Mortality prediction in patients with acute kidney injury requiring renal replacement therapy after cardiac surgery

Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Statistical analysis
3. Results
4. Discussion
5. Conclusions
Conflicts of interest
Funding
Author’ contributions
Ethical approval
R E F E R E N C E S
- Rosner, M.H.; Okusa, M.D. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol 2006, 1, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-term risk of mortality and other adverse outcomes after acute kidney injury: a systematic review and meta-analysis. Am J Kidney Dis 2009, 53, 961–73. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.B.; Suneja, M. Cardiopulmonary bypass-associated acute kidney injury. Anesthesiology 2011, 114, 964–70. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.; Kellum, J.A.; Katz, N.M.; Rosner, M.H.; Haase, M.; Ronco, C. Epidemiology of acute kidney injury. Contrib Nephrol 2010, 165, 1–8. [Google Scholar] [PubMed]
- Shaw, A. Update on acute kidney injury after cardiac surgery. J Thorac Cardiovasc Surg 2012, 143, 676–81. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.R.; Cochran, R.P.; Leavitt, B.J.; Dacey, L.J.; Ross, C.S.; MacKenzie, T.A.; et al. Northern New England Cardiovascular Disease Study Group: multivariable prediction of renal insufficiency developing after cardiac surgery. Circulation 2007, 116, 1139–43. [Google Scholar] [CrossRef] [PubMed]
- Mariscalco, G.; Lorusso, R.; Dominici, C.; Renzulli, A.; Sala, A. Acute kidney injury: a relevant complication after cardiac surgery. Ann Thorac Surg 2011, 92, 1539–47. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Worley, S.; Arrigain, S.; Yared, J.-P.; Paganini, E.P. Influence of renal dysfunction on mortality after cardiac surgery: modifying effect of preoperative renal function. Kidney Int 2005, 67(3), 1112–9. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Paganini, E.P. (Eds.) Acute renal failure after cardiac surgery. In Critical Care Nephrology, 2nd ed.; Elsevier: Saunders, 2009; pp. 977–83. [Google Scholar]
- Bagshaw, S.M.; Wald, R.; Barton, J.; Burns, K.E.; Friedrich, J.O.; House, A.A.; et al. Clinical factors associated with initiation of renal replacement therapy in critically ill patients with acute kidney injury-a prospective multicenter observational study. J Crit Care 2012, 27, 268–75. [Google Scholar] [CrossRef] [PubMed]
