
Thrombomodulin Serum Levels—A Predictable Biomarker for the Acute Onset of Ischemic Stroke
 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
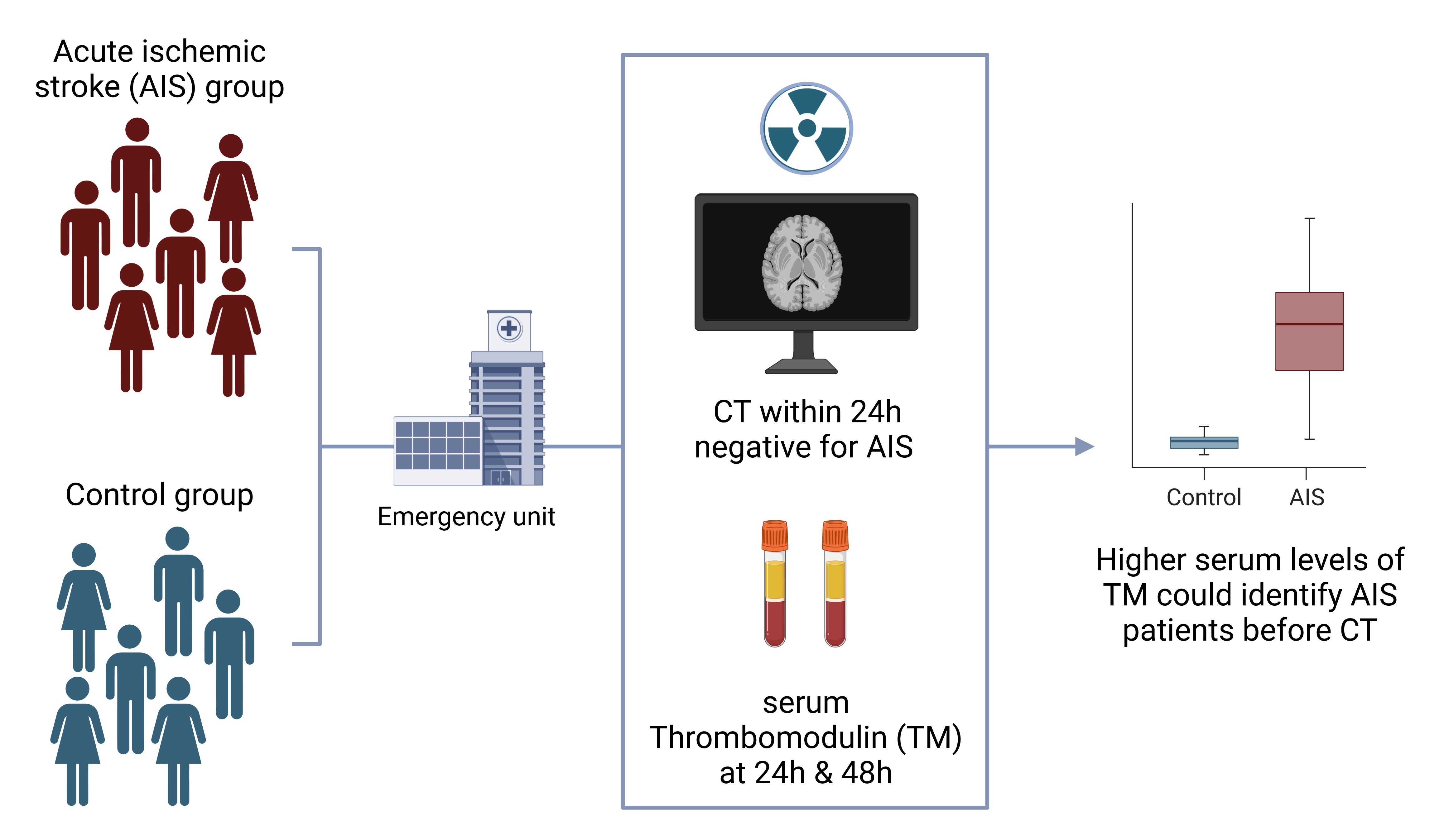
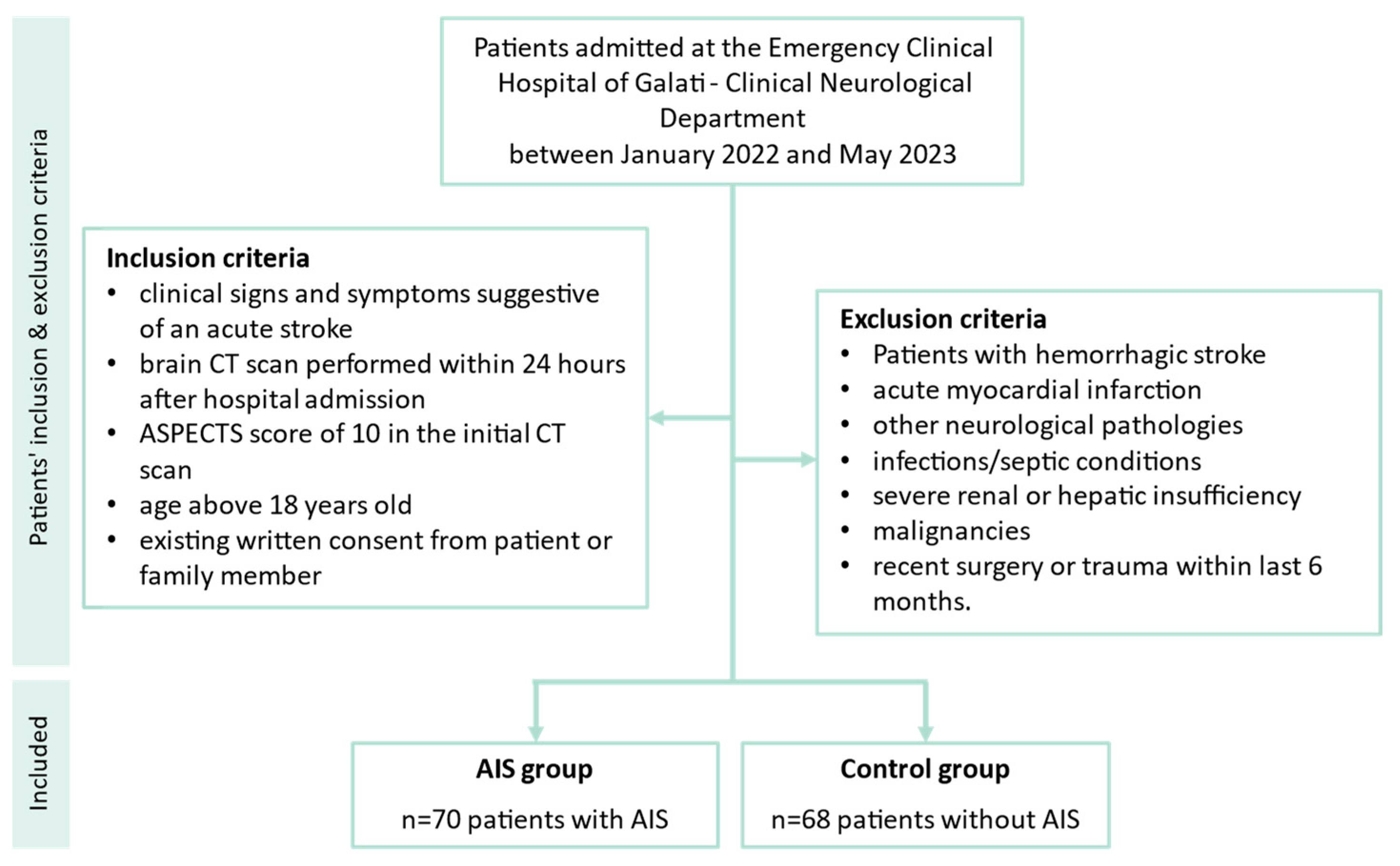
2.1. Study Design and Patients’ Inclusion Criteria
2.2. Blood Work and TM Analysis
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
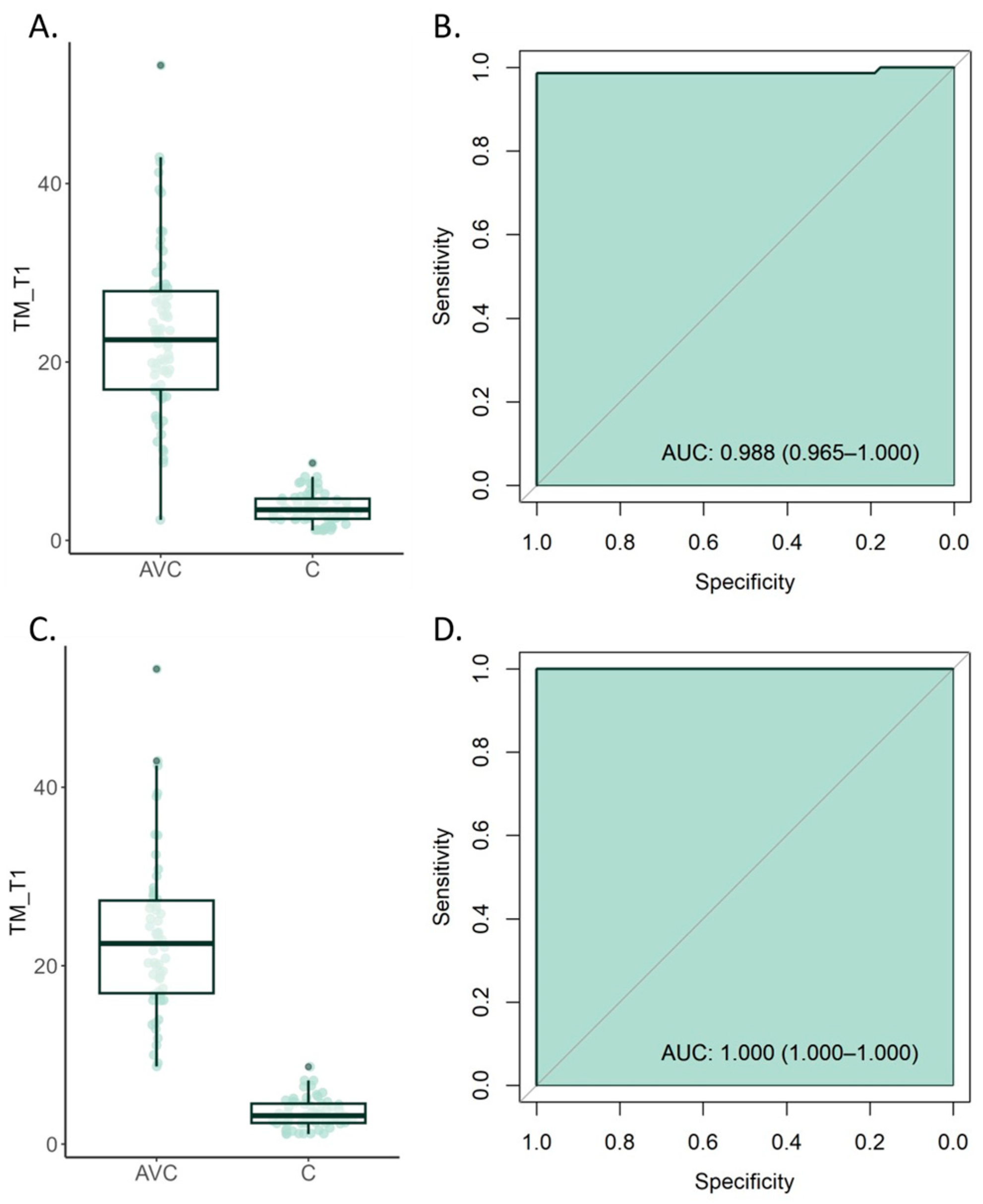
3.2. Serum TM Levels Significantly Increase in Acute Stroke Patients
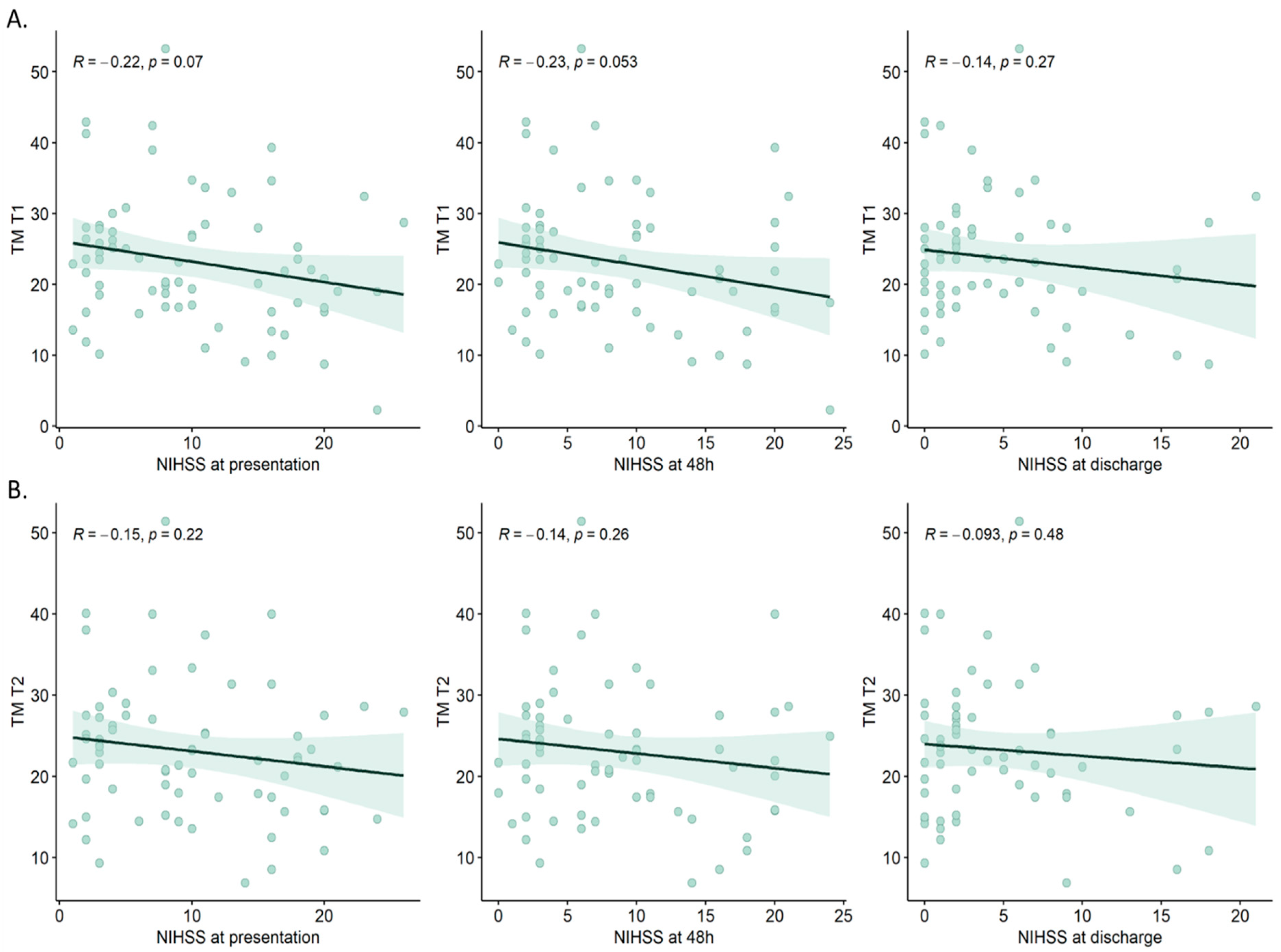
3.3. Serum TM Levels Correlation with Clinical Features in Patients with Developing Stroke
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnston, S.C.; Rothwell, P.M.; Nguyen-Huynh, M.N.; Giles, M.F.; Elkins, J.S.; Bernstein, A.L.; Sidney, S. Validation and Refinement of Scores to Predict Very Early Stroke Risk after Transient Ischaemic Attack. Lancet 2007, 369, 283–292. