachment over 5 years in 14- to 19-year-old adolescents. J Clin Periodontol 1995, 22, (January (1)). 15–21. [Google Scholar] [CrossRef] [PubMed]
- Wolf, HF; Hassell, TM. Periodontology. Color Atlas of Dental Hygiene Color atlas of dental hygiene: periodontology. Thieme: Stuttgart, 2006. [Google Scholar]
- The State of Oral health in Europe. Report commissioned by the platform for better oral health in Europe. 2012. Available from: http://www.oralhealthplatform.eu/wp-content/uploads/2015/09/Report-the-State-of-Oral-Health-in-Europe.pdf.
- Laganà, G; Abazi, Y; Nastasi, EB; Vinjolli, F; Fabi, F; Divizia, M; et al. Oral health conditions in an Albanian adolescent population: an epidemiological study. BMC Oral Health 2015, 15, 67. [Google Scholar]
- Mizutani , S; Ekuni, D; Furuta, M; Tomofuji, T; Irie, K; Azuma, T; et al. Effects of self-efficacy on oral health behaviours and gingival health in university students aged 18- or 19-years-old. J Clinic Periodontol 2012, 39, 844–9. [Google Scholar] [CrossRef] [PubMed]
- Hessari , H; Vehkalahti, MM; Eghbal, MJ; Samadzadeh, H; Murtomaa, HT. Oral health and treatment needs among 18-year-old Iranians. Med Princ Pract 2008, 17, 302–7. [Google Scholar] [CrossRef] [PubMed]
- Petersen, PE; Ogawa, H. The global burden of periodontal disease: towards integration with chronic disease prevention and control. Periodontology 2000 2012, 60, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Novaes Júnior, AB; Souza, SLS; Taba, M; Grisi, MFM; Suzigan, LC; Tunes, RS. Control of gingival inflammation in a teenager population using ultrasonic prophylaxis. Braz Dent J 2004, 15(1), 41–5. [Google Scholar] [CrossRef]
- Susin , C; Haas, AN; Valle, PM; Oppermann, RV; Albandar, JM. Prevalence and risk indicators for chronic periodontitis in adolescents and young adults in South Brazil. J Clin Periodontol 2011, 38, 326–33. [Google Scholar] [CrossRef] [PubMed]
- Jenkins , WMM; Papapanou, PN. Epidemiology of periodontal disease in children and adolescents. Periodontology 2000 2001, 26, 16–32. [Google Scholar] [CrossRef]
- Wilkins, EM. Clinical practice of the dental hygienist, 9th edLippincott Williams &Wilkins: Philadelphia, PA, 2005. [Google Scholar]
- Furuta, M; Ekuni, D; Irie, K; Azuma, T; Tomofuji, T; Ogura, T; et al. Sex differences in gingivitis relate to interaction of oral health behaviors in young people. J Periodontol 2011, 82(4), 558–65. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, JS; Abrahamsson, KH; Östregal, AL; Hellström, MK; Jönsson, K; Wennström, JL. Periodontal health status in Swedish adolescents: an epidemiological, cross-sectional study. Swed Dent J 2009, 33, 131–9. [Google Scholar] [PubMed]
- Antunes, JLF; Peres, MA; Frias, AC; Crosato, EM; Biazevic, MGH. Gingival health of adolescents and the utilization of dental services, state of São Paulo, Brazil. Rev Saúde Pública 2008, 42(2), 1–7. [Google Scholar]
- Levin, L; Margvelashvili, V; Bilder, L; Kalandadze, M. Periodontal status among adolescents in Georgia. A pathfinder study. PeerJ 2013, 1, e137. [Google Scholar] [CrossRef] [PubMed]
- Ericssons, JS; Östberg, AL; Wennström, JL; Abrahamsson, KH. Oral health-related perceptions, and behavior in relation to oral hygiene conditions in an adolescent population. Eur J Oral Sci 2012, 120, 335–41. [Google Scholar] [CrossRef] [PubMed]
- Bartold , PM; Van Dyke, TE. Periodontitis: a host-mediated disruption of microbial homeostasis. Unlearning learned concepts. Periodontology 2000 2013, 62, 203–17. [Google Scholar] [CrossRef] [PubMed]
- Tseveenjav, B; Virtanen, JI; Wang, NJI; Widström, E. Working profiles of dental hygienists in public and private practice in Finland and Norway. Int J Dent Hyg 2009, 7, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Brukienė, V; Aleksejūnienė, J. An overview of oral health promotion in adolescents. Int J Paediatr Dent 2009, 1, 163–71. [Google Scholar]
- Statistics Lithuania. Education 2014; Vilnius 2015. Available from: https://osp.stat.gov.lt/services-portlet/pub-edition-file?id=18138.



{kind=link}
{kind=link}
| Codes of the PSR index | Gender | Place of residence | Parental education level | ||||
|---|---|---|---|---|---|---|---|
| Boys | Girls | Urban | Rural | Low | Medium | High | |
| 0 | 72 (18.1)a | 156 (26.2)a | 161 (23.4) | 67 (21.8) | 63 (21.6) | 65 (23.8) | 74 (25.1) |
| 1 | 79 (19.8)b | 73 (12.2)b | 107 (15.6) | 45 (14.7) | 54 (18.6)c | 26 (9.5)c | 39 (13.2) |
| 2 | 245 (61.6) | 367 (61.6) | 417 (60.7) | 195 (63.5) | 174 (59.8) | 182 (66.7) | 182 (61.7) |
| 3 | 2 (0.5) | 0 | 2 (0.3) | 0 | 0 | 0 | 0 |
| χ2 = 18.81, df = 3, P < 0.001; | χ2 = 1.524, df = 3, P = 0.677 | χ2 = 10.301, df = 4, P = 0.036; cP = 0.002 | |||||
| a,bP < 0.01 | |||||||
| Values are number (percentage). The same superscript letters indicate a statistically significant difference in the prevalence of PSR index codes. | |||||||
© 2017 The Lithuanian University of Health Sciences. Production and hosting by Elsevier Sp. z o.o. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Share and Cite
Bendoraitienė, E.; Zūbienė, J.; Vasiliauskienė, I.; Saldūnaitė, K.; Andruškevičienė, V.; Basevičienė, N.; Slabšinskienė, E. Periodontal status in 18-year-old Lithuanian adolescents: An epidemiological study. Medicina 2017, 53, 253-258. https://doi.org/10.1016/j.medici.2017.06.002
Bendoraitienė E, Zūbienė J, Vasiliauskienė I, Saldūnaitė K, Andruškevičienė V, Basevičienė N, Slabšinskienė E. Periodontal status in 18-year-old Lithuanian adolescents: An epidemiological study. Medicina. 2017; 53(4):253-258. https://doi.org/10.1016/j.medici.2017.06.002
Chicago/Turabian StyleBendoraitienė, Eglė, Jūratė Zūbienė, Ingrida Vasiliauskienė, Kristina Saldūnaitė, Vilija Andruškevičienė, Nomeda Basevičienė, and Eglė Slabšinskienė. 2017. "Periodontal status in 18-year-old Lithuanian adolescents: An epidemiological study" Medicina 53, no. 4: 253-258. https://doi.org/10.1016/j.medici.2017.06.002