- Mårtensson, J.; Martling, C.R.; Oldner, A.; Bell, M. Impact of sepsis on levels of plasma cystatin C in AKI and non-AKI patients. Nephrol Dial Transplant 2012, 27, 576–81. [Google Scholar] [CrossRef] [PubMed]
- Siew, E.D.; Deger, S.M. Recent advances in acute kidney injury epidemiology. Curr Opin Nephrol Hypertens 2012, 21(3), 309–17. [Google Scholar] [CrossRef] [PubMed]
- Englberger, L.; Suri, R.M.; Li, Z.; Dearani, J.A.; Park, S.J.; Sundt, T.M., 3rd; et al. Validation of clinical scores predicting severe acute kidney injury after cardiac surgery. Am J Kidney Dis 2010, 56, 623–31. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Arrigain, S.; Worley, S.; Yared, J.P.; Paganini, E.P. A clinical score to predict acute renal failure after cardiac surgery. J Am Soc Nephrol 2005, 16(1), 162–8. [Google Scholar] [CrossRef] [PubMed]
- KDIGO. Clinical Practice Guideline for Acute Kidney Injury: definition and classification of AKI. Kidney Int 2012, 2(1), 19–36. [Google Scholar]
- ACCP/SCCM Consensus Conference Committee. Definitions for sepsis and organ failure and guidelines for use of innovate therapies in sepsis. Crit Care Med 1992, 20, 867–74. [Google Scholar]
- Machado, M.N.; Nakazone, M.A.; Maia, L.N. Prognostic value of acute kidney injury after cardiac surgery according to kidney disease: improving global outcomes definition and staging (KDIGO) criteria. PLOS ONE 2014, 9, e98028. [Google Scholar] [CrossRef] [PubMed]
- Vives, M.; Wijeysundera, D.; Marczin, N.; Monedero, P.; Rao, V. Cardiac surgery-associated acute kidney injury. Interact CardioVasc Thorac Surg 2014, 18(5), 637–45. [Google Scholar] [CrossRef] [PubMed]
- Bastin, A.J.; Ostermann, M.; Slack, A.J.; Diller, G.P.; Finney, S.J.; Evans, T.W. Acute kidney injury after cardiac surgery according to Risk/Injury/Failure/Loss/End-stage. Acute kidney injury network, and kidney disease: improving global outcomes classifications. J Crit Care 2013, 28, 389–96. [Google Scholar] [CrossRef] [PubMed]
- Parolari, A.; Pesce, L.L.; Pacini, D.; Mazzanti, V.; Salis, S.; Sciacovelli, C.; et al. Risk factors for perioperative acute kidney injury after adult cardiac surgery: role of perioperative management. Ann Thorac Surg 2012, 93, 584–91. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.R.; Kramer, R.S.; Coca, S.G.; Parikh, C.R. Duration of acute kidney injury impacts long-term survival after cardiac surgery. Ann Thorac Surg 2010, 90, 1142–8. [Google Scholar] [CrossRef] [PubMed]