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.C.; Gress, D.R.; Browner, W.S.; Sidney, S. Short-Term Prognosis after Emergency Department Diagnosis of TIA. JAMA 2000, 284, 2901–2906. [Google Scholar] [CrossRef]
- Lioutas, V.-A.; Ivan, C.S.; Himali, J.J.; Aparicio, H.J.; Leveille, T.; Romero, J.R.; Beiser, A.S.; Seshadri, S. Incidence of Transient Ischemic Attack and Association with Long-Term Risk of Stroke. JAMA 2021, 325, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Prakash, R.; Carmichael, S.T. Blood−brain Barrier Breakdown and Neovascularization Processes after Stroke and Traumatic Brain Injury. Curr. Opin. Neurol. 2015, 28, 556. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, J.; Assmann, J.C.; Schwaninger, M. Thrombomodulin—A New Target for Treating Stroke at the Crossroad of Coagulation and Inflammation. Curr. Med. Chem. 2014, 21, 2025–2034. [Google Scholar] [CrossRef]
- Wu, K.K.; Matijevic-Aleksic, N. Thrombomodulin: A Linker of Coagulation and Fibrinolysis and Predictor of Risk of Arterial Thrombosis. Ann. Med. 2000, 32 (Suppl. 1), 73–77. [Google Scholar]
- Nesheim, M.; Wang, W.; Boffa, M.; Nagashima, M.; Morser, J.; Bajzar, L. Thrombin, Thrombomodulin and TAFI in the Molecular Link between Coagulation and Fibrinolysis. Thromb. Haemost. 1997, 78, 386–391. [Google Scholar] [CrossRef]
- Morser, J. Thrombomodulin Links Coagulation to Inflammation and Immunity. Curr. Drug Targets 2012, 13, 421–431. [Google Scholar] [CrossRef]
- Mosnier, L.O.; Elisen, M.G.; Bouma, B.N.; Meijers, J.C. Protein C Inhibitor Regulates the Thrombin-Thrombomodulin Complex in the up- and down Regulation of TAFI Activation. Thromb. Haemost. 2001, 86, 1057–1064. [Google Scholar] [CrossRef]
- Loghmani, H.; Conway, E.M. Exploring Traditional and Nontraditional Roles for Thrombomodulin. Blood 2018, 132, 148–158. [Google Scholar] [CrossRef]
- Esmon, C.T.; Esmon, N.L.; Harris, K.W. Complex Formation between Thrombin and Thrombomodulin Inhibits Both Thrombin-Catalyzed Fibrin Formation and Factor V Activation. J. Biol. Chem. 1982, 257, 7944–7947. [Google Scholar] [CrossRef] [PubMed]
- Esmon, N.L.; Carroll, R.C.; Esmon, C.T. Thrombomodulin Blocks the Ability of Thrombin to Activate Platelets. J. Biol. Chem. 1983, 258, 12238–12242. [Google Scholar] [CrossRef]
- Keshk, W.A.; Zineldeen, D.H.; El-heneedy, Y.A.; Ghali, A.A. Thrombomodulin, Alarmin Signaling, and Copeptin: Cross-Talk between Obesity and Acute Ischemic Stroke Initiation and Severity in Egyptians. Neurol. Sci. 2018, 39, 1093–1104. [Google Scholar] [CrossRef]
- Wouwer, M.V.D.; Plaisance, S.; Vriese, A.D.; Waelkens, E.; Collen, D.; Persson, J.; Daha, M.R.; Conway, E.M. The Lectin-like Domain of Thrombomodulin Interferes with Complement Activation and Protects against Arthritis. J. Thromb. Haemost. 2006, 4, 1813–1824. [Google Scholar] [CrossRef] [PubMed]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and Reliability of a Quantitative Computed Tomography Score in Predicting Outcome of Hyperacute Stroke before Thrombolytic Therapy. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.r-project.org/ (accessed on 31 October 2023).