- Hobson, C.E.; Yavas, S.; Segal, M.S.; Schold, J.D.; Tribble, C.G.; Layon, A.J.; et al. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation 2009, 119, 2444–53. [Google Scholar] [CrossRef] [PubMed]
- Malov, A.A.; Borisov, A.S.; Lomivorotov, V.V.; Efremov, S.M.; Ponomarev, D.N.; Mukhoedova, T.V.; et al. Mortality prediction in patients with dialysis-dependent acute kidney injury after cardiac surgery with cardiopulmonary bypass. Heart Lung Circ 2014, 23, 325–31. [Google Scholar] [CrossRef] [PubMed]
- Huen, S.C.; Parikh, C.R. Predicting acute kidney injury after cardiac surgery: a systematic review. Ann Thorac Surg 2012, 93, 337–47. [Google Scholar] [CrossRef] [PubMed]
- Karkouti, K.; Wijeysundera, D.N.; Yau, T.M.; Callum, J.L.; Cheng, D.C.; Crowther, M.; et al. Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation 2009, 119, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Alsabbagh, M.M.; Asmar, A.; Ejazc, N.I.; Aiyer, R.K.; Kambhampati, G.; Ejaz, A.A. Update on clinical trials for the prevention of acute kidney injury in patients undergoing cardiac surgery. Am J Surg 2013, 206, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, B.C.; Stearns, S.C.; Rossi, J.S.; D’Arcy, L.P.; Federspiel, J.J.; Carey, T.S. Three-year outcomes of multivessel revascularization in very elderly coronary syndrome patients. Ann Thorac Surg 2010, 89, 1889–94. [Google Scholar] [CrossRef] [PubMed]
- Mukhoedova, T.V.; Lomivorotov, V.N.; Kolesnikov, S.V.; Litasova, E.E.; Malov, A.A.; Borisov, A.S. Prediction of the outcomes of renal replacement therapy for acute renal failure after cardiosurgical interventions. Anesteziol Reanimatol 2005, 2, 53–8. [Google Scholar]


{kind=link}
| Factors | All (n = 111) | Survivors (n = 26) | Non-survivors (n = 85) | P |
|---|---|---|---|---|
| Demographic and preoperative | ||||
| Age, years | 67.15 ± 1.06 | 67.58 ± 2.56 | 67.02 ± 1.15 | 0.826 |
| Female | 68.66 ± 2.45 | 69.75 ± 7.51 | 68.48 ± 2.64 | 0.084 |
| Male | 66.62 ± 1.15 | 67.18 ± 2.77 | 66.42 ± 1.21 | |
| Female/male, n (%) | 29 (26.1)/82 (73.9) | 4 (15.4)/22 (84.6) | 25 (29.4)/60 (70.6) | 0.154 |
| Diabetes, n (%) | 19 (17.1) | 5 (19.2) | 14 (16.5) | 0.744 |
| Myocardial infarction, n (%) | 26 (23.4) | 6 (23.1) | 20 (23.5) | 0.962 |
| Chronic renal failure, n (%) | 17 (16.22) | 2 (7.7) | 15 (17.6) | 0.093 |
| Serum creatinine, µmol/L | 145.38 ± 8.61 | 142.04 ± 81.03 | 144.49 ± 88.43 | 0.900 |
| eGFR using MDRD, mL/min/1.73 m2 | 60.18 ± 2.88 | 66.59 ± 6.56 | 58.21 ± 3.04 | 0.331 |
| <30, n (%) | 12 (10.8) | 1 (3.8) | 11 (12.9) | 0.485 |
| 30–59, n (%) | 43 (38.8) | 11 (42.3) | 32 (37.6) | |
| 60–89, n (%) | 39 (35.1) | 11 (42.3) | 28 (32.9) | |
| ≥90, n (%) | 17 (15.3) | 3 (11.5) | 14 (16.5) | |
| Surgical | ||||
| Urgent surgery, n (%) | 62 (55.9) | 13 (50.0) | 49 (57.6) | 0.492 |
| Cardiac surgery type | ||||
| Valve, n (%) | 11 (9.9) | 5 (19.2) | 6 (7.1) | 0.255 |
| CABG, n (%) | 45 (40.5) | 11 (42.3) | 34 (40.0) | |
| CABG and valve, n (%) | 18 (16.2) | 5 (19.2) | 13 (15.3) | |
| Reconstruction of aorta, n (%) | 18 (16.2) | 2 (7.7) | 16 (18.8) | |
| Others, n (%) | 19 (17.1) | 3 (11.5) | 16 (18.8) | |
| CPB, n (%) | 90 (81.1) | 23 (88.5) | 67 (78.8) | 0.272 |
| CPB time, min | 156.72 ± 9.29 | 171.00 ± 22.41 | 151.82 ± 9.86 | 0.371 |
| APACHE II score | 24.77 ± 6.16 | 22.19 ± 1.11 | 25.56 ± 0.66 | 0.014 |
| SOFA score | 14.59 ± 0.44 | 11.27 ± 0.981 | 15.38 ± 0.49 | 0.0001 |
| Liano score | 0.628 ± 0.17 | 0.556 ± 0.341 | 0.650 ± 0.194 | 0.02 |
| Postoperative | ||||
| Administration of inotropes | ||||
| None, n (%) | 25 (22.5) | 8 (30.8) | 17 (20.0) | 0.627 |
| Low dose, n (%) | 19 (17.1) | 5 (19.2) | 14 (16.5) | |
| Moderate dose, n (%) | 45 (40.5) | 9 (34.6) | 36 (42.4) | |
| High dose, n (%) | 22 (19.8) | 4 (15.4) | 18 (21.2) | |
| Hospitalization duration before ICU (days) | 7.66 ± 1.08 | 8.58 ± 1.93 | 7.38 ± 1.28 | 0.640 |
| Hospitalization duration in ICU before RRT initiation (days) | 6.61 ± 0.70 | 5.58 ± 0.99 | 6.93 ± 0.86 | 0.419 |
| Risk factors of AKI | ||||
| 0, n (%) | 20 (18.0) | 5 (19.2) | 15 (17.6) | 0.748 |
| 1–3, n (%) | 83 (74.8) | 20 (76.9) | 63 (74.1) | |
| >3, n (%) | 8 (7.2) | 1 (3.8) | 7 (8.2) | |
| Sepsis without septic shock, n (%) | 7 (7.2) | 3 (11.5) | 4 (4.7) | 0.379 |
| Sepsis with septic shock, n (%) | 23 (20.7) | 4 (15.4) | 19 (22.4) | |
| Oliguria, n (%) | 65 (58.6) | 13 (50.0) | 52 (61.2) | 0.311 |
| Serum creatinine before RRT, mmol/L | 400.37 ± 14.49 | 449.77 ± 31.83 | 385.26 ± 15.97 | 0.059 |
| Blood urea before RRT, mmol/L | 27.91 ± 1.35 | 26.88 ± 2.49 | 28.22 ± 1.58 | 0.676 |
| Serum potassium before RRT, mmol/L | 5.31 ± 0.09 | 5.17 ± 0.15 | 5.34 ± 0.10 | 0.421 |
| RRT modality, n (%) | ||||
| IHD | 49 (44.1) | 17 (65.4) | 32 (37.6) | 0.240 |