- Ho, D.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef]
- Zhu, Z.; Guo, D.; Jia, Y.; Zhang, K.; Shi, M.; Peng, Y.; Yang, P.; Chen, J.; Zhang, J.; Wang, A.; et al. Plasma Thrombomodulin Levels and Ischemic Stroke. Neurology 2022, 99, e916–e924. [Google Scholar] [CrossRef]
- Andreou, A.P.; Crawley, J.T.B. Thrombomodulin Analogues for the Treatment of Ischemic Stroke. J. Thromb. Haemost. 2011, 9, 1171–1173. [Google Scholar] [CrossRef]
- Anderson, L. Candidate-Based Proteomics in the Search for Biomarkers of Cardiovascular Disease. J. Physiol. 2005, 563, 23–60. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Brown, N.J.; Vaughan, D.E.; Harrison, D.G.; Mehta, J.L. Established and Emerging Plasma Biomarkers in the Prediction of First Atherothrombotic Events. Circulation 2004, 109, IV-6–IV-19. [Google Scholar] [CrossRef] [PubMed]
- Olivot, J.-M.; Labreuche, J.; Aiach, M.; Amarenco, P. Soluble Thrombomodulin and Brain Infarction. Stroke 2004, 35, 1946–1951. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, W.; Tseng, M.-C.; Sandercock, P. Blood Biomarkers in the Diagnosis of Ischemic Stroke. Stroke 2008, 39, 2902–2909. [Google Scholar] [CrossRef]
- Dohi, Y.; Ohashi, M.; Sugiyama, M.; Takase, H.; Sato, K.; Ueda, R. Circulating Thrombomodulin Levels Are Related to Latent Progression of Atherosclerosis in Hypertensive Patients. Hypertens. Res. 2003, 26, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Marcovina, S.M.; Crea, F.; Davignon, J.; Kaski, J.C.; Koenig, W.; Landmesser, U.; Pieri, P.L.; Schulz-Menger, J.; Shaw, L.J.; Sobesky, J. Biochemical and Bioimaging Markers for Risk Assessment and Diagnosis in Major Cardiovascular Diseases: A Road to Integration of Complementary Diagnostic Tools. J. Intern. Med. 2007, 261, 214–234. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Tanigami, H.; Suzuki, K.; Shimaoka, M. Thrombomodulin: A Bifunctional Modulator of Inflammation and Coagulation in Sepsis. Crit. Care Res. Pract. 2012, 2012, e614545. [Google Scholar] [CrossRef]
- Yang, L.; Manithody, C.; Walston, T.D.; Cooper, S.T.; Rezaie, A.R. Thrombomodulin Enhances the Reactivity of Thrombin with Protein C Inhibitor by Providing Both a Binding Site for the Serpin and Allosterically Modulating the Activity of Thrombin. J. Biol. Chem. 2003, 278, 37465–37470. [Google Scholar] [CrossRef]
- Preissner, K.T.; Delvos, U.; Mueller-Berghaus, G. Binding of Thrombin to Thrombomodulin Accelerates Inhibition of the Enzyme by Antithrombin III. Evidence for a Heparin-Independent Mechanism. Biochemistry 1987, 26, 2521–2528. [Google Scholar] [CrossRef]
- Castellino, F.J. Human Protein C and Activated Protein C: Components of the Human Anticoagulation System. Trends Cardiovasc. Med. 1995, 5, 55–62. [Google Scholar] [CrossRef]
- Navi, B.B.; Sherman, C.P.; Genova, R.; Mathias, R.; Lansdale, K.N.; LeMoss, N.M.; Wolfe, J.; Skakodub, A.; Kamel, H.; Tagawa, S.T.; et al. Mechanisms of Ischemic Stroke in Patients with Cancer: A Prospective Study. Ann. Neurol. 2021, 90, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Tanne, D.; Macko, R.F.; Lin, Y.; Tilley, B.C.; Levine, S.R. Hemostatic Activation and Outcome after Recombinant Tissue Plasminogen Activator Therapy for Acute Ischemic Stroke. Stroke 2006, 37, 1798–1804. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Group N = 68 | Stroke Group N = 70 | p-Value | |
|---|---|---|---|---|
| Age (years) mean ± SD | 69.28 ± 10.5 | 70.24 ± 10.93 | 0.598 | |
| Gender N (%) | Female | 30 (44.12) | 27 (38.57) | 0.508 |
| Male | 38 (55.88) | 43 (61.43) | ||
| Residential background N (%) | Urban | 36 (52.94) | 46 (65.71) | 0.127 |
| Rural | 32 (47.06) | 24 (34.29) | ||
| Atrial Fibrillation N (%) | No | 51 (75) | 43 (61.43) | 0.087 |
| Yes | 17 (25) | 27 (38.57) | ||
| Dyslipidemia N (%) | No | 34 (50) | 27 (38.57) | 0.177 |
| Yes | 34 (50) | 43 (61.43) | ||
| Diabetes N (%) | No | 41 (60.29) | 55 (78.57) | 0.020 |
| Yes | 27 (39.71) | 15 (21.43) | ||
| Hypertension N (%) | grade 1 | 11 (16.18) | 5 (7.14) | 0.027 |
| grade 2 | 32 (47.06) | 24 (34.29) | ||
| grade 3 | 25 (36.76) | 41 (58.57) | ||
| Chronic Alcohol Use N (%) | No | 47 (69.12) | 60 (85.71) | 0.020 |
| Yes | 21 (30.88) | 10 (14.29) | ||
| Chronic Smoker N (%) | No | 45 (66.18) | 60 (85.71) | 0.007 |
| Yes | 23 (33.82) | 10 (14.29) |
| Variable | N (%)/Mean ± SD | |
|---|---|---|
| Clinical features | ||
| Stroke type N (%) | Cardioembolic | 27 (38.57) |
| Atherothrombotic | 43 (61.43) | |
| Affected vascular territory N (%) | Left middle cerebral artery | 32 (45.71) |
| Right middle cerebral artery | 24 (34.29) | |
| Vertebrobasilar system | 14 (20) | |
| Received thrombolysis | No | 60 (85.72) |
| Yes | 10 (14.28) | |
| Exitus N (%) | No | 62 (88.57) |
| Yes | 8 (11.43) | |
| NIHSS at presentation mean ± SD | 10.07 ± 6.93 | |
| Severity of NIHSS at presentation N (%) | minor (NIHSS = 0–4) | 22 (31.43) |
| moderate (NIHSS = 5–15) | 28 (40) | |
| moderate to severe (NIHSS = 16–20) | 15 (21.43) | |
| severe (NIHSS = 21–42) | 5 (7.14) | |
| NIHSS at 48 h mean ± SD | 8.53 ± 6.67 | |
| Severity of NIHSS at 48 h N (%) | no stroke signs (NIHSS = 0) | 2 (2.86) |