| CVVH or CVVHDF | 43 (38.7) | 5 (19.2) | 38 (44.7) | 0.601 |
| IHD + CVVH or CVVHDF | 19 (17.2) | 4 (15.4) | 15 (17.7) | 0.165 |
| Other outcomes | ||||
| Length of hospital stay, days | 35.5 ± 3.24 | 65.69 ± 7.93 | 26.26 ± 2.80 | 0.0001 |
| Values are mean ± standard deviation. CABG, coronary artery bypass grafting; CPB, cardiopulmonary bypass; RRT, renal replacement therapy; ICU, intensive care unit; IHD, intermittent hemodialysis; CVVH, continuous venovenous hemofiltration; CVVHDF, continuous venovenous hemodiafiltration. | ||||
| Variable | Coefficient estimate | Odds ratio (95% CI) | P |
|---|---|---|---|
| Glasgow coma points | 0.547 | 3.304 (1.130–9.662) | 0.0029 |
| Mean arterial blood pressure | 0.642 | 3.872 (1.01–13.616) | 0.035 |
| Postoperative platelet count | 0.554 | 3.731 (1.259–11.054) | 0.018 |
| Preoperative serum creatinine | 0.531 | 0.347 (0.123–0.982) | 0.046 |
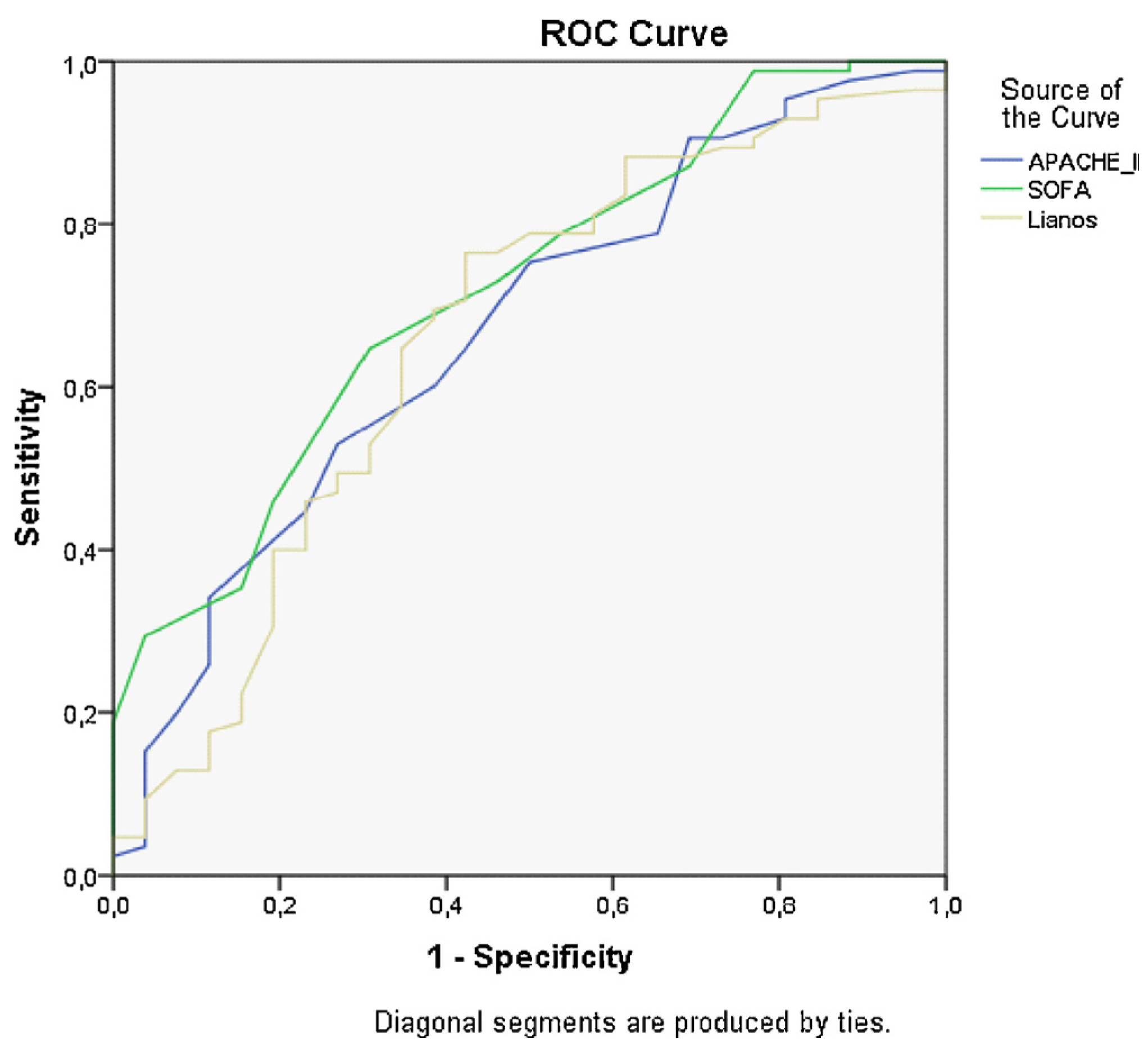
| SOFA | APACHE II | Liano | |
|---|---|---|---|
| Area under curve (AUC) | 0.719 | 0.668 | 0.661 |
| Standard error | 0.062 | 0.060 | 0.064 |
| 95% CI | 0.598–0.841 | 0.550–0.785 | 0.535–0.787 |
© 2017 The Lithuanian University of Health Sciences. Production and hosting by Elsevier Sp. z o.o. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Share and Cite
Skarupskienė, I.; Adukauskienė, D.; Kuzminskienė, J.; Rimkutė, L.; Balčiuvienė, V.; Žiginskienė, E.; Kuzminskis, V.; Adukauskaitė, A.; Pentiokinienė, D.; Bumblytė, I.A. Mortality prediction in patients with acute kidney injury requiring renal replacement therapy after cardiac surgery. Medicina 2017, 53, 217-223. https://doi.org/10.1016/j.medici.2017.06.003
Skarupskienė I, Adukauskienė D, Kuzminskienė J, Rimkutė L, Balčiuvienė V, Žiginskienė E, Kuzminskis V, Adukauskaitė A, Pentiokinienė D, Bumblytė IA. Mortality prediction in patients with acute kidney injury requiring renal replacement therapy after cardiac surgery. Medicina. 2017; 53(4):217-223. https://doi.org/10.1016/j.medici.2017.06.003
Chicago/Turabian StyleSkarupskienė, Inga, Dalia Adukauskienė, Jurgita Kuzminskienė, Laima Rimkutė, Vilma Balčiuvienė, Edita Žiginskienė, Vytautas Kuzminskis, Agnė Adukauskaitė, Daiva Pentiokinienė, and Inga Arūnė Bumblytė. 2017. "Mortality prediction in patients with acute kidney injury requiring renal replacement therapy after cardiac surgery" Medicina 53, no. 4: 217-223. https://doi.org/10.1016/j.medici.2017.06.003