| minor (NIHSS = 0–4) | 26 (37.14) | |
| moderate (NIHSS = 5–15) | 27 (38.57) | |
| moderate to severe (NIHSS = 16–20) | 12 (17.14) | |
| severe (NIHSS = 21–42) | 3 (4.29) | |
| Severity of NIHSS at discharge N (%) | no stroke signs (NIHSS = 0) | 12 (19.35) |
| minor (NIHSS = 0–4) | 27 (43.55) | |
| moderate (NIHSS = 5–15) | 17 (27.42) | |
| moderate to severe (NIHSS = 16–20) | 5 (8.06) | |
| severe (NIHSS = 21–42) | 1 (1.61) | |
| NIHSS at discharge mean ± SD | 4.69 ± 5.26 | |
| Bloodwork parameters | ||
| LDL Cholesterol (mg/dL) mean ± SD | 108.07 ± 45.83 | |
| HDL Cholesterol (mg/dL) mean ± SD | 47.62 ± 14.49 | |
| Total Cholesterol (mg/dL) mean ± SD | 180.32 ± 58.81 | |
| Triglycerides (mg/dL) mean ± SD | 124.16 ± 77.41 | |
| Total Lipids (mg/dL) mean ± SD | 611.13 ± 183.2 | |
| Hemoglobin (g/dL) mean ± SD | 13.59 ± 1.73 | |
| Thrombocytes (109/L) mean ± SD | 228.17 ± 59.96 | |
| Alanine aminotransferase (ALAT) (U/L) mean ± SD | 28.44 ± 20.19 | |
| Aspartate aminotransaminase (ASAT) (U/L) mean ± SD | 29.56 ± 22.19 | |
| Urea (mg/dL) mean ± SD | 41.13 ± 25.41 | |
| Creatinine (mg/dL) mean ± SD | 1.23 ± 0.68 | |
| Na (mmol/L) mean ± SD | 140.66 ± 3.27 | |
| Cl (mmol/L) mean ± SD | 103.63 ± 12.74 | |
| K (mmol/L) mean ± SD | 4.2 ± 0.52 | |
| AR (mmol/L) mean ± SD | 23.59 ± 3.98 | |
| TM-T1 | Threshold | Specificity | Sensitivity | Accuracy | NPV | PPV |
|---|---|---|---|---|---|---|
| All cases | 8.69 | 1 | 0.986 | 0.993 | 0.986 | 1 |
| After propensity matching | 1 | 1 | 1 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaharia, A.-L.; Tutunaru, D.; Oprea, V.D.; Tănase, C.E.; Croitoru, A.; Stan, B.; Voinescu, D.C.; Ionescu, A.-M.; Coadǎ, C.A.; Lungu, M. Thrombomodulin Serum Levels—A Predictable Biomarker for the Acute Onset of Ischemic Stroke. Curr. Issues Mol. Biol. 2024, 46, 677-688. https://doi.org/10.3390/cimb46010044
Zaharia A-L, Tutunaru D, Oprea VD, Tănase CE, Croitoru A, Stan B, Voinescu DC, Ionescu A-M, Coadǎ CA, Lungu M. Thrombomodulin Serum Levels—A Predictable Biomarker for the Acute Onset of Ischemic Stroke. Current Issues in Molecular Biology. 2024; 46(1):677-688. https://doi.org/10.3390/cimb46010044
Chicago/Turabian StyleZaharia, Andrei-Lucian, Dana Tutunaru, Violeta Diana Oprea, Claudiu Elisei Tănase, Ana Croitoru, Bianca Stan, Doina Carina Voinescu, Ana-Maria Ionescu, Camelia Alexandra Coadǎ, and Mihaiela Lungu. 2024. "Thrombomodulin Serum Levels—A Predictable Biomarker for the Acute Onset of Ischemic Stroke" Current Issues in Molecular Biology 46, no. 1: 677-688. https://doi.org/10.3390/cimb46010044